
This case report confirms the theory that tendon rupture is caused by systemic disease. In this case, chronic kidney disease causes inflammatory changes that alter the structure of the tendon. Early surgical treatment offers promising outcomes.
Dr. Collen Sandile Nkosi, Department Orthopaedic Surgery, Chris Hani Baragwanath Academic Hospital, 26 Chris Hani Rd, Diepkloof 319-Iq, Johannesburg, 1864, South Africa. E-mail: drcsnkosi@gmail.com
Introduction: Simultaneous quadriceps tendons with contralateral patellar tendon ruptures are extremely uncommon. We present a rare case of a male with bilateral simultaneous knee extensor mechanism injuries following a fall who is known to have a systemic end-stage medical disease.
Case Report: A 36-year-old African male is known to have end-stage renal disease following bilateral congenital kidney disease. He receives hemodialysis 3 times a week at our academic hospital renal unit. He presented at our casualty with bilateral knee pains, knee swelling, and an inability to mobilize both legs. He had an inability to extend his knee, a palpable gap along the patella tendon on the left, and a palpable gap in the right quadriceps tendon. We performed plain radiographs to confirm the clinical diagnosis.
Conclusion: We experienced a simultaneous rupture of the quadriceps tendon with the contralateral patellar tendon in a 36-year-old with chronic renal failure on hemodialysis. Surgical repair was performed earlier, and he achieved good functional outcomes.
Keywords: Chronic kidney disease, tendons, patella, quadriceps, orthopaedics.
Simultaneous quadriceps tendons with contralateral patellar tendon ruptures (PTR) are extremely uncommon [1]. According to Emre et al., there is a gradual rise in cases with chronic renal failure experiencing simultaneous rupture of the patellar and contralateral quadriceps tendons [2]. Patients over 40 years old are more likely to experience isolated quadriceps tendon ruptures (QTR), whereas patients of younger ages get isolated PTRs [3]. It usually occurs spontaneously in patients with chronic medical conditions due to the poor tendon blood supply and degeneration of collagen fibrils [1]. The chronic medical treatment for this ailment includes gout, rheumatoid arthritis, systemic lupus erythematosus, hyperparathyroidism, chronic kidney failure, connective tissue disorders that are inherited, prolonged corticosteroid treatment, and fluoroquinolone medications [1,2,4]. We present a 36-year-old male with bilateral simultaneous knee extensor mechanism injuries following a fall who is known to have a systemic end-stage medical disease.
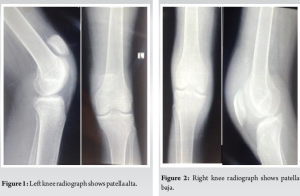
A 36-year-old African male is known to have end-stage renal disease following bilateral congenital kidney disease. He receives hemodialysis 3 times a week at the Academic Hospital renal unit. He presented at our casualty with bilateral knee pains, knee swelling, and an inability to mobilize both legs. It happened while he was walking; he tripped over a stone and fell onto both knees. He has been receiving hemodialysis for his chronic renal disease since 2017, as well as Erythropoietin D 4000s/c weekly and 1α Vitamin D 0.25 mg PO daily. He was a young male, well-kept, presented in a wheelchair, and had normal vital signs. He had a perm catheter going into the right subclavian vein. On knee examination, he had no wounds, bilateral knee swelling, or anterior knee tenderness with palpable right suprapatellar and left infrapatellar gaps. His knees were in 90° flexion with an inability to extend the knees actively; he was unable to hold the knees in extension when passively moved. He was neurovascular intact on both legs. On plain radiographs of the bilateral knees, the left knee showed a patella alta both on anteroposterior and lateral views, and the right knee showed a patella baja on anteroposterior and lateral views (Fig. 1 and 2).
He was then planned for open surgical repair. The left patella tendon rupture was at the insertion site of the inferior pole; it was debrided and fixed with suture anchors from Stryker.
The right knee QTR was at the insertion site of the superior pole; it was debrided and fixed with suture anchors from Stryker. The patient was placed on an above-knee back slab and applied an extension in the theatre. For the left knee with patella tendon injury at 2 weeks, sutures were removed, and range of motion was started as tolerated by the physiotherapist on a brace. For the right knee with quadriceps tendon injury at 2 weeks, sutures were removed, and the back slab was kept for another 2 weeks as per our hospital protocol. At 6 months, his range of motion was 0–95° on the right knee and 0–100° on the left knee.
