
Our study shows flexible IM nailing is better than external fixator in the fractures shaft tibia in Gustilo type II, IIIA and IIIB.
Dr. Susheel Kumar Soni, Department of Orthopaedic, LNCT Medical College and Sewakuj Hospital, Kanadia, Indore - 452001, Madhya Pradesh, India. E-mail: drsusheelsoni0@gmail.com
Abstract
Background: Open tibial fractures, usually caused by high-energy trauma, are among the most common long bone fractures. Clinically, the treatment of open tibial fractures remains a major therapeutic problem for surgeons because of the poor soft tissue coverage and blood supply in the tibia, with resultant difficulties arising from infection and poor bone healing. In this study we will assess the results of intramedullary flexible nailing and external fixator in the management of fractures shaft tibia (G.A. type II, IIIA and IIIB)
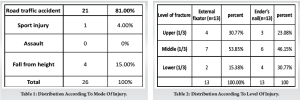
Material & Methods: Twenty six patients who presented with open fractures of the tibial shaft type II, IIIA, and IIIB (Gustilo) were treated. We included the patients of both sexes, age between 18-65 years with diaphysial fractures 5cm distal to the tibial tuberosity and at least 5 cm proximal to the tibial plafond, irrespective of fibula fracture. Thirteen patients were treated by external fixator and Thirteen patients by flexible intramedullary nailing and the outcome were assessed.
Results: Mean age in our study was 36 years for flexible intramedullary nailing group and 38 years for external fixator group. Male involvement was in 69.23% (18 patients) and female involvement was 30.76% (8 patients). In present study for external fixation mean age was 38 years (25-60) , union rate was 84.4%, non–union rate 16.6% and malunion was 33.3%, Pin track infection rate was 50%., average time of union 27.08 weeks (26-30 weeks) and osteomyelitis is 16.6%. In present study results for flexible intramedullary nailing, the mean age is 36 years (20-62 years), mal-union is 8.3%, pain at nail head rate is 16.6%, average time of union is 25 weeks and Union achieved in all cases.
Conclusion: Flexible intramedullary nailing is more efficacious than external fixator in the management of fractures shaft tibia ( Gustilo type II, IIIA and IIIB). Advantages observed are maintaining limb alignment and fewer serious complication, fewer operation needed, and a better range of motion of adjacent joints obtained. It reduces hospital stay of patients and later patient can return early to work, thus minimizes psychological trauma and financial burden. Flexible intramedullary nailing has easy learing curve. External fixator group had more disability and difficulties in daily routine activity like sleeping, bathing and other social activity.
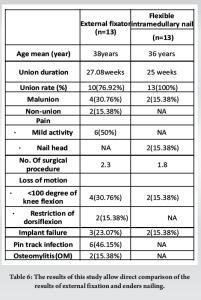
Keywords: G.A.- Gustilo Anderson Classification of Compound fracture , OM- Osteomyelitis , NA – Not Applicable, IM- Intramedullary nail.
Open tibial fractures, usually caused by high-energy trauma, are among the most common long bone fractures . Clinically, the treatment of open tibial fractures remains a major therapeutic problem for surgeons because of the poor soft tissue coverage and blood supply in the tibia, with resultant difficulties arising from infection and poor bone healing [1,2,3]. Both bone instability and disrupted soft tissues are a current focus of all orthopaedic and plastic surgeons. The treatment of open tibia fractures remains controversial. The precarious blood supply and lack of soft-tissue cover of the shaft of tibia make these fractures vulnerable to non-union and infection. The rate of infection may be as high as 50% in grade-IIIB open fractures [1]. Attempts to reduce these complications have led to aggressive protocols which include immediate intravenous antibiotics, repeated soft-tissue debridement, stabilization of the fracture, early soft-tissue cover and prophylactic bone-grafting [2,3]. External fixation has been popular because of the relative easy of application and the limited effect on the blood supply of the tibia, but these advantages have been outweighed by high incidence of pin-track infection, difficulties related to soft-tissue management and the potential for mal-union [4-7]. However, with use of systemic antibiotics and better avoidance of bone gap [8] now-a-days also prefer flexible intramedullary nailing, which provides a relatively more stable fixation and better bone union efficacy with less bone cavity exposure and less bone marrow related complications [9]. We reviewed the
results of comparative studies and controlled trials designed to determine the therapeutic effects of the 2 different methods. As the choice of these two methods remained inconsistent, our purpose were to better define their advantages and disadvantages, and thereby enabling better decision making in a tertiary level health facility.
