This case highlights the importance of considering myxoma in the differential diagnosis of dorsal hand swellings, despite its rarity. The successful surgical excision and follow-up in a 34-year-old female with a myxoma on the dorsum of the hand underscore the need for early diagnosis and treatment to prevent potential complications.
Dr. Rui Manuel Henriques Valente Marques de Sousa, Unidade Local de Saúde de Viseu Dão-Lafoes – Av. Rei Dom Duarte, 3504-509 Viseu, Portugal. E-mail: ruivmsousa@gmail.com
Introduction: Myxoma is a rare benign tumor of primitive connective tissue, most commonly found in the heart. It can also occur in other soft tissues, such as the skin, muscles, jawbones, and near joints. Myxomas of the upper limb, particularly in the hand, are extremely rare. This case adds to the limited literature on hand myxomas, providing insights into its clinical presentation, diagnosis, and management. Apart from this case, only two more cases of myxoma with similar topography have been described.
Case Report: A 34-year-old Caucasian female with no prior significant medical history presented with a non-painful, gradually enlarging mass on the dorsum of her right hand, which had been growing for a year and a half. The lesion was oval and mobile, without involvement of the extensor tendons. Imaging revealed a well-defined nodular lesion in the subcutaneous fat layer of the dorsomedial hand, suggestive of a myxoid-type lesion. A surgical excision was performed and a histopathological examination confirmed the diagnosis of myxoma, describing a 3 cm nodular fragment of compact, soft, mucinous tissues. At the 2-month follow-up, the patient had a fully healed wound with complete finger and wrist mobility, preserved muscular strength, and no pain. At the 1-year follow-up, no recurrence of the lesion was observed.
Conclusion: This case emphasizes the need to consider myxoma in the differential diagnosis of dorsal hand swellings. Early diagnosis and complete surgical excision are essential to prevent recurrence and potential complications. The successful management and follow-up in this patient illustrate the potential for favorable outcomes with appropriate treatment. This case report provides valuable information to the literature, enhancing our understanding of the clinical presentation and management of rare myxomas in the hand and highlighting the importance of awareness and thorough evaluation in managing unusual soft-tissue tumors.
Keywords: Myxoma, hand tumor, soft-tissue tumor, surgical excision.
A myxoma is a rare benign myxoid tumor of primitive connective tissue. Its designation was first used by Virchow to describe certain tumors that were grossly and microscopically analogous to umbilical tissue. It is the most common primary tumor of the heart in adults [1, 2], but can also occur in other soft-tissue locations, most commonly in the skin, muscles (especially of the lower limb), jawbones, or in the vicinity of the joints (juxta-articular) [3, 4]. Myxomas of the upper limb are extremely rare and those in the hand are even rarer [3]. We present the case of a 34-year-old female with a myxoma of the dorsal aspect of the hand.
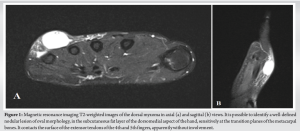
We present the case of a 34-year-old Caucasian female with no prior significant medical history, who presented with a non-painful gradually enlarging mass on the dorsum of the right hand, which had been growing for a year and a half. The lesion was oval and mobile, without interference or mobility upon movement of the extensor tendons. A magnetic resonance imaging was performed, revealing a well-defined nodular lesion of oval morphology, in the subcutaneous fat layer of the dorsomedial aspect of the hand, sensitively at the transition planes of the metacarpal bones, contacting the surface of the extensor tendons of the 4th and 5th fingers, apparently without involvement, and suggestive of a myxoid type lesion (Fig. 1). Subsequently, the patient was referred for surgical en bloc excision of the lesion (Fig. 2).
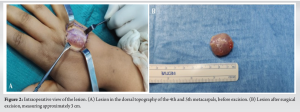
A 4 cm dorsal curvilinear incision over the lesion was carefully planned and marked to provide optimal exposure while preserving key anatomical landmarks, including the extensor tendons of the 4th and 5th fingers, given the lesion’s close proximity. Dissection was meticulously performed in a layer-by-layer approach progressing through the skin, subcutaneous tissue, and fascial plane to enhance visualization and minimize tissue damage. Special attention was given to identifying and preserving the extensor tendons and avoiding injury to the dorsal branches of the ulnar and radial nerves by employing blunt dissection near the tendon sheaths. No intra-operative extensor tendon or sagittal band involvement was observed. As a myxoid lesion was expected, gentle handling with atraumatic instruments and fine dissecting scissors was required due to its soft and mucinous nature and to avoid fragmentation. Clear separation planes from surrounding tissues were identified, allowing for the lesion’s complete and intact excision. After thorough hemostasis, the surgical site was then closed in layers, with interrupted sutures applied to the skin, to minimize the risk of hematoma or seroma formation and to promote optimal healing. Histopathological examination confirmed the diagnosis of myxoma, describing a nodular fragment of 3 cm, apparently limited and non-encapsulated, and consisting of compact, soft, mucinous tissues.
