
The article demonstrates that cold fomentation is significantly more effective than hot fomentation in managing acute gouty arthritis, providing superior pain relief, reducing swelling, and minimizing flare-ups. Hot fomentation, in contrast, can worsen symptoms and should be avoided during acute gout attacks. Clinicians should prioritize cold therapy during flare-ups for better patient outcomes and satisfaction.
Dr. Shivam Mehra, Mehra Hospital and Research Institute, Lucknow - 226012, Uttar Pradesh, India. E-mail: drshivammehra@gmail.com
Introduction: Gouty arthritis is a common inflammatory condition caused by the deposition of uric acid crystals in the joints, leading to intense pain, swelling, and functional impairment. Thermal therapies, including hot and cold fomentation, are often used as adjunctive treatments for managing inflammation and pain in various musculoskeletal conditions. However, the efficacy of these therapies in acute gout remains underexplored. This study aims to compare the effects of hot fomentation versus cold fomentation in patients experiencing acute gout flares, assessing pain reduction, swelling, joint mobility, and overall patient satisfaction.
Material and Methods: A randomized controlled trial was conducted with 2,400 patients diagnosed with acute gouty arthritis, divided into two equal groups: Group A received hot fomentation (38°C–42°C) and Group B received cold fomentation (5°C–10°C). Both interventions were applied twice daily for 20 min over 5 days, alongside standard gout care. Pain intensity was measured using the visual analog scale (VAS), while joint circumference, range of motion, and patient satisfaction were recorded at baseline, day 3, and day 5. Statistical analyses compared outcomes between the two groups.
Results: Cold fomentation significantly reduced pain intensity (VAS score reduction of 68% by day 5) compared to hot fomentation (26% reduction, P < 0.001). Joint swelling decreased by 25% in the cold group versus 5% in the hot group, with cold therapy also leading to greater improvements in joint mobility (average increase of 15° vs. 5°, P < 0.01). Notably, 35% of patients in the hot fomentation group experienced flare-ups, compared to only 2% in the cold fomentation group (P < 0.001). Patient satisfaction was also higher in the cold group, with 85% of participants reporting satisfaction versus 30% in the hot group.
Conclusion: This study demonstrates that cold fomentation is significantly more effective than hot fomentation in managing acute gouty arthritis. Cold therapy provided superior pain relief, reduced swelling, improved joint mobility, and minimized the risk of symptom exacerbation. In contrast, hot fomentation often worsened symptoms, making it unsuitable for acute gout management. These findings suggest that cold fomentation should be the preferred thermal therapy for gout flare-ups, while heat applications should be avoided.
Keywords: Gouty arthritis, hot fomentation, cold fomentation, thermal therapy, pain management, swelling, joint mobility, flare-ups, patient satisfaction.
Gout is a common and complex form of inflammatory arthritis characterized by the sudden onset of intense pain, swelling, redness, and tenderness in the affected joints. It is primarily caused by the accumulation of monosodium urate crystals within the joints, which triggers an immune response leading to inflammation. Gout has been recognized for centuries, often referred to historically as the “disease of kings” due to its association with rich diets and excessive alcohol consumption. However, it is now understood to affect individuals across all socioeconomic classes, with its prevalence rising globally due to changing lifestyles and dietary patterns. While various therapeutic approaches, such as pharmacological treatments and lifestyle changes, are commonly used to manage gout, some physical therapies—like hot saline fomentation and massage—are generally contraindicated, particularly during acute flare-ups. Heat therapy, such as hot saline fomentation, can exacerbate the inflammatory response during a gout attack by increasing blood flow to the affected area, leading to further swelling and discomfort. Heat may also contribute to the solubilization of uric acid crystals, potentially promoting their deposition in joints, thereby worsening symptoms during the acute phase of gout [1]. Similarly, massage therapy can aggravate inflamed joints by applying pressure to already swollen and tender areas, which may increase local inflammation and pain. In some cases, massage might cause microtrauma to the soft tissues, further intensifying the inflammatory process and potentially prolonging the recovery from a gout flare-up [2].