This is a Retrospective and prospective study at Department of Orthopaedic in LNCT medical college & Sewakunj hospital and research centre Indore from June 2021 to March 2023. Twenty six patients who presented with open fractures of the tibial shaft type II, IIIA, and IIIB (Gustilo) were treated. In this study we included the patients of both sexes, age between 18-65 years with diaphysial fractures 5cm distal to the tibial tuberosity and at least 5 cm proximal to the tibial plafond, irrespective of fibula fracture and Open fractures type II, IIIA, and IIIB according to Gustilo Anderson classification. We excluded the patients with intraarticular fractures of proximal and distal tibia, closed fractures and Gustilo type IIIC fractures, multiple comorbities, surgically unfit patient, unwilling patient. In this study 18 male and 8 female were included. Other than the fixation method, standard treatment protocol followed for both groups. Thirteen patients were treated by external fixator and thirteen patients by flexible intramedullary nailing.
In this study younger patients were more prone for open fracture because those are more active and outside worker. The incidence is higher in male population is due to the distribution of high energy and heavy work in male population as compare to female population. According to side of extremity right and left side is injured equally in our study. (Table 1-5).
External fixator group:
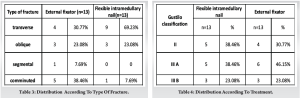
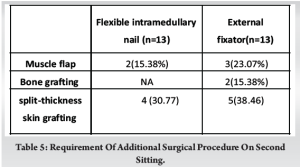
The patients in external fixator group comprised of 13 patients. The average age of the patients was 38 years (25 to 60 years). All fractures patients were stabilised by external fixator. In all cases delta configuration for fixation were used. Ten fractures (76.92%) were used six schanz pin per case and three patients (23.08%) used seven pin per case. The average time in external fixation was 12 weeks. After removal of fixator ten fractures patients were treated with a cast, but two patients require second surgery as bone grafting. Three patients required muscle flap surgery to cover the bone. The time of union averaged 27.08 weeks (26 to 30 weeks); the average time for union was 26 weeks for grade II, 26.75 weeks for grade IIIA, 27.66 weeks for grade IIIB. Two fracture (15.38%) had 7 degree of valgus angulation; two (15.38%) had 7 degree of varus mal-union, three patients had between 7 and 10 degree of recurvatum, two patients present with comminuted fracture healed with shortening of 1 cm. 8 fracture had between 110 and 130 degree knee flexion, four patients had 100 or less knee flexion, two patients had 5 degree of extension deficit. Two patients had major loss of dorsiflexion of the ankle. Two patients had equines contracture. Three fracture patients (23%) had loosening of schanz pin from insertion site. Seven patients were associated with mild pain in the leg, and pain usually was exacerbated by activity.no neurovascular complications were associated with the insertion of pins. The total number of operations averaged 2.3 including debridement, delayed primary closure, removal of fixator and application of a cast, iliac-crest bone–grafting, split-thickness skin grafting, local or free flap coverage. In six patients (46.15%), a pin track infection developed. Five patients infection cleared after application of betadine pin track dressing and antibiotics but one needed curettage of the infected tract. Two patients (15.38%) grade IIIB developed deep infection (chronic osteomylitis) with pus discharging sinus and were convert in infected non-union.
Flexible intramedullary nailing group-
The flexible intramedullary nailing group consisted of thirteen fracture patients. The average age of the patients was 36 years (range 20 to 62 years). Eight fracture (61.54%) needed only two flexible intramedullary nail, three fracture (23.08%) were stabilised with three nail, and two (15.38%) had four nails. The average duration of immobilisation, generally with slab, was 2.7 months. The 4.0 mm nail was most commonly used, although the 4.5 mm nail was inserted in young patients who had a large medullary canal. Union was occurred in all patients. The time to union averaged 25 week (range 22 to 28 weeks); the average time of union was 23.5 weeks for grade II fractures; 25.6 weeks for grade IIIA; 26.5 weeks for grade IIIB. One fracture (7.69%) had 8 degree of valgus angulation, one fracture (7.69%) had 7 degree of recurvatum. Ten fracture (76.92%) had 130-degree knee flexion, two patients (15.38%) had 120 or less knee flexion; no one patients had extension deficit; ankle movement of normal in all patients. In two patient one nail back out through the skin, no nail broke in the shaft portion. Two (15.38%) patient were complaint of nail insertion site pain, patients needed removal of nail for relief of pain. Three patients (23.08%) were associated with mild activity related pain in the leg at the level of fracture. The total number of operations averaged 1.8 including debridement, delayed primary closure, skin grafting, local or free flap coverage and removal of nail.
