
Robotic assited total knee arthroplasty helps to restore jointline accurately which helps in better range of motion, decrease knee instability and improve natural feel and patient satisfaction and prolong the longevity of the implant .
Dr. Sawankumar Pawar, Department of Orthopedics, Fortis Hiranandani Hospitals Vashi, Navi Mumbai, Maharashtra, India. E-mail: drsawanortho@gmail.com
Introduction: Changes in joint line (JL) position after total knee arthroplasty (TKA) have revealed implant failure, diminished knee function, and altered knee biomechanics. The purpose of this study was to compare the joint line restoration of robotic-assisted TKA (RA-TKA) and conventional TKA (c-TKA).
Materials and Methods: In a prospective cohort study trial, trained fellows performed radiographic analyses on patients receiving RA-TKA (group-1) and c-TKA (group-2) to quantify joint line using the adductor tubercle method. Statistical analysis was used using t-tests, with statistical significance defined as a P < 0.005.
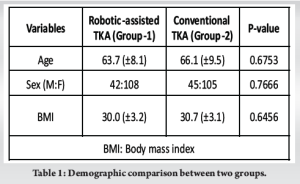
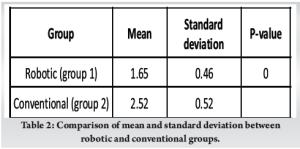
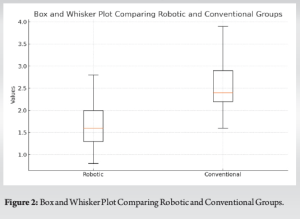
Results: The study contained 150 RA-TKAs and 150 total C-TKAs. Both groups were comparable in demographics such as age, gender, and body mass index. On average, RA-TKAs resulted in a 1.65 ± 0.46 mm shift in the JL position, while C-TKAs resulted in a 2.52 ± 0.52 mm change (P = 0.000). The interclass correlation coefficient between the robotic and conventional groups is around 0.992.
Conclusion: RA-TKA restores the JL position better than C-TKA, which appears to depend on precise planning and ligament balancing, which is attainable with robotic-aided surgery. The clinical relevance of this statistically significant difference requires additional investigation.
Keywords: Total knee arthroplasty, joint line restoration, robotic-assisted, conventional.
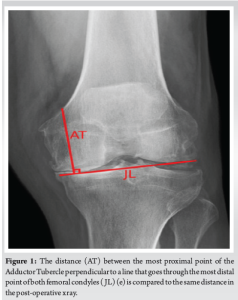
The geometry, alignment, and position that constitute the tibiofemoral joint interaction affect knee function. It is intricately linked with kinematics, kinetics, and balance of the knee joint. The tibiofemoral joint surface is designed to act alongside the ligaments that support the knee [1]. This multifaceted relationship between ligaments and joint interaction remains neglected, posing a significant obstacle to total knee arthroplasty (TKA). TKA remains the widely prevalent procedure for stage 4 arthritis in the knees, and its effectiveness is dependent on its restitution of natural knee kinematics. TKA aims to restore the joint line (JL) [2]. A JL is the point where the proximal tibia meets the distal femur. With extended knees, A JL is normally determined by connecting the furthest distant locations between the medial and lateral femur condyles [3]. According to Luyckx et al. [4], joint stress will change both its form and its position with plastic deformation, even though the interface with the surface is frequently assumed to be a fixed region or point. Second, this JL is primarily depicted with the knee extended from a static perspective. However, it constitutes a dynamic framework, and the motion of the joint will cause the JL to change position in 3D space. Understanding how the knee JL changes position across the entire range of movement requires a grasp of knee kinematics and biomechanics. A change in the JL following TKA affects the biomechanics of the knee by causing changes in the posterior cruciate ligament (PCL) tenseness and mid-flexion laxity [5, 6], as well as anterior knee discomfort, decreased range of movement, patella mal-tracking [4], and patellar tendon impingement, which may have a deleterious impact on post-operative results [7]. Various adaptations to conventional techniques implant designs, and tools are currently being developed to attain the same objectives. Up until this point, numerous computer-assisted and navigational devices have been invented. Navigation has been developed to aid surgeons place implants accurately. Past research indicates that the use of computer-aided methods fails to enhance a surgeon’s skill to re-establish the presumed knee JL in conventional TKA (c-TKA) [8, 9], therefore current improvements include the introduction of robotic-assisted TKA (RA-TKA). This research sought to determine whether RA-TKA was more effective in restoring joint height than TKA performed with a more conventional method. The pre-operative JL orientation will be maintained more effectively with robotic aids than with conventional techniques, according to our hypothesis. (Fig. 1).
