
Total hip replacement can be successfully performed in multiple-times failed fixation of subtrochanter fracture.
Dr. Bushu Harna, Department of Orthopaedic Surgery, Indus International Hospital, Derrabassi, Panjab, India. E-mail: bushu.edu@gmail.com
Introduction: Subtrochanteric fractures are difficult fractures to manage, and a failed fixation in these fractures is a complex and challenging entities. Re-osteosynthesis and prosthesis replacement are two viable options. We present a case of four failed subtrochanter fracture fixations, managed with cementless long stem total hip replacement and augmented plate.
Case Report: A 68-year-old lady presented with pain and difficulty in walking for 12 years with four failed surgeries. The initial diagnosis was a subtrochanteric fracture managed with a proximal femur nail. The construct failed and was revised with a proximal femur plate. After a few years, the plate was broken and revised with the proximal femur nail again. Subsequently, the nail also failed after 3 years for which re-osteosynthesis with proximal femur nail was performed. The fixation again failed after 3 years leading to the inability to bear weight on the limb and pain. Cementless long stem total hip replacement with augmented plate along with bone grafting was performed as a one-time solution to the complexities in the management of 4 time-failed subtrochanter femur fractures. At 1 year of follow-up, the patient was walking pain-free and independently without any aid.
Conclusion: Failed subtrochanter femur fracture fixation is a complex situation to manage. Re-osteosynthesis is the favored modality of treatment but prosthesis replacement is a feasible option in elderly patients. Total hip replacement provides a single solution to all the intricate problems in the management of failed subtrochanter femur fractures in the elderly.
Keywords: Long stem, salvage, failed fracture fixation, total hip replacement, subtrochanter fracture.
The prevalence of proximal femur fractures is increasing owing to the longer life expectancy and high-velocity traumas. The subtrochanteric fractures are however the ones which are seen both in the younger as well as the elderly [1]. The subtrochanteric region is present from the lesser trochanter to the 5 cm distally. Subtrochanteric region fractures had been successfully treated with various intramedullary and extramedullary fixation techniques. The presence of high stress and traction forces in this region poses a challenge for management [2]. There is no single implant or technique available to cater to all the variations and difficulties in fracture fixation. There are various reasons for fixation failure in these fractures including wrong implant selection, mal reduction, improper surgical technique, and delayed or non-union at the fracture site. Failure of the fixation could lead to a disastrous result leading to complex problems for further fracture management. The challenges after fracture failure include complex fracture patterns, infections, compromised soft tissue, poor bone stock, and suboptimal fixation subsequently. Prosthesis replacement is now considered a feasible option in elderly patients after subtrochanter fracture fixation failure [3,4]. Although re-fixation was considered a standard and time-tested procedure with high failure rates [5]. There is few published literature favoring hip replacement as a salvage procedure in failed subtrochanter fracture fixation [4-8]. We present a rare case of 4 times failed subtrochanteric fracture fixation in an elderly female, managed successfully with hip replacement and augmented plating.
