
The osteochondromas are uncommon in flat bones but can still manifest at any site.
Dr. Karthik Loganathan, Assistant Professor, Department of Orthopedics, Government Stanley Medical College, Chennai, Tamil Nadu, India. E-mail: karindu1989@gmail.Com
Introduction: Osteochondroma is a bony lesion arising from the surface of the bone. It com-prises a large percentage of all benign bone tumors. A unique feature of this tumor is the conti-nuity of cortical and medullary components between the normal bony tissue and aberrant tissue of osteochondroma. Even though the predominant composition is bone, growth takes place in the cartilaginous portion. The incidence of osteochondroma in flat bones which are ossified by intramembranous type of ossification including the scapula, clavicle, ribs, and pubic ramus is usually rare.
Case Report: We report three cases of osteochondroma involving less common and unusual sites. We have included one case of osteochondroma of the medial end of the clavicle, one case of iliac wing osteochondroma, and one case of radial head osteochondroma.
Conclusion: Osteochondroma rarely occurs in unusual sites. Although uncommon, osteochon-droma can involve small and flat bones.
Keywords: Osteochondroma, exostosis, clavicle, iliac wing, proximal radius.
Osteochondroma is a bony outgrowth surrounded by a cartilage layer and involves long bones around the knee and elbow. [1]. It is usually diagnosed before the third decade of life particularly around the knee joint and proximal humerus. The flat bones which are ossified by intramembranous type of ossification including the scapula, clavicle, ribs, and pubic ramus are less commonly involved. Whether osteochondroma is a tumor or a developmental condition is still up for debate. Osteochondromas are bony projections that form on the outside of bones and are covered in cartilage, [2]. Although bone makes up the majority of the composition, the cartilaginous region is where growth occurs.
In our study, we report three cases of solitary osteochondromas occurring at rare sites, varied clinical presentation, and their management.
Case 1: Medial end of clavicle
A 16-year-old female patient presented to our orthopedic clinic at Government Stanley Hospital with swelling in the anterior aspect of the neck. Over the previous 6 months, it was seen that the edema was getting bigger. Other than the cosmetic appearance, the patient did not have any other symptoms. Upon examination, the swelling on the front aspect of the left clavicle’s medial end was discovered to be hard and inflexible. On X-ray chest PA view and X-ray left shoulder, the lesion is located at the anteromedial aspect of the left clavicle. We ordered for a computed tomography which suggested a bony lesion of size 1 × 0.8 × 0.9 cm suggestive of an osteochondroma. An MRI of the same lesion was done which also suggested a solitary osteochondroma of the clavicle. The diagnosis and the necessity of excision surgery followed by biopsy were explained to the patient and consent was obtained (Fig. 1).
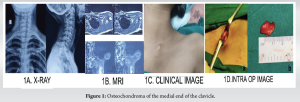
Osteochondroma excision was done under general anesthesia. On the left side of the neck, directly lateral to the sternoclavicular joint, a linear skin incision was performed over the bony prominence along the Langerhans line. A longitudinal separation of the strap muscles revealed the bony protrusion. Following electrocautery to delineate the base, an osteotome was used to perform the osteotomy of the osteochondroma. Gel foam was used to establish hemostasis at the excision site. The excised mass a brown bony tissue measuring 1 × 0.9 × 1 cm was sent for histopathological examination. The pathology report was consistent with osteochondroma. The patient was reviewed regularly for a period of 6 months with no further complaints.
Case 2: Solitary osteochondroma of Radial head
A 16-year-old female presented to orthopedics OPD in Government Stanley Medical College and Hospital with complaints of progressive swelling over the left elbow region for the past 5 years associated with pain over the elbow joint. The patient was examined and on palpation, a non-tender, hard mass was located over the anterolateral aspect of the elbow. It was non-reducible, non-compressible, and fixed to the underlying bone. Terminal flexion and rotational movements of the elbow were restricted. On investigation, a plain X-ray of the elbow showed exostosis in the proximal radius metaphysis. CT and MRI were taken, which showed a 3 × 4 × 2.4 cm size swelling arising from the proximal metaphyseal region of the radius with a cartilaginous cap of 2.4 mm (Fig. 2).