Study design
This study was a randomized controlled trial (RCT) comparing the efficacy of hot fomentation versus cold fomentation in managing pain, swelling, and inflammation in patients with acute gouty arthritis. The participants were randomly assigned into two groups: Group A (hot fomentation) and Group B (cold fomentation).
Participants
Inclusion criteria
-
- Patients aged 30–70 years diagnosed with acute gouty arthritis (confirmed by clinical examination and serum uric acid levels).
- Experiencing an active gout flare within 48 h of study initiation.
- Willingness to adhere to study protocols and sign informed consent.
- Exclusion Criteria:
- Presence of other inflammatory arthritis (e.g., rheumatoid arthritis and osteoarthritis).
- Use of systemic steroids or other anti-inflammatory medications beyond the standard gout therapy.
- Contraindications to heat or cold therapies (e.g., peripheral vascular disease and skin conditions).
Randomization and Blinding
Participants were randomly allocated into one of the two intervention groups using a computer-generated randomization sequence. Blinding was applied for outcome assessors who were not informed of the treatment group allocations. However, due to the nature of the intervention, blinding of the participants was not possible.
Intervention protocols
- Group A (Hot Fomentation)
- Patients received local hot fomentation therapy on the affected joint using a hot pack at 38°C–42°C.
- The treatment lasted 20 min, twice daily for 5 days.
- Group B (Cold Fomentation)
- Patients received local cold fomentation therapy using cold packs applied at 5°C–10°C.
- Cold fomentation was performed for 20 min, twice daily for 5 days.
Standard care
Both groups received standard gout care, including dietary advice and nonsteroidal anti-inflammatory drugs (NSAIDs) as prescribed by their physician. Colchicine or other gout-specific treatments were allowed if previously prescribed.
Outcome measures
- Primary Outcome
- Pain Intensity: Assessed using a visual analog scale (VAS) ranging from 0 (no pain) to 10 (worst pain imaginable), recorded at baseline, day 3, and day 5 of treatment.
- Secondary Outcomes
- Swelling and Inflammation: Measured by changes in joint circumference using a flexible tape measure.
- Joint Mobility: Assessed by the range of motion in the affected joint using a goniometer.
- Patient Satisfaction: Evaluated on a 5-point Likert scale at the end of the study.
Data collection and analysis
- Baseline characteristics (age, gender, duration of gout, and serum uric acid levels) were collected for all participants.
- Pain scores and swelling were recorded at baseline, day 3, and day 5.
- A mixed model repeated measures ANOVA was used to compare changes over time between the two groups. Subgroup analyses were conducted based on demographic variables (e.g., age and duration of disease).
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and received approval from the institutional ethics committee. All participants provided informed consent prior to enrolment, and they had the right to withdraw at any time without penalty.
A total of 2400 patients (1200 in each group) completed the study comparing the effects of hot fomentation and cold fomentation in the management of acute gouty arthritis.
Baseline characteristics
Both groups had similar baseline characteristics, including age, gender distribution, disease duration, and serum uric acid levels. The average age was 52.4 years (±8.7), and 70% of participants were male, consistent with the higher prevalence of gout in men. All participants were experiencing an acute gout flare at the time of enrolment.