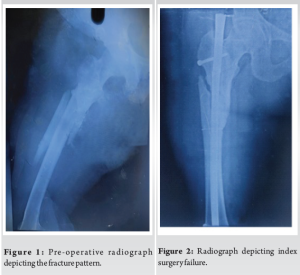
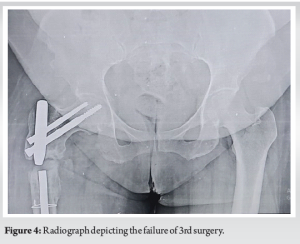
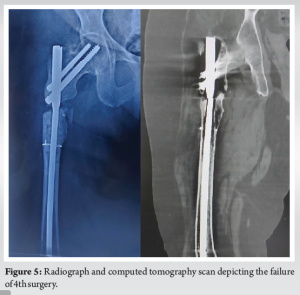
A 68-year-old lady presented in the outpatient department with a complaint of pain in the left thigh and inability to bear weight for the past 12 years. The patient initially suffered a road traffic accident leading to an isolated subtrochanter femur fracture on the left side (Fig. 1). The patient was initially managed with a femur nail (Fig. 2) but always complained of pain and inability to bear weight on that limb since then. The patient was re-operated, probably for non-union at the fracture site after 3 years of the index surgery. The patient was managed with a proximal femur locking plate with autologous bone grafting. The patient was partial weight bearing on that limb for the next 3 years. The patient was never pain-free nor able to bear full weight on that limb. The pain subsequently increased over the period of the next 3 years. The radiographs depicted a broken femur locking plate with no union at the fracture site (Fig. 3). The patient again underwent revision surgery with proximal femur nail and autologous bone grafting. The patient was also given an injection of teriparatide for 3 months. The next 3 years were uneventful with bearable pain and partial weight-bearing mobilization with a walker. The patient one day suffered a jerky movement leading to exaggerated pain in the left thigh. The radiographs depicted a broken proximal femur nail and non-union at the fracture site (Fig. 4). The patient underwent 4th surgery, 9 years post-index surgery. The patient was again managed with the proximal femur nail. The patient was never able to even partial weight bear on that limb after the surgery. After 3 years of the 4th surgery, the patient presented to our hospital with pain in the left thigh and an inability to bear weight on that limb. Over the past 12 years (post-injury) due to decreased activities and inability to mobilize independently, the patient gained 35 kg of weight and currently weighed 125 kg. There were three long surgical scars over the thigh with no signs of infection. The patient was unable to stand and had excruciating pain while sitting or standing with support. The radiographs depicted a broken proximal femur nail with a gap non-union at the fracture site (Fig. 5). The computer tomography (CT) depicted non-union at the fracture site with a bone gap of around 2–3 cm (Fig. 5). The patient was counseled and considering the age, and repeated failure of osteosynthesis, hip arthroplasty was planned. The biochemical markers for infections (erythrocyte sedimentation rate, C-reactive protein, and procalcitonin) were within the normal range.

Surgical challenges and technique
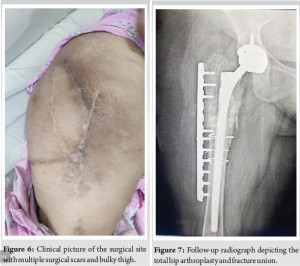
The patient was planned for long-stem total hip arthroplasty (THA). There were three surgical healed scars (Fig. 6) on the left thigh, not appropriate for implant removal and THA. The middle scar was utilized for Moore’s approach and implant removal. The thigh was bulky and stout. Deep retractors were used to reach the fracture site and acetabulum.
The initial challenge was to remove the broken nail in an osteoporotic bone. The CT scan helped in the assessment of the size and fitness of the nail in the medullary canal. The nail was lying loose in the canal and was easily extracted after removing the bolts of the nail from the fracture site. The proximal fragment was osteoporotic with multiple holes. The margins of the fracture site were freshened. The proximal fragment was manipulated with the help of a Schanz screw and the femoral head was dislocated posteriorly. The acetabulum was prepared and a hydroxyapatite-coated cementless cup was placed (XL- axenture Resurge cup II®, 50 mm). The femoral canal preparation was performed. On careful observation, a faint fracture line was recognized extending distally 5–6 cm from the non-union fracture site. This was stabilized by three loops of stainless-steel wires. The 260 mm long cementless stem (XL- axenture Resurge stem®, 16 mm × 260 mm) was placed through the proximal fragment of the proximal femur. There was a bone gap of around 3–4 cm after debridement and placing of the stem. The bone from the femoral head was morselized and placed at the fracture site. The proximal fragment of the proximal femur was osteoporotic and hollow. There was no purchase of the stem in the proximal fragment. The proximal fragment was stabilized with a locking plate. Two units of blood transfusion were given intraoperatively.