The study was conducted at the Department of Orthopedics and Research Center at a tertiary care facility.
Study population
The study included male and female patients with knee arthritis who received primary “robotic-assisted TKA (RA-TKA) or c-TKA” between March 2021 and February 2023.
Study design
This is a randomized, prospective study conducted in the Department of Orthopedics to evaluate the accuracy of joint line restoration using radiographs in patients undergoing robotic TKA versus c-TKA.
Data source
The study investigated patients who had operations between 2021 and 2023. The ethics committee of the institution approved the study.
Patient preference
The study included all patients with primary type 4 Kellegren and Lawrence osteoarthritis who underwent TKA between 2021 and 2023, using either robotic assistance or conventional methods. Patients with infective painful arthritis, arthritis caused by trauma, missed follow-up, and revisions have been excluded from the research protocol. The sample size for the study was calculated based on the global prevalence of knee osteoarthritis over the age of 40 years, which was 22.9%, with a 95% confidence level and 5% margin of error, which came out to be 272. A total of about 300 patients were divided into two groupsA total of about 300 patients divided into two groups: 150 in RA-TKA using “an autonomous Cuvis-Joint Robot” (“Meril Opulent, Republic of Korea”) (Group 1) and 150 in c-TKA (Group 2) using same implant.
Data collection
From the surgical operating data, investigations such as pre-and post-operative imaging, as well as demographic information including age, gender, and body mass index, were gathered. Two separate, skilled fellows in arthroplasty evaluated pre- and post-operative images for the JL calculation. The operational team did not include an independent observer. The adductor tubercle method [10, 11] was used to measure the height of the JL with the ImageJ software. This technique required measuring the height of the JL from the adductor tubercle in a line perpendicular to a line connecting the farthest points of both femoral condyles. After RA-TKA and C-, these measures were compared to ascertain how JL’s position changed. A successful JL restoration occurs when the distance between the new femoral component and the original JL is no more than 2 mm. This measurement is employed because radiographic and anatomical examinations have demonstrated that cartilage made of hyaline within the condyles of the femur can be gauged up to 2 mm in thickness [12, 13]. Since the cartilage itself is not visible on radiographs, the femoral component should be positioned up to 2 mm. The variations between pre- and post-operative JL positions were identified.
Statistics
The data were originally produced and collected with Microsoft Excel. The data analysis had been carried out with “Epi info (Version 7.2; CDC, Atlanta).” The qualitative variables are expressed in percentages. The Kolmogorov-Smirnov test was used to evaluate the ordinality concerning the data set. Numerical data were presented using the average and deviation from the mean. An independent sample t-test was used to assess whether there was a significant difference between the two means. The difference between the two proportions was analyzed using either the “Fisher’s Exact test or the Chi-squared test.” In every two-tailed analysis, the significance level was set at 0.05. Intra- and inter-observer variability were evaluated through an “intra-class correlation test.”
The trial included a total of 300 patients who were randomly divided into two groups of 150 each. The characteristics of the two groups appeared to be alike in terms of their demographics. The average age of patients who undergo robotic surgery is 61.7 years, while those who have conventional joint replacement surgery are typically 59.9 years old. The difference in age between the two groups is not statistically significant (P > 0.05). The population was predominately female in both categories (72% vs. 70%) (Table 1).
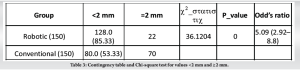
When Group 1 patients underwent RA-TKA compared to Group 2 patients who received conventional measurement, Group 2 had more femoral component distalization. In Group 1, femoral component distalization was 1.65 ± 0.46, but in Group 2, it was 2.52 ± 0.52 (P = 0.000) (Table 2 and Fig. 2). Display the average variance in JL s before and after surgery. Based on (Table 3), it was found that patients in Group 1 had a greater chance of having femoral components positioned within 2 mm of the JL compared to patients in Group 2. Specifically, (85.33%) of patients in Group 1 met this criterion, while only (53.33%) of patients in Group 2 did. The robotic and conventional groups had an interclass correlation coefficient of around 0.992 (Table 4).