With all methods of treatment of compound tibia fractures the major problem encountered are infection, non-union, joint stiffness and mal alignment. All these complications prolong the patient’s disability. Mean age in our study was 36 years for flexible intramedullary nailing group and 38 years for external fixator group which was quite comparable to other studies (Graph- 1). All these studies show that these injuries occur in a younger age group [10-12].
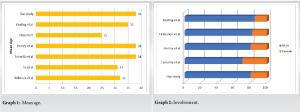
In present study male involvement was in 69.23% (18 patients) and female involvement was 30.76% (8 patients).Which is almost identical to other studies in the literature. (Graph – 2). Several series of patients who were treated only by external fixation have been published. Dr. Muhammedimran et al (2007) [13] conducted study on 25 patients with open fractures of the tibia diaphysis. The end result of the external fixation of 25 tibia shaft fractures; 18 (72%) men and 7(28%) women with average age of 37.7 years (16-65 years). The union rate was 83%, non-union rate was 12% and mal-union was 5%. Pin track infection rate was 10% and average time of union was 28.5 weeks (15-22 weeks). John and Holbrook et al (1989) [14] conducted study on sixty-three open tibia fractures using external fixation in twenty-eight patients. Average age 25 years, average time of union 26 wks, mal-union in ten patients (36%) non-union was in 3 patients (11%), pin track infection presents in 6 patients (21%). In present study for external fixation mean age was 38 years (25-60). The union rate was 84.4%, non–union rate 16.6% and malunion was 33.3%. Pin track infection rate was 50%. And average time of union 27.08 weeks (26-30 weeks). A shikali et al (2010) [15] fixation of compound fractures of distal tibia with external fixator mean time of union 24 weeks. Tucker et al [16] and schatzker [17] in separate studies reported union time of 25.6 weeks and 21.9 weeks respectively. Similarly, wheelwright and court brown [18] and antich et al [19] reported a union rate of 27.5 weeks and 26 weeks respectively. Kaftandziev [20] in his study produced union in 71.1% of the patients. Bratislav stojkovic [21] reported a union rate of 83.68% in his 49 patients. Kimmel [22] reviewed fifteen open tibia fractures that were treated with external fixation noted a 7 percent rate of non-union, a 50 percent rate of pin tract drainage, a 47 percent rate of osteomyelitis, and 26 percent rate of malunion. In present study rate of osteomyelitis is 16.6% which is lower than above study. Velazco and fleming [23] studied on fourty open tibial fractures, noted an 80 percent rate of pin tract infection, a 12.5 percent rate of delayed union, and 12.5 percent rate of amputation. Malunion were not described. Because of the disadvantage of external fixation, interst in nailing without reaming of tibia fractures is increasing. Dobozi et al [24] reported on 192 tibial fractures, including sixty-one open fractures that were treated with flexible intramedullary nailing. They noted a 5 percent of malunion, a 3 percent rate non-union, and 3 percent of deep infection in the open fracture group. John and Holbrook et al (1989) conducted study on sixty three open tibia fractures used enders nailing in twenty-nine patients, average age 28 years, average time of union 24 wks, mal-union in 6 patients (21%) non- union rate was 10%, pain at nail head in 11 patients (38%). In present study results for flexible intramedullary nailing, the mean age is 36 years (20-62 years), mal-union is 8.3%, pain at nail head rate is 16.6%. And average time of union is 25 weeks. Union achieved in all cases. These study result were approximately same to above mentioned studies. Flexible intramedullary nail offers advantages of Good fixation and control of alignment without periosteal stripping or risk of pin tract infection, early walking with weight-bearing, low incidence of infection, good acces for care of the wound and early mobilisation of the joint. Flexible intramedullary nails have some disadvantages also like frequent use of a second surgery for nail removal procedure, the necessity for surgical expertise in closed nailing, less secure fixation in fracture of the distal and proximal one –thirds of the tibia and in comminuted fractures, possibility of loss of reduction, discomfort in the knee joint from prominent nail–heads, the risk of extension of infection throughout the medullary canal. (Table 6)
Limb alignment was better maintained by flexible intramedullary nail group than by external fixation. Fracture treated with flexible intramedullary nail had fewer infection /inflammations than did those treated with external fixator, as expected the external fixator group was prone to pin tract problems, and these problems contributed to a statistically significant higher incidence of these complications at surgical interfaces for this fixation method. The incidence of osteomyelitis was higher in external fixation group. The patients in the external fixation group needed considerably more operative procedures. In external fixator group three patients required muscle flap surgery for wound closure. Many patients in the external fixation group complained of pain at the fracture site due to mild activity compared with the patients in the enders nailing group. The rate of discomfort in the knee joint due to prominent nail-head was problem in ender nailing group and was similar to that in the other reported series. Postoperative hospital staying was varied 5-7 days in flexible intramedullary nail group but in external fixator hospital stay duration more than flexible intramedullary nail group because patients need proper physiotherapy training and learned self-pin track dressing. In external fixator group were required readmission of two patient for non-union treatment. Final Functional result on modified Ketenjian criteria of flexible intramedullary nail is excellent (83.3%), good (16.6%) as compared to external fixator is excellent (50%), good (25%), fair (8.3%), and poor (16.6%).