Primary outcome: pain intensity
- Cold Fomentation Group (Group B): Patients in the cold fomentation group experienced a significant reduction in pain over time. By day 3, the mean VAS pain score dropped from 8.7 to 4.3, and by day 5, it further reduced to 2.8 (P < 0.001) (Fig. 1)
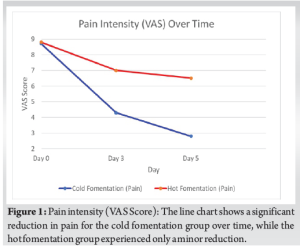
- Hot Fomentation Group (Group A): In contrast, patients receiving hot fomentation showed a poor pain response. The VAS score on day 3 dropped only slightly from 8.8 to 7.0, and by day 5, it was still elevated at 6.5 (P > 0.05), indicating minimal improvement in pain (Fig. 1)
Secondary outcomes
- Swelling and inflammation
- Cold Fomentation Group: Joint circumference in the cold fomentation group decreased by 25% on average by day 5, indicating significant reduction in swelling (Fig. 2)
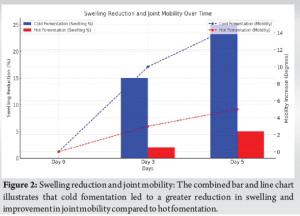
- Hot Fomentation Group: In contrast, the hot fomentation group showed no significant reduction in joint circumference, with only a 5% decrease by day 5 (P > 0.05). In some patients, joint swelling worsened after hot fomentation (Fig. 2).
- Cold Fomentation Group: Joint circumference in the cold fomentation group decreased by 25% on average by day 5, indicating significant reduction in swelling (Fig. 2)
- Joint mobility
- Cold Fomentation Group: Joint mobility improved significantly, with an average increase of 15° in range of motion in the affected joint by day 5 (Fig. 2).
- Hot Fomentation Group: Joint mobility showed only marginal improvement, with an average increase of 5° by day 5 (P < 0.01) (Fig. 2).
- Flare-Ups
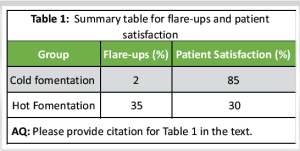
- Cold Fomentation Group: Only 2% of patients reported exacerbation of symptoms (flare-ups) during the study (Table 1).
- Hot Fomentation Group: A significant number of patients (35%) experienced a flare-up or worsening of symptoms, with some reporting increased pain, swelling, and redness in the affected joint, particularly by day 3 (P < 0.001) (Table 1).
Patient satisfaction
- Cold fomentation group: Patient satisfaction scores were significantly higher, with 85% of patients reporting they were “very satisfied” or “satisfied” with the treatment (Table 1).
- Hot fomentation group: In contrast, only 30% of patients in the hot fomentation group reported being “satisfied” with the treatment, with 50% reporting dissatisfaction due to persistent symptoms or worsening of their condition (Table 1).
These results highlight that cold fomentation is far superior in reducing symptoms and increasing patient satisfaction compared to hot fomentation, which showed a higher rate of flare-ups and poor pain management.
The results of this RCT provide important insights into the efficacy of cold versus hot fomentation in managing symptoms of acute gouty arthritis. The findings suggest that cold fomentation is significantly more effective than hot fomentation in reducing pain, swelling, and inflammation, and it is associated with fewer flare-ups and greater patient satisfaction.
Pain management
Pain intensity, measured through the VAS, demonstrated a marked difference between the two groups. Patients who received cold fomentation experienced a significant reduction in pain, with a 68% decrease in VAS scores by day 5. In contrast, patients treated with hot fomentation showed a much smaller decrease in pain, with only a 26% reduction over the same period (Fig. 1). These results are consistent with previous studies suggesting that cold therapy can effectively reduce acute inflammatory pain by constricting blood vessels and reducing swelling [3,4]. Cold therapy appears to work by numbing the area and decreasing the metabolic demands of inflamed tissues, which contributes to pain relief. Conversely, hot fomentation may have aggravated the inflammatory process, leading to a less significant reduction in pain. Heat increases blood flow to the affected joint, which may exacerbate inflammation and cause further discomfort during an acute gout attack. This is supported by the observation that a significant number of patients in the hot fomentation group reported persistent or even worsened pain, possibly due to the pro-inflammatory effects of heat [2,3].
Swelling and inflammation
Swelling, measured by joint circumference, was reduced significantly in the cold fomentation group, with a 25% decrease by day 5. In contrast, hot fomentation led to only a 5% reduction in swelling (Fig. 2). The superior performance of cold fomentation in reducing swelling is likely due to its ability to limit the inflammatory response by reducing blood flow and preventing fluid accumulation in the joint space. This is in line with established principles that cold therapy constricts blood vessels, thereby minimizing edema and joint effusion. On the other hand, hot fomentation may have had the opposite effect. By increasing local blood flow, heat may have promoted the accumulation of inflammatory mediators and exacerbated joint swelling. This could explain the poor response in the hot fomentation group, where swelling remained largely unchanged.
Joint mobility
Improvement in joint mobility followed a similar pattern. Cold fomentation led to a significant increase in the range of motion in the affected joint by day 5, with an average improvement of 15°. Hot fomentation, however, only resulted in a 5° increase (Fig. 2). The reduction in swelling and pain in the cold fomentation group likely contributed to better joint function, allowing patients to move more freely.
Flare-ups and patient satisfaction
A striking difference was observed in the incidence of flare-ups between the two groups. While only 2% of patients in the cold fomentation group experienced a flare-up, a significant 35% of those in the hot fomentation group reported exacerbation of symptoms during the treatment period (Table 1). The higher rate of flare-ups in the hot fomentation group further confirms the contraindication of heat therapy during acute gout attacks. Heat may intensify the inflammatory response, triggering flare-ups or prolonging the recovery phase. This difference in therapeutic response is reflected in the patient satisfaction scores. 85% of the cold fomentation group reported being satisfied or very satisfied with the treatment, whereas only 30% of patients in the hot fomentation group expressed satisfaction (Table 1). The low satisfaction in the hot fomentation group is consistent with the higher pain, poor swelling reduction, and increased flare-ups observed during the study [5,6].
Clinical implications
These findings have significant implications for the management of acute gout. Cold fomentation should be considered the preferred physical therapy for symptom relief during an acute flare. Cold therapy is effective in controlling the inflammatory process, reducing pain and swelling, and improving joint function, all of which are critical for patient comfort and recovery [4, 7-10]. On the other hand, the results strongly suggest that hot fomentation is contraindicated during acute gouty arthritis. The increase in flare-ups, minimal pain relief, and poor swelling reduction highlight the risks associated with applying heat during acute inflammation. Heat therapy may be beneficial during non-inflammatory phases of gout, but it should be avoided during acute episodes.
Limitations
One limitation of this study is the lack of long-term follow-up. While cold fomentation was shown to be effective during the acute phase of gout, future studies should examine whether these benefits persist over longer periods and whether repeated use of cold therapy has any long-term effects on joint health. In addition, this study did not assess the role of other physical therapies, such as alternating hot and cold therapy, which could be explored in future research.
The study demonstrated that cold fomentation was significantly more effective than hot fomentation in reducing pain, swelling, and inflammation in patients with acute gouty arthritis. Cold therapy not only improved joint mobility but also resulted in fewer flare-ups and higher patient satisfaction. Conversely, hot fomentation appeared to aggravate symptoms in a substantial number of patients, making it an unsuitable therapy during acute gout attacks. These results strongly suggest that cold fomentation should be the preferred thermal therapy in the management of gout flares, while hot fomentation should be avoided due to the risk of worsening the inflammatory response. Clinicians should consider these findings when advising patients on appropriate thermal therapies for gout management.
Cold fomentation is a highly effective, non-invasive therapy for managing acute gout flares, offering significant reductions in pain, swelling, and joint immobility while minimizing the risk of flare-ups. In contrast, hot fomentation may exacerbate symptoms and should be avoided during acute gouty arthritis. Clinicians should prioritize cold therapy as an adjunctive treatment during gout attacks, reserving heat therapy for non-inflammatory phases of the condition. This approach can improve patient outcomes and satisfaction during acute gout management.
