Cost-effective medial meniscus posterior root tear (MMPRT) repair using a handmade all-suture anchor
Dr Hitendra G Patil, Department of Orthopaedics, Pimprikar Hospital, Chowk No 5, Govind Nagar, Nashik, Maharashtra, India. E-mail: drhitendrapatil@gmail.com
Introduction: The arthroscopic transtibial pullout technique is popular option for the medial meniscus posterior root tear repair. The technique involves passing sutures through the meniscus tissue at the root, creating a bone tunnel, and bringing the sutures through the bone tunnel on the anteromedial surface of the tibia. The suture threads are then tied over anteromedial surface of tibia with the help of various fixation devices to secure the root at its footprint.
Surgical Technique: A sleeve of no 5 ethibond is used to fix the pull-out threads to anteromedial surface of tibia achieving secure and stable fixation of the posterior root to anatomical footprint with option of adjusting the tension.
Conclusion: HitPat’s modified all-suture technique is a cost-effective solution to medial meniscus posterior root repair with the distinct advantage of less prominent hardware and the option to adjust the tension in repair.
Keywords: Medial meniscus root tear, no 5 ethibond sleeve, all-suture technique.
The medial and lateral meniscus are a pair of semilunar fibrocartilages that plays a vital role if the functioning of knee joint [1]. Around 10–28% of all meniscal tears are at or near the attachment sites [2, 3]. Historically overlooked medial meniscus posterior root tear (MMPRT) is now recognized as significant pathology [4]. If left untreated, they cause meniscal extrusion, increasing contact pressures across the condyles, ultimately progressing to secondary osteoarthritis [5]. Although the ideal surgical technique for MMPRT repair is still debatable, the transtibial pullout technique is popular, with promising results reported [6, 7]. We present our transtibial pullout repair (TPR) technique using sutures only.
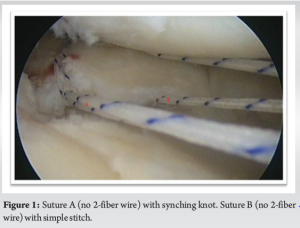
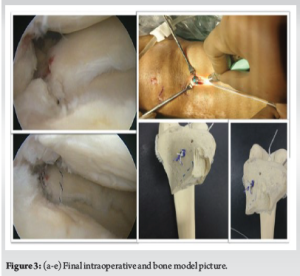
The patient is supine under spinal anesthesia with lateral thigh support applied at the level of the tourniquet. Standard arthroscopy portals are created for meniscus repair. Pie crusting of the medial collateral ligament is done to prevent the scuffing of the cartilage. With the help of an available suture passing device, a loop of no-2 fiber wire is passed through the most medial portion of the posterior horn of the medial meniscus, creating a synching knot (Suture A). A single strand of another no-2 fiber wire (Suture B) is passed 5 mm medial to the first suture through a healthy portion of the medial meniscus (Fig. 1) thus, allowing the insertion of Duncan’s sliding knot. A bone tunnel is created at the footprint of the MMPRT using an anterior cruciate ligament jig fixed at 50° from the anteromedial aspect of the tibia. The cartilage around the tunnel is removed to expose the subchondral bone. A retrograde beath pin with a suture loop is inserted through the tibia in the knee joint. The loop, along with the sutures from the medial meniscus, is pulled through the tunnel, avoiding a soft-tissue bridge to the anteromedial surface of the tibia. With the help of No. 5 ethibond, a sleeve is created around all four strands, as shown in (Fig. 2a) [8]. Duncan’s sliding non-locking knot is created with the help of two strands of suture B (Fig. 2b). By pulling the post, Duncan’s knot slides toward the anterior tibial surface, which pushes the ethibond sleeve toward the anterior surface of the tibia, creating a crumpled knot that obliterates the tibial tunnel with ethibond, which does not allow Duncan’s knot to advance further (Fig. 2c). As one tightens the knot, the posterior most end of the meniscus gets fixed at the anatomical footprint of the root. Further tension can be adjusted by pulling the post of Duncan’s knot with the help of knot pusher simultaneously viewing arthroscopically in 30° of knee flexion, and the knot is locked and secured using further half hitches (Fig. 2d). Both strands of suture A are pulled out to adjust the tension at the footprint of the root further, and multiple half hitches are put (Fig. 2e). Excess threads of sutures A and B are cut. Finally, the medial meniscus root is fixed to the anatomic footprint (Fig. 3).

