
Awareness of Mueller-Weiss syndrome in flat foot, which is one of the differential diagnoses of flat foot and can be treated conservatively, if treated early.
Dr. Prasamsha Sitaula, Department of Orthopedics Surgery, Nepal Medical College and Teaching Hospital, Gokarneshwar, Nepal. E-mail: sitaulaprasamsha@gmail.com
Introduction: There are numerous causes of flatfoot, among them osteonecrosis of the navicular bone, a rare disease known as Mueller-Weiss syndrome, also leads to deformity
Case Report: A 53-year-old male presented to our Outpatient Department with pain and swelling over bilateral foot for 3 years with increased severity in the left. Physical examination as well as footprint revealed a bilateral flat foot, and there was tenderness as well as swelling over the dorsomedial aspect of bilateral foot. After a detailed physical examination and radiological assessment, the case was diagnosed as Mueller-Weiss syndrome. He was treated with non-steroidal anti-inflammatory drugs, custom ankle-foot orthotic brace for 6 weeks, and activity modification and symptoms were relieved and he was able to do daily activities without any discomfort.
Conclusion: MW syndrome is a rare condition, where conservative treatment provides better results if it is diagnosed and treated early, whereas late cases require surgical intervention.
Keywords: Flat foot, Mueller-Weiss syndrome, Osteonecrosis of navicular bone.
Progressive collapsing foot deformity (Flatfoot) is a complex pathology defined by the collapse of the medial longitudinal arch of the foot with continued progressive deformity of foot and ankle. It may start with only mild symptoms but can progress to a painful, debilitating, and dysfunctional flatfoot [1]. There are numerous causes of flatfoot, among them osteonecrosis of the navicular bone, a rare disease known as Mueller-Weiss syndrome, also leads to deformity [2]. Mueller-Weiss syndrome is a rare idiopathic degenerative disease of the adult where there is progressive collapse and fragmentation of navicular bone leading to mid and hindfoot pain and deformity [3]. It is characterized by navicular compression and fragmentation between talar head and lateral cuneiform with talar head displaced laterally, causing hindfoot varus and flattened medial plantar arch leading to chronic dorsomedial midfoot pain on weight-bearing [4]. Radiologically, there will be decreased navicular size, a comma-shaped configuration, increased radiodensity, fragmentation, and medial or dorsomedial protrusion [5]. Initially, conservative management consists of non-steroidal anti-inflammatory drugs (NSAID) and activity modification with insoles, orthosis, and non-weight bearing cast. When prolonged conservative treatment is not relieving pain, surgery is indicated but it must depend upon severity of symptoms rather than deformity [3]. Surgical intervention options include decompression and autologous bone grafting and talonavicular-cuneiform or Triple arthrodesis [6,7].
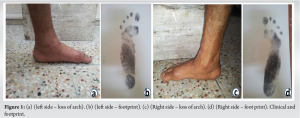
A 53–year-old male presented to our Outpatient Department with pain and swelling over bilateral foot for 3 years with increased severity in the left. The pain was dull aching and insidious in onset that exacerbated with weight-bearing activities. He gave no history of trauma, fever, weight loss, morning stiffness, and other joint pain. Physical examination as well as footprint (Fig. 1a, b, c, and d) revealed bilateral flat foot and there was tenderness as well as swelling over the dorsomedial aspect of bilateral foot. The ankle and subtalar movement were within normal ranges and neurovascular status was normal in both feet.
The weight-bearing plain radiograph revealed decreased size of the navicular, a comma-shaped configuration, increased radiodensity, collapse of the lateral aspect of bone, and dorsomedial protrusion (Fig. 2a, b, c, and d).

The following angles were measured on X-ray: Calcaneal inclination, Meary’s angle, Talonavicular angle, and Talo Calcaneal Angle, showing abnormal value (Table 1).

After a detailed physical examination and radiological assessment, the case was diagnosed as Mueller-Weiss syndrome. Conservative and surgical options were explained, and patients denied surgical intervention. He was treated with NSAID, a custom ankle-foot orthotic brace for 6 weeks, and activity modification. The patient’s symptoms were relieved and he was able to do daily activities without any discomfort.