At the 2-month follow-up, the patient presented with a fully healed wound, complete finger and wrist mobility, fully preserved muscular strength, and no pain. At the 1-year follow-up, no recurrence of the lesion was observed.
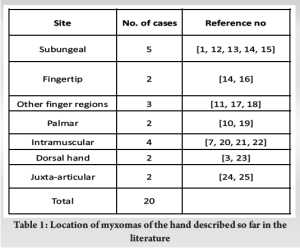
About < 1% of all upper-limb tumors occur in the hand [5], therefore, tumors at this body site are not well-studied [6]. Myxomas are rare, benign, soft-tissue tumors formed by the accumulation of mucinous tissue. They are most commonly found in the heart (incidence of 0.5–1 case per 106 individuals per year) [2]. Myxomas can be classified into various types based on their tissue of origin (bone or soft tissue) [7]. Originating from the bone itself, myxomas are predominantly found in the jaw, whereas periosteal myxomas typically occur in the long bones (e.g., the femur) [8]. The juxta-articular types are most commonly found in larger joints, such as the knee [9], shoulder, elbow, foot, and ankle, and only rarely in the hand and wrist [10]. Al-Qattan classified myxomas according to their origins and thought that they were subungual, bony, or from soft tissues [11]. On the hand, various sites have been described, including the subungual [1, 12, 13, 14, 15], fingertip [14, 16], other finger regions [11, 17, 18], palmar [10, 19], intramuscular [7, 20, 21, 22], dorsal [3, 23], and juxta-articular [24, 25] (Table 1).
Myxomas clinically present as a slowly enlarging mass and do not necessarily provoke pain [26, 27]. They present as cystic formations [27] of soft or friable consistency, white to yellow, ranging from 2 to 6 cm in size [24]. Due to the anatomical features of the hand, patients tend to notice a hand mass early in the course of the disorder. Consequently, individuals with hand myxoma typically seek medical attention within the 1st year of the condition and present with a mass of small to medium size [3].
Treatment of a myxoma is complete surgical excision. Continued follow-up is important because the local recurrence rate after resection is high [25]. Incomplete resection may be the reason for this recurrence rate [9]. Although classified as benign lesions, myxomas can be locally destructive and thus cause symptoms such as pain or nerve palsy [28, 29, 30]. In the setting of local tissue destruction, one must consider malignancy in the differential diagnosis [24].
Myxoma of the hand is an extremely rare condition. To our best knowledge, only two more cases of myxoma with similar topography have been described, one from the intermetacarpal space [23] and the other purely dorsal [3]. Despite its rarity, it should be considered part of the differential diagnosis of dorsal hand swelling.
The successful management of this rare entity, as represented in this case, emphasizes the need for early and accurate identification of myxomas to prevent recurrence and potential complications. This report provides valuable insights into the clinical presentation, imaging characteristics, and management strategies for hand myxomas, contributing to the limited literature on this rare condition. It underscores the significance of thorough evaluation and awareness in managing uncommon soft-tissue tumors, offering guidance for clinicians who may encounter similar cases.