Two main techniques for repairing the meniscal posterior root tear are the suture anchor and TPR techniques. Jiang et al., in their systematic review of multiple databases, found no consensus on biomechanical superiority between TPR and suture anchor repair if done anatomically [9]. TPR technique involves passing sutures through meniscus tissue at the root, creating a bone tunnel, bringing the sutures through the bone tunnel on the anterior surface of the tibia, and tying the threads on the anteromedial surface of the tibia, thus attaching the meniscus root to the anatomical footprint in the joint [10]. The options to fix pullout sutures to anteromedial tibial surface are buttons (titanium/peek), suture post, or tensionable anchor. Suture posts or first-generation buttons like suture discs are cost-effective but have the issue of prominent hardware. Second-generation buttons have sleek designs, which solve the problem of prominent hardware, but it increases the cost. Tensionable anchors have the advantage of adjusting the tension in final repair, but the cost is still a concern. Joshi et al. described a cost-effective technique for making all-suture anchors [8]. They used all-suture anchors placed near the medial meniscus posterior root footprint through the bone tunnel, and the meniscus was tied to the anatomical footprint. This technique lacks the advantage of adjusting the final tension at the repair side. We modified the “make and use suture anchor” (Joshi et al.) and repaired the meniscus using the TPR method. HitPat’s modified all-suture technique is simple. It addresses the issue of prominent hardware and also has the advantage of adjusting the final tension in the repair without adding cost to the treatment.
HitPat’s modified all-suture technique is a cost-effective solution to medial meniscus posterior root repair. It has the distinct advantage of less prominent hardware and the option to adjust the tension during repair.
Cost-effective medial meniscus posterior root repair can be done without using metal/peek button or tensionable anchor.
References
- 1.Moulton SG, Bhatia S, Civitarese DM, Frank RM, Dean CS, LaPrade RF. Surgical techniques and outcomes of repairing meniscal radial tears: A systematic review. Arthroscopy 2016;32:1919-25. [Google Scholar]
- 2.Bin SI, Kim JM, Shin SJ. Radial tears of the posterior horn of the medial meniscus. Arthroscopy 2004;20:373-8. [Google Scholar]
- 3.Ozkoc G, Circi E, Gonc U, Irgit K, Pourbagher A, Tandogan RN. Radial tears in the root of the posterior horn of the medial meniscus. Knee Surg Sports Traumatol Arthrosc 2008;16:849-54. [Google Scholar]
- 4.LaPrade CM, Jansson KS, Dornan G, Smith SD, Wijdicks CA, LaPrade RF. Altered tibiofemoral contact mechanics due to lateral meniscus posterior horn root avulsions and radial tears can be restored with in situ pull-out suture repairs. J Bone Joint Surg Am 2014;96:471-9. [Google Scholar]
- 5.Hein CN, Deperio JG, Ehrensberger MT, Marzo JM. Effects of medial meniscal posterior horn avulsion and repair on meniscal displacement. Knee 2011;18:189-92. [Google Scholar]
- 6.Moon HS, Choi CH, Jung M, Lee DY, Hong SP, Kim SH. Early surgical repair of medial meniscus posterior root tear minimizes the progression of meniscal extrusion: 2-Year follow-up of clinical and radiographic parameters after arthroscopic transtibial pull-out repair. Am J Sports Med 2020;48:2692-702. [Google Scholar]
- 7.Krych AJ, Boos AM, Lamba A, Smith PA. Satisfactory clinical outcome, complications, and provisional results of meniscus centralization with medial meniscus root repair for the extruded medial meniscus at mean 2-year follow-up. Arthroscopy 2024;40:1578-87. [Google Scholar]
- 8.Joshi A, Basukala B, Sharma R, Singh N, Bista R, Pradhan I. “Make and use” all suture anchor-a cost-effective method of making an all-suture anchor. Arthrosc Tech 2023;12:e1311-8. [Google Scholar]
- 9.Jiang EX, Everhart JS, Abouljoud M, Kirven JC, Magnussen RA, Kaeding CC, et al. Biomechanical properties of posterior meniscal root repairs: A systematic review. Arthroscopy 2019;35:2189-206.e2. [Google Scholar]
- 10.Chen HY, Lin KY. Arthroscopic transtibial pull-out repair for meniscal posterior root tear: The slip knot technique. Arthrosc Tech 2022;11:e209-15. [Google Scholar]