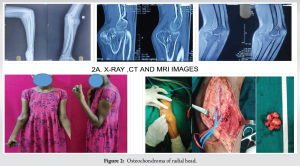
After doing thorough pre-operative evaluation, the patient was taken up for surgery. Under the supraclavicular block, the incision was made and superficial dissection was done. Since the brachial artery was in close proximity to the tumor, vascular surgeon assistance was obtained to isolate the brachial artery. Marginal excision of the exostosis was done. The intraoperative and post-operative periods were uneventful. Confirmatory post-operative radiographs were taken.
Case 3: Iliac wing osteochondroma
An 18-year-old male presented to the outpatient department in Government Stanley Medical College Hospital with complaints of progressive swelling over the left iliac region for the past 5 years associated with pain while sitting and sleeping in a decubitus position. The patient was examined. On palpation, a tender hard mass was located poster superior to the left anterior superior iliac spine (ASIS) of the iliac bone. The skin over the swelling was free and mobile. On investigation, a plain X-ray pelvis showed exostosis in the iliac bone. MRI was taken and it showed a swelling of size 8.1 × 5.3 × 6.1 cm present in the left iliac bone with irregular cartilaginous cap thus confirming our diagnosis (Fig. 3).

With the patient in the right lateral position, a skin incision was made from the left side ASIS to the left side posterior superior iliac spine (PSIS). The site was dissected in layers and then the tumor mass was identified. In extra periosteal manner, tumor excision was done along with a pedunculated stalk. The specimen was sent for histopathological examination. Post-operative X-ray showed complete excision of the tumor mass. The patient mobilized on immediately post-operative. Suture removal was done on POD 14th. At 6 months follow up the patient is mobilizing without pain and no recurrence of tumor.
Osteochondromas are benign tumors that are typically discovered by accident and are asymptomatic. These are the most prevalent kinds of benign bone tumors, appearing on the external surface of bones. The metaphyseal area of long bones is where they are most frequently found. It is more prevalent around the knee joint and more common in the proximal humerus after the third decade [3,4]. A small masculine preponderance has been noted in certain research studies. The clavicle, scapula, ribs, pubic ramus, and iliac wing – flat bones that are typically ossified by intramembranous type of ossification during the fetal period – are less frequently implicated [5,6]. There is controversy regarding the genesis of osteochondroma. They are described as either real neoplasms that may result from cell separation in the epiphyseal plate, or as developmental lesions in certain studies. Numerous investigations have documented the emergence of osteochondroma following radiation therapy or trauma [7]. Osteochondroma is a true neoplastic lesion, as evidenced by numerous research that indicate genetic alterations in both solitary and hereditary varieties [8]. Osteochondroma manifests clinically in two different ways: as a single lesion known as solitary osteochondroma, or as several lesions known as multiple osteochondroma. It is called a pedunculated type of tumor if it has a stalk or stems protruding from the normal bone. The tumor expansion is referred to as sessile type if it has a wider base attached to the bone. Large, sessile osteochondromas with a thick cartilage covering are typical of multiple hereditary osteochondromas. Solitary osteochondroma is commonly known as exostosis. Most isolated osteochondroma is discovered accidentally and is asymptomatic. The location and size of the exostosis are frequently associated with symptoms in patients. They cease when skeletal maturity is attained, growing gradually and slowly alongside the affected bone. Greater intensity of pain may be brought on by edema, a pathological fracture, or