The wound was thoroughly washed and infiltrated with 1 g of injection vancomycin and tranexamic acid. The wound closure was performed in layers and compression bandage was given. The patient had an uneventful post-operative period and the wound healed over 3 weeks. She was mobilized on post-operative day 1 with the help of a walker. She was allowed to weight bear as tolerated for the next 3 weeks. Gradually the mobilization improved at 4 weeks, 8 weeks, and 6 months. The patient was full weight bearing at 6 months postoperatively. At 1.5 years follow-up, the patient was walking independently pain-free, without any aid, and radiographs depicting the fracture union and implant in situ (Fig. 7).
Subtrochanteric femoral fractures are commonly encountered in the emergency room by orthopedic departments. However, dealing with a failed subtrochanteric fracture presents a completely different and more challenging aspect of management. In younger patients, re-fixation is often the preferred treatment choice. In this particular case, a patient underwent four re-fixation attempts using nail and plating systems. While some studies in the literature advocate for a total hip replacement as a better salvage option compared to re-osteosynthesis, hemiarthroplasty is also considered for salvage procedures. Nevertheless, failed surgeries can result in poor bone and cartilage quality, making total hip replacement a more suitable option over hemiarthroplasty. Although a few studies are recommending total hip replacement after failed proximal femur fracture fixation, mostly performed for failed intertrochanter femur fracture. Consequently, fewer studies have reported on the outcomes of hip replacement in failed subtrochanteric fracture fixation. Enocson et al. [4] conducted a study involving 88 patients who underwent salvage arthroplasty after experiencing failed fixation of either trochanteric or subtrochanteric fractures. The authors utilized standard femoral stems or long stems for all patients. The follow-up period ranged from 5 to 11 years, with a revision rate of 16% (14 out of 88 hips). These results suggested that arthroplasty could be a successful approach for failed fixations. The use of long stems was based on the idea of bridging the previous bone defect, thereby reducing the risk of reoperation. Similarly, in this case, we performed long stem cementless total hip replacement. To the best of our knowledge, this is the first case reported in the English literature depicting the success of total hip replacement after four subtrochanteric femur fracture fixation failures. Weiss et al. [9] also presented a case series involving 30 patients who underwent salvaged total hip replacements following failed proximal femur fractures. In their study, a modular cementless stem was used for all cases, and the follow-up period was 4 years. The reoperation rate was found to be 23%, with 7 out of 30 patients requiring reoperation due to failed trochanteric or subtrochanteric fractures. Similarly, Jin et al. [10] reported 18 patients of salvage total hip replacement after failed subtrochanteric fixation. The mean follow-up period for these cases was 5.2 years, and only one out of the 18 patients required reoperation. The findings from their study were consistent with previous research, indicating good pain relief and independent walking without support. While existing studies have generally shown replacement as a suitable option after one or two failed fixation surgeries, the case mentioned in this case report involved four failed surgeries, raising concerns about the appropriateness of replacement as a salvage option. Consequently, a randomized controlled trial is warranted to assess the efficacy of proximal femur failed fixation salvage procedures and to establish a proper consensus and protocol among surgeons. Such research would provide valuable insights into the best approach for managing failed subtrochanteric femoral fractures, leading to improved patient outcomes and optimized treatment strategies for this challenging condition. In this patient apart from the long stem total hip replacement we added augmented plating and filled the fracture gap with bone graft from the femoral head. The idea was to stabilize the proximal femur fragment, which was loose as there was no hold of the stem in the proximal fragment. The abductor muscles of the hip were attached to this proximal femur fragment. The augmented plate stabilized this fragment even after the contraction of these muscles while walking and minimizing the micromotion at the fracture site. This helped in the union at the fracture site and faster rehabilitation.
Subtrochanteric femoral fractures can present significant challenges for orthopedic departments, especially when dealing with failed fixation. While re-fixation is often preferred in younger patients, total hip replacement emerges as a promising salvage option, particularly in cases where multiple re-fixation attempts have been unsuccessful. However, existing studies suggest favorable outcomes with the use of standard or long femoral stems in salvage arthroplasty. Further research, including randomized controlled trials, is needed to establish a consensus and protocol for managing failed subtrochanteric fractures and to enhance the effectiveness of salvage procedures.