References
- 1.Sanusi ID. Subungual myxoma. Arch Dermatol 1982;118:612-4. [Google Scholar]
- 2.Keeling IM, Oberwalder P, Anelli-Monti M, Schuchlenz H, Demel U, Tilz GP, et al. Cardiac myxomas: 24 years of experience in 49 patients. Eur J Cardiothorac Surg 2002;22:971-7. [Google Scholar]
- 3.Nasır S, Altuntaş S, Karagöz MA, Aydın MA, Kapucuoğlu N. Myxoma of the dorsal hand. J Plast Surg Hand Surg 2013;47:78-80. [Google Scholar]
- 4.Forcucci JA, Bruner ET, Smith MT. Benign soft tissue lesions that may mimic malignancy. Semin Diagn Pathol 2016;33:50-9. [Google Scholar]
- 5.Muramatsu K, Ihara K, Yoshida K, Tominaga Y, Hashimoto T, Taguchi T. Musculoskeletal sarcomas in the forearm and hand: Standard treatment and microsurgical reconstruction for limb salvage. Anticancer Res 2013;33:4175-82. [Google Scholar]
- 6.Nicholson S, Milner RH, Ragbir M. Soft tissue sarcoma of the hand and wrist: Epidemiology and management challenges. J Hand Microsurg 2018;10:86-92. [Google Scholar]
- 7.Al-Qattan MM, El-Shayeb A, Rasool MN. An intramuscular myxoma of the hand. Hand Surg 2004;9:97-9. [Google Scholar]
- 8.Chacha PB, Tan KK. Periosteal myxoma of the femur. A case report. J Bone Joint Surg Am 1972;54:1091-4. [Google Scholar]
- 9.Ozcanli H, Ozenci AM, Gurer EI, Tuzuner S. Juxta-articular myxoma of the wrist: A case report. J Hand Surg Am 2005;30:165-7. [Google Scholar]
- 10.Keoshian LA, Lower RR, Eversole SL, Nelsen TS. Myxoma of the palm; a case report. Plast Reconstr Surg 1964;34:66-70. [Google Scholar]
- 11.Al-Qattan MM. Myxoma of the hand. J Hand Surg Br 1996;21:690-2. [Google Scholar]
- 12.Rozmaryn LM, Schwartz AM. Treatment of subungual myxoma preserving the nail matrix: A case report. J Hand Surg Am 1998;23:178-80. [Google Scholar]
- 13.Gourdin FW, Lang PG Jr. Cylindrical deformity of the nail plate secondary to subungual myxoma. J Am Acad Dermatol 1996;35:846-8. [Google Scholar]
- 14.Winke BM, Blair WF, Benda JA. Myxomas in the fingertips. Clin Orthop Relat Res 1988;237:271-4. [Google Scholar]
- 15.Kaehr D, Klug MS. Subungual myxoma. J Hand Surg Am 1986;11:73-6. [Google Scholar]
- 16.Hill TL, Jones BE, Park KH. Myxoma of the skin of a finger. J Am Acad Dermatol 1990;22:343-5. [Google Scholar]
- 17.Rakoto-Ratsimba HN, Razafimahandry HJ, Tsiaviry P, Rakototiana A, Rakotozafy G. Digital myxoma. A case report and review of the literature. Chir Main 2005;24:270-2. [Google Scholar]
- 18.Stout AP. Myxoma, the tumor of primitive mesenchyme. Ann Surg 1948;127:706-19. [Google Scholar]
- 19.Tolhurst DE. Myxoma of the palm. Hand 1973;5:260-2. [Google Scholar]
- 20.Firouzbakht PK, Israel JS, Christie BM, Rao VK. Rare hypothenar myxoma causing ulnar neuropathy: Histopathology and treatment pearls. Plast Reconstr Surg Glob Open 2018;6:e1806. [Google Scholar]
- 21.Tolis KE, Raptis KG, Zafeiris CP, Antonopoulos DK, Spyridonos SG. A rare intramuscular myxoma of the hypothenar. J Musculoskelet Neuronal Interact 2015;15:372-4. [Google Scholar]
- 22.Enzinger FM. Intramuscular myxoma; a review and follow-up study of 34 cases. Am J Clin Pathol 1965;43:104-13. [Google Scholar]
- 23.Fletcher JW, Watson HK, Weinzweig J. Recurrent myxoma of the hand. J Hand Surg Am 2000;25:772-5. [Google Scholar]
- 24.Irving A, Gwynne-Jones D, Osipov V, Nicholson M. Juxta-articular myxoma of the palm. J Surg Case Rep 2012;2012:12. [Google Scholar]
- 25.Claudi C, Andreisek G, Vrugt B, Ganser J. A Juxta-articular myxoma of the thumb. J Hand Surg Glob Online 2020;2:171-4. [Google Scholar]
- 26.Murphey MD, McRae GA, Fanburg-Smith JC, Temple HT, Levine AM, Aboulafia AJ. Imaging of soft-tissue myxoma with emphasis on CT and MR and comparison of radiologic and pathologic findings. Radiology 2002;225:215-24. [Google Scholar]
- 27.Meis JM, Enzinger FM. Juxta-articular myxoma: A clinical and pathologic study of 65 cases. Hum Pathol 1992;23:639-46. [Google Scholar]
- 28.Yano K, Yoneda A, Ohta Y, Kaneshiro Y. Carpal tunnel syndrome caused by a juxta-articular myxoma: A case report. J Hand Surg Asian Pac Vol 2024;29:152-5. [Google Scholar]
- 29.Sakai H, Fujioka H, Makino T. Posterior interosseous nerve palsy caused by a myxoma. J Hand Surg Eur Vol 2008;33:84-5. [Google Scholar]
- 30.Valer A, Carrera L, Ramirez G. Myxoma causing paralysis of the posterior interosseous nerve. Acta Orthop Belg 1993;59:423-5. [Google Scholar]