related nerve compression. Osteochondroma malignant transformation is extremely uncommon, occurring in approximately 1% of isolated tumors. In contrast, the frequency of malignant transformation in cases with multiple exostosis is approximately 10% [9]. New-onset discomfort, irregular calcification, growth beyond skeletal maturity, irregular borders, and erosion of surrounding bone are indicators of malignant change [8]. Another predictor is the thickness of the cartilage cap; in adults, a cap thickness of more than 2 cm, and in teenagers, a thickness of 3 cm is predictive of malignancy [9,10]. The majority of clavicle-related cases, according to our review of the literature, occur toward the lateral end of the clavicle [11,12]. Osteochondroma of the medial/proximal end of the clavicle is very rare [13,14]. Some of the manifestations reported in the literature for this type of lesion are Horner syndrome [15,16], tendinopathy [12], subclavian thrombosis [17], brachial plexopathy [18], and impingement syndrome [11]. In one of our cases, the patient presented with an osteochondroma of the medial end but without any symptoms except for cosmetic deformity. In our second case involving the iliac wing, the lack of major symptoms allowed the osteochondroma to grow unnoticed until it became evident from its mass effect. When these secondary effects become noticed, they can present in multiple ways interfering in day-to-day activities. A pelvic tumor can grow to the extent that it can even cause sexual dysfunction [19]. In our third case involving the proximal radius, the main symptom was swelling, pain, and restriction of movements. Only five cases of osteochondroma involving the proximal radius were reported in the literature with one particular case presenting with radial head dislocation [20]. Another one case presented with impingement of the posterior interosseous nerve with symptoms resembling radial tunnel syndrome [21]. The treatment for these isolated lesions that did not reveal anything concerning during the first imaging is to perform routine, straightforward follow-ups. After surgical excision, there is a 1–2% chance of recurrence. For a single osteochondroma, the prognosis is usually better than that of multiple osteochondromas.
Osteochondroma is a benign lesion that usually presents without any symptoms. The incidence of osteochondroma in flat bones in particular is rare and often has unusual symptoms. The presenting symptoms can be attributed to mechanical block at the presenting site, which may vary across different locations. Excision of the lesion is a curative form of treatment without any recurrence. However, the surgical technique must be precise as the involvement in unusual sites may pose a risk to neurovascular structures. Regular follow-up is important to prevent any recurrence or malignant transformation. Hence, we would like to conclude that though unusual, osteochondroma can still involve small and flat bones.
Although osteochondroma is rare in unusual sites, it is important to evaluate all patients presenting with swelling and pain over bony regions to diagnose and manage accordingly.
References
- 1.Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of oste-ochondroma: Variants and complications with radiologic-pathologic correlation. Radi-ographics 2000;20:1407-34. [Google Scholar | PubMed]
- 2.World Health Organization. The WHO Manual of Diagnostic Imaging: Radiographic Anatomy and Interpretation of the Musculoskeletal System. Available from: https://www.who.int/publications/i/item/9241545550 [Last accessed on 2024 Sep 04]. [Google Scholar | PubMed]
- 3.Differential Diagnosis in Orthopaedic Oncology. Available from: https://www.wolterskluwer.com/en/solutions/ovid/differential-diagnosis-in-orthopaedic-oncology-3530 [Last accessed on 2024 Sep 04]. [Google Scholar | PubMed]