This study of 26 patients of open tibia fractures, treated by using a prospective, systematically allocated protocol, shows that flexible intramedullary nailing is more efficacious than external fixator. Advantages observed are maintaining limb alignment and fewer serious complication, fewer operation needed, and a better range of motion of adjacent joints obtained. It reduces hospital stay of patients and later patient can return early to work, thus minimizes psychological trauma and financial burden. Flexible intramedullary nailing has easy learing curve. External fixator group had more disability and difficulties in daily routine activity like sleeping, bathing and other social activity. Intramedullary nailing for Gustilo’s grade I is established worldwide. Availability of plastic surgery facility, better asepsis and newer broad-spectrum antibiotics are encouraging nailing in grade II also. Dilemma between rigid nailing and external fixator is persisting in grade II, IIIA, IIIB. Authors feel role of flexible intramedullary nailing is better than external fixator in these fractures.
Open tibial fractures are among the most common long bone fractures. Clinically, the treatment of open tibial fractures remains a major therapeutic problem for surgeons because of the poor soft tissue coverage and blood supply in the tibia. This study shows that flexible intramedullary nailing is more efficacious than external fixator because by nail maintaining limb alignment is better, fewer serious complication, fewer operation needed, and a better range of motion of adjacent joints obtained.
References
- 1.Court-Brown CM, Rimmer S, Prakash U, McQueen MM. The epidemiology of open long bone fractures. Injury. 1998;29:529–534. doi: 10.1016/S0020-1383(98)00125-9. [PubMed] [CrossRef] [Google Scholar] [Google Scholar | PubMed | CrossRef]
- 2.Giannoudis PV, Papakostidis C, Roberts C. A review of the management of open fractures of the tibia and femur. J Bone Joint Surg Br. 2006;88:281–289. doi: 10.1302/0301-620X.88B3.16465. [PubMed] [CrossRef] [Google Scholar] [Google Scholar | PubMed | CrossRef]
- 3.French, B. & Tornetta, P. 3rd. High-energy tibial shaft fractures. Orthop Clin North Am33, 211–230, ix (2002). [PubMed] [Google Scholar | PubMed]
- 4.Gustilo R.B., Anderson J.T. Prevention of infection in the treatment of 1025 open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453–458. [PubMed] [Google Scholar] [Google Scholar | PubMed]
- 5.Gustilo R.B., Gruninger R.P., Davis T. Classification of type III (severe) open fractures relative to treatment and results. Orthopaedics. 1987;10:1781–1788. [PubMed] [Google Scholar] [Google Scholar | PubMed]
- 6.Gustilo R.B., Mendoza R.M., Williams D.N. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24:742–746. [PubMed] [Google Scholar] [Google Scholar | PubMed]
- 7.Henley M.B. Intramedullary devices for tibial fracture stabilization. Clin Orthop. 1989;240:87–96. [PubMed] [Google Scholar] [Google Scholar | PubMed]
- 8.Kakar S, Tornetta P., III Open fractures of the tibia treated by immediate intramedullary tibial nail insertion without reaming: a prospective study. J Orthop Trauma. 2007;21(3):153–57. [Google Scholar | PubMed]
- 9.Melvin JS, et al. Opentibial shaft fractures: II. Definitive management and limb salvage. J Am AcadOrthop Surg. 2010;18(2):108–17. [Google Scholar | PubMed]
- 10.Olson SA. Open Fractures of the Tibial Shaft. The Journal of Bone and Joint Surgery 1996; 78-A: 1428-1437 [Google Scholar | PubMed]
- 11.Ostermann PAW, Selgison D, Henry SL. Local Antibiotic Therapy for Severe Open Fractures. The Journal of Bone and Joint Surgery 1995; 77-B: 93-97 [Google Scholar | PubMed]