The current research found that RA-TKA maintains a better JL position compared to C-TKA on average. According to our findings, the total number of TKA with the JL distalized differed significantly between RA-TKA and C-TKA. Although employing conventional methods resulted in a greater number of distal variations where the JL location moved in excess of 2 mm, the changes are statistically significant. Vaidya [14] reported that joint line was accurately restored with RA-TKA and patellofemoral kinematics improved when in comparison with c-TKA, which supports our results demonstrating RA-TKA contributes to enhanced JL preservation. In a randomized investigation of 60 patients, Liow et al. [15] discovered a decrease in joint-line outliers in comparison with c-TKA. Popat et al. [16] conducted a study; the study discovered that RA-TKA is more accurate in restoring the JL position and posterior offset when compared to traditional methods. Jawhar et al. [8] adopted the measuring method reported by Snider and Macdonald [17]. The mean variation in the JL position was observed to be 0.6 mm. The JL height for c-TKA and robotic-assisted TKA was identical. The utilization of a measuring tool with a precision of 1 mm by the authors may have led to inaccuracies. Babazadeh et al. [9] published the findings of a randomized controlled trial with a smaller population. They employed a computerized navigation system (Ci System, Depuy) without imaging for guidance and found no notable changes in JL positioning compared to c-TKA. According to Herry et al. [18], RA-UKA allowed for more precise JL restoration in unicondylar knee arthroplasty when compared to conventional UKA (“1.4 ± 2.6 mm vs. 4.7 ± 2.4 mm”; P < 0.005). According to the current research, c-TKA distalizes the knee distally by 2.52 mm, while RA-TKA repositions the JL to within 1.6 mm of the original knee. Nevertheless, more research is needed to determine whether the 0.92 mm variation in JL height across c-TKA and RA-TKA results in alteration in the clinical outcomes of knee biomechanics and flexion of the knee. Every innovative operative technology in TKA aims to assist the surgeon in correctly executing an intended plan, which may result in superior clinical results and implant durability. Although the findings are statistically significant for JL preservation, their therapeutic relevance must be examined in future studies. Analyzing patients in follow-up studies for range of motion of the knee, balance, alignment, patella tracking, and occurrence of anterior knee pain in both groups could help determine the scientific importance.
Limitation of study
First, the clinical results of patients undergoing robotic versus conventional surgery were not examined. Patients should be followed for a longer period to gain an improved understanding of their clinical outcomes. Second, CT is a highly reliable measurement method although exposing patients to excessive radiation is not justified [19]. A recent study demonstrated high inter-observer reliability for radiological readings. Third, this study did not compare the effectiveness of robotically assisted TKA to c-TKA in terms of duration of operation or cost-benefit assessment.
Our study found that using the cuvis robotic system in TKA leads to a precise anatomical restoration of the JL more accurately when compared with the c-TKA technique. To validate its durability and sustainability, this group needs to be tracked over an extended length of time.
For orthopaedic arthroplasty surgeons, achieving precise joint line restoration is critical in total knee arthroplasty. Robotic-assisted techniques can enhance alignment accuracy, potentially improving functional outcomes, patient satisfaction, and implant longevity compared to conventional methods.