In 1983, Loehr and Welsh reported a case of simultaneous ruptures of the right patellar tendon with contralateral left quadriceps tendon in a 27-year-old patient suffering from chronic renal failure brought on by lifting, and it appears that this was the first case in English literature of this nature, based on our review of the literature [5]. The knee extensor tendons are infrequently injured, and QTR is more common than PTR, with an incidence of more than 1.37/100,000 people per year for QTRs and <1/100,000 people per year for PTRs [1]. We managed to identify 17 previously reported cases in the English literature review of simultaneous rupture of the quadriceps tendon with contralateral patellar tendon from 1983 to December 2023. Males were impacted at a higher rate than females, with 88.2% (15 cases) compared to 11.8% (two cases). These simultaneous PTR with contralateral QTR affect patients aged 42.3 (21–67 years). Of the 17 cases, seven injuries occurred to the left QTR, seven to the right PTR, 10 to the right QTR, and 10 to the left PTR. Unfortunately, hand dominance was not documented in these cases [1-17]. Our case had a right QTR with a contralateral left PTR. The concurrent rupture of the knee extensor mechanism is primarily caused by systemic chronic medical disorders, primarily chronic renal failure. We identified 12 cases with chronic renal failure, four healthy patients, and one case with systemic lupus erythematous [1-17]. The mechanism of injury was spontaneous in seven cases with CRF followed by a fall, and in healthy cases, the mechanism of injury was mainly trauma [1-17]. The exact mechanism responsible for the simultaneous rupture of the quadriceps tendon with the contralateral patellar tendon is still unknown. The increased number of cases could be associated with the increased use of hemodialysis, which has increased the lifespan and quality of life in patients with chronic renal failure. Although it is still debatable, bilateral QTR is now thought to be a complex disorder predominantly caused by secondary hyperparathyroidism from prolonged hemodialysis treatment rather than just connective tissue elastosis [18]. Bilateral PTR has three reported theories in the literature. The first theory has to do with systemic disease, which causes inflammatory changes that alter the structure of the tendon; the second theory is an injectable steroid that affects collagen production and comprises vascular supply, thereby weakening the tendon; and the third theory is that chronic repetitive microtrauma leads to rupture [19]. The diagnosis of simultaneous rupture of the quadriceps tendon with the contralateral patellar tendon is based mainly on history, physical examination, and imaging. Plain radiographs were used to confirm our diagnosis in this study. To mitigate the possibility of misdiagnosis of partial tears, the literature suggests utilizing ultrasound and magnetic resonance imaging [10,12]. The management of the simultaneous rupture of the quadriceps tendon with the contralateral patellar tendon has progressed over the past decades through multiple surgical procedures techniques such as end-to-end repair, transosseous tendon repair, suture anchor tendon repair, and additional augmentation [1-17]. Regarding outcomes, these patients do have a good range of motion, as seen by the 17 case reports and our case [1-17].
We experienced a simultaneous rupture of the quadriceps tendon with the contralateral patellar tendon in a 36-year-old male with chronic renal failure on hemodialysis. Surgical repair was performed earlier, and he achieved good functional outcomes.
Simultaneous rupture of the quadriceps tendon and contralateral patellar tendon is extremely rare and requires swift surgical procedures, followed by rehabilitation to enhance the patient’s functional results.
References
- 1.Bennis A, Youssef J, Elghoul N, Zine A, Tanane M, Jaafar A, et al. Simultaneous rupture of the quadriceps tendon with contralateral patellar tendon: A rare combination. Int J Orthop 2020;6:930-2. [Google Scholar | PubMed]
- 2.Emre B, Cornelis V, Alper KY, Ozkan K, Onder K. Simultaneous quadriceps and contralateral patellar tendon ruptures in a patient with chronic renal failure following electric shock; A case report and review of the literature. Rom J Orthop Surg Traumatol 2019;2:9-17. [Google Scholar | PubMed]
- 3.Muratli HH, Çelebi L, Hapa O, Biçimoğlu A. Simultaneous rupture of the quadriceps tendon and contralateral patellar tendon in a patient with chronic renal failure. J Orthop Sci 2005;10:227-32. [Google Scholar | PubMed]