Mueller-Weiss syndrome, spontaneous osteonecrosis of the tarsal navicular bone in adults, is an uncommon with the number of causes has been speculative, including Kohlers disease, primary osteonecrosis, biomechanical or traumatic causes, and navicular osteoarthritis [3]. Bilateral distribution of spontaneous osteonecrosis with less severe radiographic changes is usually seen and unilateral distribution is often associated with other causes [5]. The plantar pressure distribution in patients with Mueller-Weiss syndrome and normal individuals by Hetsroni et al. [8] concluded that Mueller-Weiss syndrome has increased plantar pressure at the midfoot combined with the reduction in toe pressure, which correlates with characterized navicular pathological changes. The radiographic finding is dorsal or dorsal medial protrusion of navicular bone with characteristic comma-shaped deformity due to collapse of the lateral portion of the bone [5]. There is no gold standard treatment for Mueller-Weiss syndrome, as per the available literature, early-diagnosed is best treated with conservative therapy, whereas surgical intervention is considered for failure of conservative therapies. Later on, once symptoms are not relieved then percutaneous decompression of the navicular bone and excision of the bone and arthrodesis [9]. In the present case, patients were having pain and swelling over bilateral feet with X-ray finding, decreased size of the navicular, a comma-shaped configuration, increased radiodensity, collapse of lateral aspect of bone, and dorsomedial protrusion. These findings are consistent with that of Brailsford [4], Haller et al. [5], and Viladot et al. [10] supporting the diagnosis of Mueller-Weiss syndrome. Our patients were treated conservatively and improved in a few months and were able to perform daily activities without any discomfort.
Mueller-Weiss syndrome should be considered in differential diagnosis of flat foot. Mueller-Weiss syndrome is a rare condition, where conservative treatment provides better results if it is diagnosed and treated early, whereas late presentation requires surgical intervention. Although further studies with a large number of case series and long-term follow-up are required to properly assess the best treatment modalities. This article attempts to bring awareness of Mueller-Weiss syndrome in flat foot.
Awareness of Mueller-Weiss syndrome, which is one of the differential diagnosis of flat foot and can be treated conservatively, if treated early.
References
- 1.Deland J. Adult-acquired flatfoot deformity. J Am Acad Orthop Surg 2008;16:399-406. [Google Scholar]
- 2.Bresnahan P. Flatfoot deformity pathogenesis. A trilogy. Clin Podiatr Med Surg 2000;17:505-12. [Google Scholar]
- 3.Maceira E, Rochera R. Muller-Weiss disease: Clinical and biomechanical features. Foot Ankle Clin 2004;9:105-25. [Google Scholar]
- 4.Brailsford JF. Osteochondritis of the adult tarsal navicular. J Bone Joint Surg Am 1939;21:111-20. [Google Scholar]
- 5.Haller J, Sartoris DJ, Resnick D, Pathri M, Berthoty D, Howard B, et al. Spontaneous osteonecrosis of the tarsal navicular in adults: Imaging findings. AJR Am J Roentgenol 1988;151:355-8. [Google Scholar]
- 6.Lieberman JR. Core decompression for osteonecrosis of the hip. Clin Orthop Relat Res 2004;418:29-33. [Google Scholar]
- 7.De Retana PF, Maceira E, Fernandez-Valencia JA, Suso S. Arthrodesis of the talonavicular-cuneiform joints in Muller-Weiss disease. Foot Ankle Clin 2004;9:65-72. [Google Scholar]
- 8.Hetsroni I, Nyska M, Ayalon M. Plantar pressure distribution in patients with Muller-Weiss disease. Foot Ankle Int 2007;28:237-41. [Google Scholar]
- 9.Miltner O, Niedhart C, Piroth W, Weber M, Siebert CH. Transient osteoporosis of the navicular bone in a runner. Arch Orthop Trauma Surg 2003;123:505-8. [Google Scholar]
- 10.Viladot A Sr., Viladot A Jr. Osteochondroses: Aseptic necrosis of the foot. In: Jahss M, editor. Disorders of the Foot and Ankle. 2nd ed., Vol. 1., Ch. 26. Philadelphia, PA: W. B. Saunders; 1991. p. 617-38. [Google Scholar]



