
Middle phalanx fractures could potentially be stabilized with the help of double screws gaining rigid construction.
Dr. Mojahed Sakhnini, Meuhedet, Health Services, Israel. E-mail:Mojahed.sakh@gmail.com
Introduction: Techniques for treating phalangeal fractures are evolving. Intramedullary screws are a trendy surgical choice that leads to optimal results. Metacarpals and proximal phalanges could tolerate two screws. We want to demonstrate that middle phalanx fractures could also be treated with double-cannulated screws.
Case Report: A 19-year-old patient with a middle phalanx fracture of the 4th left digit was treated with Kirschner wires leading eventually to malunion. We revised the fracture with a redo, recreating the fracture and introducing retrograde crossed-cannulated screws with excellent stability that allowed an immediate range of motion. The patient achieved union with full grip and range of motion.
Conclusion: Middle phalanx fractures could be treated with two screws in a crossed configuration achieving stable fixation and obviating the proximal interphalangeal joint.
Keywords: Screws, intramedullary, fracture, middle phalanx, double
Fractures of the phalanges are common [1, 2]. New techniques have evolved to gain better outcomes and to hasten return to work following injury [3, 4]. Cannulated screws act as internal splints and allow an early range of motion. They have superior outcomes regarding union, range of motion, and time to return to work in comparison to Kirschner wires [5, 6]. Some studies demonstrated the option of introducing two screws in the metacarpal and proximal phalanx and called it Y-strutting [3, 7]. We opt to demonstrate that two screws could be inserted into the middle phalanx with straight forward simple technique.
A 19-year-old patient who came to our department after a crush injury from a car’s door was diagnosed with an open middle phalanx displaced fracture in the left 4th digit (Fig. 1). He was operated on upon arrival. The procedure included irrigation debridement and fixation with Kirschner wires (Fig. 2). Following the procedure the patient was put in a splint that was removed after 10 days to allow mobilization of the proximal interphalangeal (PIP) joint under the supervision of occupational therapy. During follow-up, the patient gained union of the fracture but with clinical malrotation as the 4th digit rided the 3rd digit impeding full grip. The patient was called for revision surgery for osteotomy and realignment 5 weeks following the primary surgery.


Surgical technique
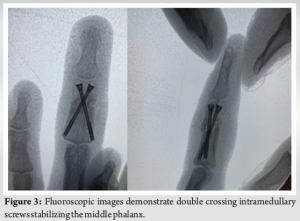
With a minimally invasive approach, a 1 cm radial mid-axial approach was utilized for the distal third for the middle phalanx. After exposing the fracture site, an osteotome and freer elevator were utilized to help reproduce the original fracture line. Following this step, while maintaining the digit in reduction following correction of the malrotation, two crossing retrograde Kirschner wires were introduced in X configuration from the set of 1.7 mm cannulated compression screw system (CCS 1.7 mm, APTUS, Medartis). The two K-wires were introduced in a way that will allow the insertion of twin self-drilling screws that will not meet in the sagittal plane (Fig. 3). Following inserting the screws, the K-wires were removed. The X-configuration screws stabilized the osteotomy site and kept its position. This allowed an immediate range of motion following the surgery.
Outcome
The fracture healed with the osseous union (Fig. 4). Clinically the patient had a full range of motion with a symmetric power grip (Fig. 5).

Treating phalanx fractures with intramedullary screws is an evolving practice that was introduced by Del Piñal et al. [3]. Multiple studies have shown the benefit of intramedullary screws treating phalanx fractures to achieve stability and allow an early range of motion [4, 8]. A good outcome is anticipated regarding the range of motion and union with marginal complications [9, 10]. The screw could either be introduced in antegrade or retrograde fashion [11-13]. Metacarpals and proximal phalanx fractures could be treated with either one cannulated screw or two screws depending on the fracture configuration [7, 14]. While multiple studies included middle phalanx fractures series treated with cannulated screws, none to our knowledge described two screws configuration to address this fracture [3, 8]. George et al. [15] described 23 middle phalanx fractures that were treated with a 1.7 mm or 2.2 mm cannulated screw that was inserted in the retrograde technique with good results. Middle phalanges are smaller than metacarpals and proximal phalanges, yet they can withhold two cannulated screws [16]. Our case report stands out as it demonstrates the capacity of the middle phalanx to hold in double screws which will add to the stability of the construct allowing immediate range of motion and potentiating union. By introducing the K-wires in a retrograde fashion at the edge of the phalanx head, it could be aimed proximally in X-configuration by allowing one wire to be dorsal and the other volar. Then we insert the 1.7 mm cannulated screws that swallow the 0.6 mm K-wires in a length that will engage the cortical contralateral edge. Our hypothesis is that this technique will allow a superior purchase than one screw construct of a 2.2 mm cannulated screw and obviate the cartilaginous surface of the PIP joint leading to a better outcome. We recognize the anecdotal nature of this case report. Our main aim is to demonstrate that middle phalanx fractures could be approached with two screws as is the case in metacarpal and proximal phalanx fractures. Still, more biomechanical and clinical studies should be performed to confirm the superiority of this technique versus one screw classical technique.