References
- 1.Van Rossom S, Wesseling M, Smith CR, Thelen DG, Vanwanseele B, Dieter VA, et al. The influence of knee joint geometry and alignment on the tibiofemoral load distribution: A computational study. Knee 2019;26:813-23. [Google Scholar]
- 2.Varacallo M, Luo TD, Mabrouk A, Johanson NA. Total Knee Arthroplasty Techniques. In: StatPearls. Treasure Island: StatPearls Publishing; 2024. [Google Scholar]
- 3.Maderbacher G, Keshmiri A, Schaumburger J, Springorum HR, Zeman F, Grifka J, et al. Accuracy of bony landmarks for restoring the natural joint line in revision knee surgery: An MRI study. Int Orthop 2014;38:1173-81. [Google Scholar]
- 4.Luyckx T, Didden K, Vandenneucker H, Labey L, Innocenti B, Bellemans J. Is there a biomechanical explanation for anterior knee pain in patients with patella alta?: Influence of patellar height on patellofemoral contact force, contact area and contact pressure. J Bone Joint Surg Br 2009;91:344-50. [Google Scholar]
- 5.Koshire S, Mohanty SS, Keny SA, Rai AK, Rathod TN, Kamble P. The influence of joint line restoration on functional outcome after primary total knee arthroplasty: A prospective study. J Clin Orthop Trauma 2022;34:102023. [Google Scholar]
- 6.Cozzarelli NF, DeSimone CA, D’Amore T, Sherman MB, Lonner JH. Joint line position change in primary total knee arthroplasty: A radiographic analysis comparing conventional and robotic techniques. Int Orthop 2024;48:1023-30. [Google Scholar]
- 7.Van Lieshout WA, Valkering KP, Koenraadt KL, Van Etten-Jamaludin FS, Kerkhoffs, GM, Van Geenen RC. The negative effect of joint line elevation after total knee arthroplasty on outcome. Knee Surg Sports Traumatol Arthrosc 2019;27:1477-86. [Google Scholar]
- 8.Jawhar A, Shah V, Sohoni S, Scharf HP. Joint line changes after primary total knee arthroplasty: Navigated versus non-navigated. Knee Surg Sports Traumatol 2013;21:2355-62. [Google Scholar]
- 9.Babazadeh S, Dowsey MM, Swan JD, Stoney JD, Choong PF. Joint line position correlates with function after primary total knee replacement: A randomised controlled trial comparing conventional and computer-assisted surgery. J Bone Joint Surg Br 2011;93:1223-31. [Google Scholar]
- 10.Iacono F, Lo Presti M, Bruni D, Raspugli GF, Bignozzi S, Sharma B, et al. The adductor tubercle: A reliable landmark for analysing the level of the femorotibial joint line. Knee Surg Sports Traumatol Arthrosc 2013;21:2725-9. [Google Scholar]
- 11.Negrín R, Duboy J, Reyes NO, Barahona M, Iñiguez M, Infante C, et al. Robotic-assisted unicompartmental knee arthroplasty optimizes joint line restitution better than conventional surgery. J Exp Orthop 2020;7:94. [Google Scholar]
- 12.Adam C, Eckstein F, Milz S, Putz R. The distribution of cartilage thickness within the joints of the lower limb of elderly individuals. J Anat 1998;193:203-14. [Google Scholar]
- 13.Shah RF, Martinez AM, Pedoia V, Majumdar S, Vail TP, Bini SA. Variation in the thickness of knee cartilage. The use of a novel machine learning algorithm for cartilage segmentation of magnetic resonance images. J Arthroplasty 2019;34:2210-5. [Google Scholar]
- 14.Vaidya NV, Deshpande AN, Panjwani T, Patil R, Jaysingani T, Patil P. Robotic-assisted TKA leads to a better prosthesis alignment and a better joint line restoration as compared to conventional TKA: A prospective randomized controlled trial. Knee Surg Sports Traumatol Arthrosc 2022;30:621-6. [Google Scholar]
- 15.Liow MH, Xia Z, Wong MK, Tay KJ, Yeo SJ, Chin PL. Robot-assisted total knee arthroplasty accurately restores the joint line and mechanical axis. A prospective randomised study. J Arthroplasty 2014;29:2373-7. [Google Scholar]
- 16.Popat R, Albelooshi A, Mahapatra P, Bollars P, Ettinger M, Jennings S, et al. Improved joint line and posterior offset restoration in primary total knee replacement using a robotic-assisted surgical technique: An international multi-centre retrospective analysis of matched cohorts. PLoS One 2022;17:e0272722. [Google Scholar]
- 17.Snider MG, Macdonald SJ. The influence of the posterior cruciate ligament and component design on joint line position after primary total knee arthroplasty. J Arthroplasty 2009;24:1093-8. [Google Scholar]
- 18.Herry Y, Batailler C, Lording T, Servien E, Neyret P, Lustig S. Improved joint-line restitution in unicompartmental knee arthroplasty using a robotic-assisted surgical technique. Int Orthop 2017;41:2265-71. [Google Scholar]
- 19.Ponzio DY, Lonner JH. Preoperative mapping in unicompartmental knee arthroplasty using computed tomography scans is associated with radiation exposure and carries high cost. J Arthroplasty 2015;30:964-7. [Google Scholar]