Total hip replacement can be successfully performed as a salvage procedure in subtrochanter femur fracture fixation failure. THR not only obviates the need for fracture union but also provides the opportunity for immediate weight-bearing mobilization in such patients. The THR should be considered even after one or two subtrochanter fracture fixation failures.
References
- 1.Haidukewych GJ, Berry DJ. Nonunion of fractures of the subtrochanteric region of the femur. Clin Orthop Relat Res 2004;419:185-8. [Google Scholar | PubMed]
- 2.Joglekar SB, Lindvall EM, Martirosian A. Contemporary management of subtrochanteric fractures. Orthop Clin North Am 2015;46:21-35. [Google Scholar | PubMed]
- 3.Lotzien S, Rausch V, Schildhauer TA, Gessmann J. Revision of subtrochanteric femoral nonunions after intramedullary nailing with dynamic condylar screw. BMC Musculoskelet Disord 2018;19:448. [Google Scholar | PubMed]
- 4.Enocson A, Mattisson L, Ottosson C, Lapidus LJ. Hip arthroplasty after failed fixation of trochanteric and subtrochanteric fractures. Acta Orthop 2012;83:493-8. [Google Scholar | PubMed]
- 5.Dziadosz D. Considerations with failed intertrochanteric and subtrochanteric femur fractures: How to treat, revise, and replace. J Orthop Trauma 2015;29:S17-21. [Google Scholar | PubMed]
- 6.Luthringer TA, Elbuluk AM, Behery OA, Cizmic Z, Deshmukh AJ. Salvage of failed internal fixation of intertrochanteric hip fractures: Clinical and functional outcomes of total hip arthroplasty versus hemiarthroplasty. Arthroplast Today 2018;4:383-91. [Google Scholar | PubMed]
- 7.Shi X, Zhou Z, Yang J, Shen B, Kang P, Pei F. Total hip arthroplasty using non-modular cementless long-stem distal fixation for salvage of failed internal fixation of intertrochanteric fracture. J Arthroplasty 2015;30:1999-2003. [Google Scholar | PubMed]
- 8.Moon NH, Shin WC, Kim JS, Woo SH, Son SM, Suh KT. Cementless total hip arthroplasty following failed internal fixation for femoral neck and intertrochanteric fractures: A comparative study with 3-13 years’ follow-up of 96 consecutive patients. Injury 2019;50:713-9. [Google Scholar | PubMed]
- 9.Weiss RJ, Kärrholm J, Hailer NP, Beckman MO, Stark A. Salvage of failed trochanteric and subtrochanteric fractures using a distally fixed, modular, uncemented hip revision stem. Acta Orthop 2012;83:488-92. [Google Scholar | PubMed]
- 10.Jin SY, Jin JY, Kim MG, Kim WJ, Yoon TR, Park KS. Cementless total hip arthroplasty for failed treatment of subtrochanteric fracture. BMC Musculoskelet Disord 2021;22:384. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Surgeon-Performed Intraoperative Pericapsular Nerve Group Block in Total Hip Replacement: A Cadaveric Feasibility Study
March 1, 2026 Surgeon-Performed Intraoperative Pericapsular Nerve Group Block in Total Hip Replacement: A Cadaveric Feasibility Study February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report
February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report January 1, 2026 Total Hip Replacement in Fracture of Hip with Unicameral Bone Cyst – A Rare Case Report
January 1, 2026 Total Hip Replacement in Fracture of Hip with Unicameral Bone Cyst – A Rare Case Report January 1, 2026 Harnessing 3D Printing Technology for Complex Acetabular Reconstruction in Revision Total Hip Arthroplasty: From Childhood Hip Trauma to Customized Modern Solutions
January 1, 2026 Harnessing 3D Printing Technology for Complex Acetabular Reconstruction in Revision Total Hip Arthroplasty: From Childhood Hip Trauma to Customized Modern Solutions