This case report demonstrates the potential of the middle phalanx of the hand to contain two crossing intramedullary screws not violating the PIP joint. This technique endows a rigid construct that allows immediate motion of adjacent joints.
When feasible, middle phalanx fracture could be approached with crossing double screws, especially when stiffness is feared and an early range of motion is warranted.
References
- 1.Van Onselen E, Karim RB, Hage JJ, Ritt MJ. Prevalence and distribution of hand fractures. J Hand Surg 2003;28:491-5. [Google Scholar]
- 2.Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg 2001;26:908-15. [Google Scholar]
- 3.Del Piñal F, Moraleda E, Rúas JS, de Piero GH, Cerezal L. Minimally invasive fixation of fractures of the phalanges and metacarpals with intramedullary cannulated headless compression screws. J Hand Surg 2015;40:692-700. [Google Scholar]
- 4.Chao J, Patel A, Shah A. Intramedullary screw fixation comprehensive technique guide for metacarpal and phalanx fractures: Pearls and pitfalls. Plast Reconstr Surg Glob Open 2021;9:e3895. [Google Scholar]
- 5.DelPrete CR, Chao J, Varghese BB, Greenberg P, Iyer H, Shah A. Comparison of intramedullary screw fixation, plating, and K-wires for metacarpal fracture fixation: A meta-analysis. Hand (N Y) 2024:15589447241232094. [Google Scholar]
- 6.Supichyangur K, Tananon T, Sripakdee SA, Chunyawongsak V. Prospective comparison of the early outcomes of headless compression screw and percutaneous K-wire fixation in metacarpal fractures. J Hand Surg 2023;48:950.e1-9. [Google Scholar]
- 7.Gray RR, Rubio F, Heifner JJ, Hoekzema NA, Mercer DM. Double barrel screw fixation for proximal phalanx fracture. Tech Hand Up Extrem Surg 2022;26:214-7. [Google Scholar]
- 8.Giesen T, Gazzola R, Poggetti A, Giovanoli P, Calcagni M. Intramedullary headless screw fixation for fractures of the proximal and middle phalanges in the digits of the hand: A review of 31 consecutive fractures. J Hand Surg Eur Vol 2016;41:688-94. [Google Scholar]
- 9.Sivakumar BS, An VV, Graham DJ, Ledgard J, Lawson RD, Furniss D. Intramedullary compression screw fixation of proximal phalangeal fractures: A systematic literature review. Hand 2022;17:595-601. [Google Scholar]
- 10.Hug U, Fiumedinisi F, Pallaver A, van de Wall BJ, Beeres FJ, Giesen T, et al. Intramedullary screw fixation of metacarpal and phalangeal fractures - A systematic review of 837 patients. Hand Surg Rehabil 2021;40:622-30. [Google Scholar]
- 11.Jovanovic N, Aldlyami E, Saraj B, Fm Seidam M, Badawi H, Shaat AA, et al. Intramedullary percutaneous fixation of extra-articular proximal and middle phalanx fractures. Tech Hand Up Extrem Surg 2018;22:51-6. [Google Scholar]
- 12.Bui GA, Huang JI. Intramedullary screw fixation of metacarpal and phalangeal fractures. Hand Clin 2023;39:475-88. [Google Scholar]
- 13.Guidi M, Frueh FS, Besmens I, Calcagni M. Intramedullary compression screw fixation of metacarpal and phalangeal fractures. EFORT Open Rev 2020;5:624-9. [Google Scholar]
- 14.Gaspar MP, Gandhi SD, Culp RW, Kane PM. Dual antegrade intramedullary headless screw fixation for treatment of unstable proximal phalanx fractures. Hand (N Y) 2019;14:494-9. [Google Scholar]
- 15.George AR, Abbot H, McCarron L, Graham DJ, Sivakumar BS. Intramedullary Compression Screw Fixation for Middle Phalangeal Fractures. The Journal of Hand Surgery. 2024 Feb 2. [Google Scholar]
- 16.Aydinlioglu A, Akpinar F, Tosun N. Mathematical relations between the lengths of the metacarpal bones and phalanges: Surgical significance. Tohoku J Exp Med 1998;185:209-16. [Google Scholar]