- 12.Bhandari M, Guyatt GH, Swiontkowski MF, SchemitschEH.Treatment of Open Fractures of the Shaft of the Tibia. The Journal of Bone and Joint Surgery 2001; 83-B: 62-68. [Google Scholar | PubMed]
- 13.Khan MI, Saqib M, Alam W. Open tibial shaft fractures; treatment with external fixator. Professional Med J 2014;21(4): 654-658 [Google Scholar | PubMed]
- 14.Treatment of open fractures of the tibia shaft;enders nailing versus external fixation. A randomised ;prospective comparison JH Holbrook; MF swiontkowski;R sanders ,J bone joint surg AM ,1989 sep,71(a); 1231-1238. [Google Scholar | PubMed]
- 15.A sikali,awani ,k padha, m bhatti, h dang fixation of compound fracture of distal tibia using external fixator as a definite modality ,of treatment the internet journal of orthopaedic surgery 2010 volume 18 number 2. [Google Scholar | PubMed]
- 16.Tucker HL, Kendra JC, Kinnebrew TE. Management 18.A sikali,awani ,k padha, m bhatti, h dang fixation of compound fracture of distal tibia using external fixator as a definite modality ,of treatment the internet journal of orthopaedic surgery 2010 of unstable open and closed fractures using the Ilizarov Method. Clin Or thop1992;280:125-35. [Google Scholar | PubMed]
- 17.Schatzker H, David R, Stolero J, Grimberg B, Soundry M. Treatment of open tibial fractures with primary suture and Ilizarov fixation. Clin Or thop 1997;335:268-74. [Google Scholar | PubMed]
- 18.Wheelwright EF, Court-Brown CM. Primary external fixation and secondary intramedullary nailing in the treatment of tibial fractures. Injury 1992;23:373-6. [Google Scholar | PubMed]
- 19.Adrover PA, Garin DM, Alvarez JM, Alonso CP. External fixation and secondary intramedullary nailing of open tibial fractures. The journal of bone and joint surgery 1997;79(3):433-37. [Google Scholar | PubMed]
- 20.Kaftandziev I, Pejkova S, Saveski J. Operative treatment of iii grade open fractures of the tibial diaphysis. Contribution, Sec. Biol. Med. Sci. XXVII/1 (2006) 121–131. [Google Scholar | PubMed]
- 21.Bratislav S, Saša M, Mile R, Miodrag S, Igor K. Tibial shaft fractures treated by the external fixation method. Medicine and Biology 2006;13(3):145-47. [Google Scholar | PubMed]
- 22.Kimmel RB; results of treatment using the Hoffman external fixator for fracture of tibial diaphysis.J.trauma,22:960-965,1982 [Google Scholar | PubMed]
- 23.Velazco,A,and fleming,LL ,open fractures of tibia treated by the Hoffman external fixator. Clin.orthop,180:125-132,1983. [Google Scholar | PubMed]
- 24.Dobozi,WR and pankovich AM ,Segal,David;Saltzman,Martin;and wiss ,Donald; flexible intramedullary nailing of open tibia shaft fractures , scientific exhibit at the annual meeting of the American academy of orthopaedic surgeons,At. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2020 Amputation in Necrotizing Fasciitis – Dilemma or Reality: A Case Report and Literature Review
July 10, 2020 Amputation in Necrotizing Fasciitis – Dilemma or Reality: A Case Report and Literature Review December 4, 2020 Modified Technique for Patellar Tendon Repair Post-Total Knee Arthroplasty: A Case Report
December 4, 2020 Modified Technique for Patellar Tendon Repair Post-Total Knee Arthroplasty: A Case Report December 4, 2020 Tibial Nerve Schwannoma: An Unexplained Cause of Lateral Foot Pain – A Rare Case Report and Review
December 4, 2020 Tibial Nerve Schwannoma: An Unexplained Cause of Lateral Foot Pain – A Rare Case Report and Review December 1, 2025 Successful Staged Bilateral Hip and Knee Arthroplasty in a Patient with Long-standing Rheumatoid Arthritis with Severe Deformities
December 1, 2025 Successful Staged Bilateral Hip and Knee Arthroplasty in a Patient with Long-standing Rheumatoid Arthritis with Severe Deformities