- 4.Radaideh AM, Audat ZA, Sunallah AW, Bani-Younes HM, Obeidat O. A simultaneous rupture of the patellar tendon and the contralateral quadriceps tendon in a patient with chronic renal failure undergoing long-term hemodialysis. Med Arch 2021;75:317-20. [Google Scholar | PubMed]
- 5.Loehr J, Welsh RP. Spontaneous rupture of the quadriceps tendon and patellar ligament during treatment for chronic renal failure. Can Med Assoc J 1983;129:254-6. [Google Scholar | PubMed]
- 6.Grecomoro G, Camarda L, Martorana U. Simultaneous chronic rupture of quadriceps tendon and contra-lateral patellar tendon in a patient affected by tertiary hyperparatiroidism. J Orthop Traumatol 2008;9:159-62. [Google Scholar | PubMed]
- 7.Branco FR, Gonçalves WA. Simultaneous rupture of the patellar and contralateral quadriceps tendons in a nephropathy patient. Acta Ortop Bras 2023;31:e267719. [Google Scholar | PubMed]
- 8.Jalgaonkar A, Rafee A, Haddo O, Sarkar S. Simultaneous rupture of the quadriceps tendon with contralateral patellar tendon rupture: An unusual case and a review of the literature. Eur J Orthop Surg Traumatol 2008;18:69-71. [Google Scholar | PubMed]
- 9.Rysavy M, Wozniak A, Arun KP. Spontaneous and simultaneous quadriceps and patella tendon rupture in a patient on chronic hemodialysis. Orthopedics 2005;28:603-5. [Google Scholar | PubMed]
- 10.Chen CM, Chu P, Huang GS, Wang SJ, Wu SS. Spontaneous rupture of the patellar and contralateral quadriceps tendons associated with secondary hyperparathyroidism in a patient receiving long-term dialysis. J Formos Med Assoc 2006;105:941-5. [Google Scholar | PubMed]
- 11.Karadimas EJ, Kotzamitelos D, Kakagia DD, Hatziyiannakis A. Spontaneous rupture of the patellar tendon and the contralateral quadriceps tendon, associated with lupus erythematosus: Analysis of the literature. Case Rep Orthop 2011;2011:569363. [Google Scholar | PubMed]
- 12.Zabala IL, Pulido MC, Popescu D, Fernández-Valencia JA. Simultaneous and spontaneous rupture of patellar tendon and contralateral quadriceps tendon in a patient with tertiary hyperparathyroidism: A case report. Int J Case Rep Images 2012;3:13-6. [Google Scholar | PubMed]
- 13.Al-Jawad B, Al-Ammari N. Simultaneous rupture of the quadriceps tendon with contralateral patellar tendon in a 53-year-old male. MOJ Orthop Rheumatol 2014;1:121-3. [Google Scholar | PubMed]
- 14.Caruso G, Gambuti E, Spadoni E, Massari L. Simultaneous rupture of quadriceps tendon and contra-lateral patellar tendon: A case report and review of literature. Curr Health Sci J 2022;48:454-6. [Google Scholar | PubMed]
- 15.Rogers A, Rix S, Kulkarni R. Simultaneous rupture of a patellar tendon and contralateral quadriceps tendon in a healthy individual. Orthopedics 2003;26:817-8. [Google Scholar | PubMed]
- 16.Kumar S, Rachakatla N, Kerin C, Kumar R. Simultaneous traumatic rupture of the patellar tendon and the contralateral quadriceps tendon in a healthy individual. BMC Case Rep 2010;2010:bcr0620103057. [Google Scholar | PubMed]
- 17.Munshi NI, Mbubaegbu CE. Simultaneous rupture of the quadriceps tendon with contralateral rupture of the patellar tendon in an otherwise healthy athlete. Br J Sports Med 1996;30:177-8. [Google Scholar | PubMed]
- 18.Wu W, Wang C, Ruan J, Wang H, Huang Y, Zheng W, et al. Simultaneous spontaneous bilateral quadriceps tendon rupture with secondary hyperparathyroidism in a patient receiving hemodialysis: A case report. Medicine (Baltimore) 2019;98:e14809. [Google Scholar | PubMed]
- 19.Taylor BC, Tancev A, Fowler T. Bilateral patellar tendon rupture at different sites without predisposing systemic disease or steroid use. Iowa Orthop J 2009;29:100-4. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Aneurysmal Bone Cyst-cloaked Codman’s Tumor in the Patella: Case Report of an Easily Misdiagnosed Entity
January 1, 2026 Aneurysmal Bone Cyst-cloaked Codman’s Tumor in the Patella: Case Report of an Easily Misdiagnosed Entity June 1, 2025 Elevating Orthopaedic Care through Materiovigilance
June 1, 2025 Elevating Orthopaedic Care through Materiovigilance June 1, 2025 Ilizarov-Assisted Reduction of Femoral Condyle Locked in Tibial Fracture: A Case Report
June 1, 2025 Ilizarov-Assisted Reduction of Femoral Condyle Locked in Tibial Fracture: A Case Report May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain
May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain