
To emphasize the importance of assessing the intra-operative findings in revision TKR and appropriate management.
Dr. Yogadeepan Dhakshinamurthi, Dr. Muthus Super Speciality Orthopaedic Hospital, Coimbatore, Tamil Nadu, India. E-mail: yogadeepan5992@gmail.com
Introduction: Revision total knee replacements are very common now a days. Most common causes include early total knee replacement and increased life expectancy. Proper pre-operative planning and assessment are crucial for the appropriate management of revision cases.
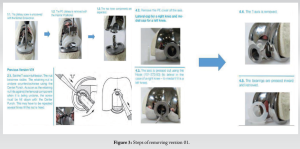
Case Report: An 83-year-old gentleman came with a history of right knee pain and instability for past 1 year. He underwent bilateral TKR 20 years back, after which he underwent two revisions for his right knee 5 and 10 years following the first surgery. Intraoperatively, femoral and tibial components were found stable, and only poly wear was noted with hinge breakage and cement mantle interposition; hence, only hinge revision was done.
Conclusion: Not all cases of revision need complete component replacement. Addressing intraoperative findings and appropriate management prevents complications.
Keywords: Revision TKR, hinje knee, polywear, cement mantle, varus instability.
Revising the primary total knee replacement is always a challenging procedure. Understanding the cause of failure of primary surgery is important. Managing the bone defect, choice of revision implant, and handling the osteoporotic bone are important considerations regarding the revision surgery. Thorough clinical examination, previous medical history, post-operative mobilization status, and range of movements following primary surgery have to be analyzed.
An 83-old-year gentleman from Bahrain came with a history of right knee pain and instability for the past 1 year. He has a history of bilateral knee TKR 20 years back. He had 2 revisions for his right knee following 5 and 10 years after primary surgery. Details and causes of previous surgeries are not known and records are not available. Clinical examination shows that the gentleman was walking with limping with the help of cane. Clinically, varus instability was demonstrated. Blood investigations were normal, and no signs of infection clinically. Neurovascular status was normal. Pre-operative X-ray showed long stem revision TKR prosthesis with hinje breakage and varus instability (Fig. 1). Bone is very osteoporotic and has multiple metaphyseal screws in the tibial area. 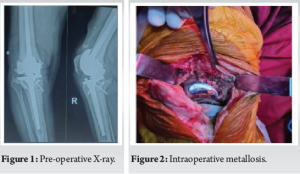
We contacted the Bahrain implant registry and we came to know that it was version 01 German LINK prosthesis, which was available only till July 2015. Now, only version 02 is available. We came to know that version 01 is exchangeable to version 02.
Technique
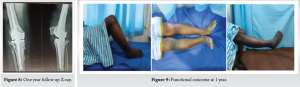
We have done proper pre-operative planning and arranged cement removal set, total custom prostheses, and bush exchange instruments and implants. Intra-operatively after opening, we have noted severe metallosis, and femur and tibial components were found stable, and only poly wear was noted medially ;hence, the knee went for varus. Both femur and tibial components were found stable, and hence, we decided to exchange only the hinge from version 01 to version 02. Extensive metallosis was present throughout the joint (Fig. 2). Steps of femoving the components of version 01 were obtained from the company (Fig. 3).
Multiple sequential intraoperative steps of removal of version 01 were demonstrated below (Fig. 4a-k). We encountered difficulty in full flexion of the knee to remove the retaining pin femur due to soft tissue contracture. Hence, we removed the posterior capsule and other soft tissues and achieved the required flexion and removed the retaining pin. After removing the bearings, we found out that a wafer of cement mantle was found to be impinging inside it, which would have acted as a third body wear, causing poly wear.

The steps of assembling version 2 are shown in Fig. 5. Multiple sequential intraoperative steps of assembling version 02 were demonstrated from Fig. 6a-e. After complete assembly, the knee range of movements was found to be 0–110°, and no varus or valgus instability was noted. The patient was mobilized the next day following the check X-ray with full weight-bearingwalker support and was discharged after 2 weeks after suture removal (Fig. 7). Patient started to walk without support after 2 months. The patient was under regular visit and no pain or implant loosening and have good functional ROM during 1-year follow-up (Fig. 8 and 9).


The number of revisions in total knee arthroplasty (TKA) is increasing because of steady increase in the number of TKA procedures [1-3]. The main reasons for TKA revision are aseptic loosening, infection, and periprosthetic fracture with component loosening [4]. Revision TKA usually requires the use of more constrained implants like hinged prosthesis. They are the most constrained types of implants. They are subjected to high stress at the bone implant surface over a long period of time, which is usually responsible for most of the failures. Nowadays, many modifications of hinge prosthesis like rotating platforms came. Barrack et al. study showed that the use of rotating hinje prosthesis had good functional and radiological outcomes [5]. However, in some rare neurological diseases, rotating hinje is not usually preferred as it is necessary to prevent the movement to only flexion extension [6]. Sanguineti et al. study of 45 rotating Endomodel hinje prosthesis had good outcomes [7]. Now a days, advancements in bone reconstructions using sleeves or cones are extensively used [8-10]. However, in many cases, there is presence of persistent instability at the metaphyseal junction even after reconstruction because of lack of soft tissues and ligaments. Because of all these, hinje prosthesis is a viable option for salvageable cases even though it has many complications which were mainly due to local risk and not due to implant itself [11,12]. Indications for a rotating hinge or pure hinge implant in primary TKA include collateral ligament insufficiency, severe varus, or valgus deformity (>20°) with extensive soft-tissue release, extensive bone loss, including insertions of collateral ligaments, gross flexion-extension gap imbalance, ankylosis, and hyperlaxity. The differential diagnosis in our patient can be infection, aseptic loosening, polywear of the hinge, mechanical loosening of hinge, or break in hinge articulation. Patient general condition, comorbid status, and functional outcomes of the surgery are to be considered primarily. Things to be considered before surgery were which company prosthesis, type and model of prosthesis, how to remove cement, how to handle paper thin cortex as patient underwent multiple revisions. Although the follow-up and survival of hinged system are not as good as compared to the primary system, these implants play a major role in cases of severe bone deficiency, severe osteoporotic bones, and ligamentous insufficiency. The presence of pre-operative instability before the revision requires that it be characterized with X-rays under stress to determine whether there is mediolateral or anteroposterior instability. It is recommended to have a hinged implant available in the operating room when this instability is identified. Periprosthetic fractures and fractures with loosened implants are the main indications for hinged system in very old fragile bone. However, in our case, only polywear of the hinge was noted, and hence, the knee went for varus we exchanged version 01 to version 02 and it was found to be stable. To our knowledge, cases of revision of only hinge in revision TKR have not been reported yet, and ours is the first case getting reported.
Rotating hinge survival is much better than pure hinge. Rotating hinge has thin poly bushings and tibial poly insert. Poly wear of these bushings may cause early wear of the hinge mechanism. Missed cement pieces may act as third body wear, causing early loosening. Meticulous surgical steps are mandatory to change version 01 rotating hinge to version 02. Flexion of the T axis of more than 90° is very essential step to remove the retaining nut. Not all revisions need full-blown component exchange and cement extraction. Proper planning and adequate instruments backup needs to be arranged.
The main content in this case report is the meticulous and extensive steps and techniques of changing the hinje from version 01 to version 02 system. An additional challenge is the osteoporotic bone, which has a high chance of iatrogenic fracture during removal, and how we overcame it. Not all revision needs component exchange, and proper pre-operative planning and intra-operative observation are very much helpful in revision cases and in preventing complications.
References
- 1.Kurtz SM, Ong KL, Schmier J, Mowat F, Saleh K, Dybvik E, et al. Future clinical and economic impact of revision total hip and knee arthroplasty. J Bone Joint Surg Am 2007;89:144-51. [Google Scholar]
- 2.National Joint Registry. National Joint Registry for England and Wales. 14th Annual Report. National Joint Registry; 2017. Available from: https://www.njrreportd.org.uk/portals/0/pdfdownloads/njr%2014th%20annual%20report%202017.pdf [Last accessed on 2018 Sep 24]. [Google Scholar]
- 3.Losina E, Thornhill TS, Rome BN, Wright J, Katz JN. The dramatic increase in total knee replacement utilization rates in the United States cannot be fully explained by growth in population size and the obesity epidemic. J Bone Joint Surg Am 2012;94:201-7. [Google Scholar]
- 4.Postler A, Lützner C, Beyer F, Tille E, Lützner J. Analysis of total knee arthroplasty revision causes. BMC Musculoskelet Disord 2018;19:55. [Google Scholar]
- 5.Barrack RL, Lyons TR, Ingraham RQ, Johnson JC. The use of a modular rotating hinge component in salvage revision total knee arthroplasty. J Arthroplasty 2000;15:158-66. [Google Scholar]
- 6.Prasad A, Donovan R, Ramachandran M, Dawson-Bowling S, Millington S, Bhumbra R, et al. Outcome of total knee arthroplasty in patients with poliomyelitis: A systematic review. EFORT Open Rev 2018;3:358-62. [Google Scholar]
- 7.Sanguineti F, Mangano T, Formica M, Franchin F. Total knee arthroplasty with rotating-hinge endo-model prosthesis: Clinical results in complex primary and revision surgery. Arch Orthop Trauma Surg 2014;134:1601-7. [Google Scholar]
- 8.Falzan A, Bohwmik-Stoker M, Alipit V, Kirk AE, Krebs VE, Harwin SF et al. Development and verification of novel porous titanium metaphyseal cones for revision total knee arthroplasty. J Arthroplasty 2017;32:1946-53. [Google Scholar]
- 9.Bugler KE, Maheshwari R, Ahmed I, Brenkel IJ, Walmsley PJ. Metaphyseal sleeves for revision total knee arthroplasty: Good short-term outcomes. J Arthroplasty 2015;30:1990-4. [Google Scholar]
- 10.Barnett SL, Mayer RR, Gondusky JS, Choi L, Patel JJ, Gorab RS. Use of stepped porous titanium metaphyseal sleeves for tibial defects in revision total knee arthroplasty: Short term results. J Arthroplasty 2014;29:1219-24. [Google Scholar]
- 11.Springer BD, Sim FH, Hanssen AD, Lewallen DG. The modular segmental kinematic rotating hinge for non neoplasic limb salvage. Clin Orthop Relat Res 2004;421:181-7. [Google Scholar]
- 12.Korim MT, Esler CN, Reddy VR, Ashford RU. A systematic review of endoprosthetic replacement for non-tumour indications around the knee joint. Knee 2013;20:367-75. [Google Scholar]