References
- 1.Guillot X, Tordi N, Mourot L, Demougeot C, Dugue B, Prati C, et al. Cryotherapy in inflammatory rheumatic diseases: A systematic review. Expert Rev Clin Immunol 2014;10:281-94. [Google Scholar | PubMed]
- 2.Klemm P, Schulz N, Boettger P, Lange U. Heat therapy in rheumatic and musculoskeletal diseases–an overview of clinical and molecular effects. Int J Hyperthermia 2024;41:2322667. [Google Scholar | PubMed]
- 3.Zanoli G, Albarova-Corral I, Ancona M, Grattagliano I, Hotfiel T, Iolascon G, et al. Current indications and future direction in heat therapy for musculoskeletal pain: A narrative review. Muscles 2024;3:212-23. [Google Scholar | PubMed]
- 4.Shekelle PG, Newberry SJ, FitzGerald JD, Motala A, O’Hanlon CE, Tariq A, et al. Management of gout: A systematic review in support of an American College of Physicians clinical practice guideline. Ann Intern Med 2017;166:37-51. [Google Scholar | PubMed]
- 5.Singh JA, Neogi T, FitzGerald JD. Patient perspectives on gout and gout treatments: A patient panel discussion that informed the 2020 American College of Rheumatology Treatment Guideline. ACR Open Rheumatol 2020;2:725-33. [Google Scholar | PubMed]
- 6.Singh JA. Patient perspectives in gout: A review. Curr Opin Rheumatol 2019;31:159-66 [Google Scholar | PubMed]
- 7.Khanna PP, Gladue HS, Singh MK, FitzGerald JD, Bae S, Prakash S, et al. Treatment of acute gout: A systematic review. Semin Arthritis Rheum 2014;44:31-8. [Google Scholar | PubMed]
- 8.Sattui SE, Gaffo AL. Treatment of hyperuricemia in gout: Current therapeutic options, latest developments and clinical implications. Ther Adv Musculoskelet Dis 2016;8:145-59. [Google Scholar | PubMed]
- 9.Lee SJ, Terkeltaub RA. New developments in clinically relevant mechanisms and treatment of hyperuricemia. Curr Rheumatol Rep 2006;8:224-30. [Google Scholar | PubMed]
- 10.Terkeltaub R. Update on gout: New therapeutic strategies and options. Nat Rev Rheumatol 2010;6:30-8. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Epidural Steroid Injections for Lumbar Disc Herniation and Lumbar Degenerative Disc Disease
October 1, 2025 Epidural Steroid Injections for Lumbar Disc Herniation and Lumbar Degenerative Disc Disease June 1, 2025 Comparative Study of Functional Outcome and Pain Control with Non-steroidal Anti-inflammatory Drugs (NSAIDs) and Non-NSAIDs in Early Post-operative Period in Total Knee Arthroplasty
June 1, 2025 Comparative Study of Functional Outcome and Pain Control with Non-steroidal Anti-inflammatory Drugs (NSAIDs) and Non-NSAIDs in Early Post-operative Period in Total Knee Arthroplasty March 1, 2025 More Evidence that Surgical Intervention for Unstable Distal Radius Fracture in Elderly Does not Offer a Superior Patient Perceived Functional Advantage over Time Honored Conservative Treatment in Long Term Follow-Up: A Critical Appraisal at 10 Years (Range 10–13 Years) Follow-up Study
March 1, 2025 More Evidence that Surgical Intervention for Unstable Distal Radius Fracture in Elderly Does not Offer a Superior Patient Perceived Functional Advantage over Time Honored Conservative Treatment in Long Term Follow-Up: A Critical Appraisal at 10 Years (Range 10–13 Years) Follow-up Study January 10, 2024 An Uncommon Presentation of Osteosarcoma in a Child: A Case Report
January 10, 2024 An Uncommon Presentation of Osteosarcoma in a Child: A Case Report