- 4.Atik OS, Sarikaya B, Kunat C, Muradi R, Ocaktan B, Topçu H. Osteochondroma of the talus. Eklem Hastalik Cerrahisi 2010;21:116-7. [Google Scholar | PubMed]
- 5.Priemel MH, Stiel N, Zustin J, Luebke AM, Schlickewei C, Spiro AS. Bone tumours of the clavicle: Histopathological, anatomical and epidemiological analysis of 113 cases. J Bone Oncol 2019;16:100229. [Google Scholar | PubMed]
- 6.Gökkuş K, Aydın AT, Sağtaş E. Solitary osteochondroma of ischial ramus causing sciat-ic nerve compression. Eklem Hastalik Cerrahisi 2013;24:49-52. [Google Scholar | PubMed]
- 7.Taitz J, Cohn RJ, White L, Russell SJ, Vowels MR. Osteochondroma after total body ir-radiation: An age-related complication. Pediatr Blood Cancer 2004;42:225-9. [Google Scholar | PubMed]
- 8.Beltrami G, Ristori G, Scoccianti G, Tamburini A, Capanna R. Hereditary multiple ex-ostoses: A review of clinical appearance and metabolic pattern. Clin Cases Miner Bone Metab 2016;13:110-8. [Google Scholar | PubMed]
- 9.Tepelenis K, Papathanakos G, Kitsouli A, Troupis T, Barbouti A, Vlachos K, et al. Os-teochondromas: An updated review of epidemiology, pathogenesis, clinical presenta-tion, radiological features and treatment options. In Vivo 2021;35:681-91. [Google Scholar | PubMed]
- 10.Brien EW, Mirra JM, Luck JV Jr. Benign and malignant cartilage tumors of bone and joint: Their anatomic and theoretical basis with an emphasis on radiology, pathology and clinical biology. II. Juxtacortical cartilage tumors. Skeletal Radiol 1999;28:1-20. [Google Scholar | PubMed]
- 11.Çıtlak A, Akgün U, Bulut T, Aslan C, Mete BD, Şener M. Subacromial osteochondroma: A rare cause of impingement syndrome. Int J Surg Case Rep 2015;6C:126-8. [Google Scholar | PubMed]
- 12.Galanopoulos I, Stavlas P, Beltsios M. Distal clavicle osteochondroma causing suprasp-inatus tendinopathy. Cureus 2019;11:e4354. [Google Scholar | PubMed]
- 13.Alrawili MH, Aldusari R, Alsayegh S, Al Robian F. Proximal clavicular osteochondro-ma: A report of an unusual site. J Pediatr Surg Case Rep 2021;77:102152. [Google Scholar | PubMed]
- 14.Prabowo Y, Fajrin Armin M, Alhuraiby SS, Canintika AF. Surgical techniques for me-dial clavicular tumors: A report of 3 cases. Int J Surg Case Rep 2023;106:108115. [Google Scholar | PubMed]
- 15.Watura K, Williams M, Bradley M. Osteochondroma of the clavicle causing Horner’s syndrome. BMJ Case Rep 2015;2015:bcr2015211705. [Google Scholar | PubMed]
- 16.Simpson JF. Horner’s syndrome due to an osteochondroma of the first rib. Can Med As-soc J 1948;59:152-5. [Google Scholar | PubMed]
- 17.Cusson DL, King AB. Osteochondroma involving the first rib with neurovascular com-pression. Bull Johns Hopkins Hosp 1961;108:157-60. [Google Scholar | PubMed]
- 18.Mollano AV, Hagy ML, Jones KB, Buckwalter JA. Unusual osteochondroma of the me-dial part of the clavicle causing subclavian vein thrombosis and brachial plexopathy. A case report. J Bone Joint Surg Am 2004;86:2747-50. [Google Scholar | PubMed]
- 19.Thomas C, Sanderson B, Horvath DG, Mouselli M, Hobbs J. An unusual case of solitary osteochondroma of the iliac wing. Case Rep Orthop 2020;2020:8831806. [Google Scholar | PubMed]
- 20.Gupta SV, Raj N. A case report of osteochondroma of radial neck in a young adult. Int J Case Rep Images 2023;14:119-22. [Google Scholar | PubMed]
- 21.Casstevens C, Hubbard J, Abrams R. Impinging exostoses of the proximal radius: A re-port of two cases with distinct clinical features. JSES Rev Rep Tech 2021;1:141-4. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report
November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling
October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling October 1, 2024 Osteochondroma versus Chondrosarcoma a Diagnostic Dilemma – a Case Report
October 1, 2024 Osteochondroma versus Chondrosarcoma a Diagnostic Dilemma – a Case Report August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review
August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review