
Delayed PIN palsy can develop in patients with old, unreduced Monteggia fractures, highlighting the need for a thorough medical history and treatment focused on relieving nerve compression while preserving the patient’s adapted function.
Dr. Fernando Macedo, Department of Orthopaedic Surgery, ULS Alto Ave, Guimarães, Portugal R. dos Cutileiros 114, Creixomil, Guimarães, Portugal. E-mail address: fe.rm@live.com.pt
Introduction: While acute posterior interosseous nerve (PIN) palsy is a recognized complication of Monteggia fractures, delayed or tardy PIN palsy due to persistent radial head dislocation is exceedingly uncommon.
Case Report: We describe a case of tardy PIN palsy 29 years after an unreduced Monteggia fracture, Bado type I.
Conclusion: While rare, delayed PIN palsy can occur in patients with old, unreduced Monteggia fractures. This underscores the need for a thorough medical history to detect potential causes, as long-standing injuries may eventually present symptoms. Treatment should target the underlying compression from the fracture dislocation while preserving the patient’s adapted function.
Keywords: Tardy, delayed, posterior interosseus nerve palsy, Monteggia, radial head dislocation.
While acute posterior interosseous nerve (PIN) palsy is a recognized complication of Monteggia fractures, delayed or tardy PIN palsy due to persistent radial head dislocation is exceedingly uncommon [1-3]. The initial case of tardy PIN palsy linked to a Monteggia fracture was documented by Lichter and Jacobsen [4], with only a handful of additional cases reported in English literature since then [5-8]. The patient was informed that data concerning the case would be submitted for publication, and she provided consent.
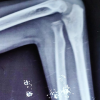
A 57-year-old female presented with a 1-year history of progressive right-hand weakness. The patient worked as a seamstress in a textile factory and had recently increased her workload before the onset of symptoms. Her initial symptom was difficulty extending her fingers while performing routine tasks at home. The patient recalled a right elbow fracture from a car accident approximately 29 years earlier, which had been treated conservatively. On examination, the patient demonstrated complete loss of extension in her wrist, thumb, and fingers. Her elbow’s range of motion was restricted from 30° of extension to 140° of flexion, a condition unchanged since her initial injury. Sensation in the superficial radial nerve distribution remained intact. Electromyography confirmed PIN palsy. Radiographs showed that the radial head was dislocated anteriorly, consistent with a Bado type I Monteggia fracture (Fig. 1).

A magnetic resonance imaging scan revealed that the dislocated radial head was pressing on the PIN, and a swollen area existed from the compression area to just before the nerve entered the supinator muscle.
We performed a Henry approach on the right elbow. The anterior cutaneous nerve of the forearm was isolated. The interval between the brachioradialis and biceps brachii was developed. A thorough neurolysis was carried out, resulting in the complete release of Frohse’s arcade. A neuroma of the PIN was found just anterior to the radial head (Fig. 2). An anterior capsulotomy and radial head excision were performed since the PIN was under tension due to anterior head dislocation and subsequent compression.

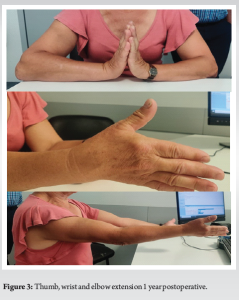
Postoperatively, a 2-week immobilization using a plaster cast was performed, and afterward, a dynamic radial nerve splint was used for 4 months. The patient was referred to physical therapy, which was initiated 1 month after the procedure. At 1 month postoperatively, there was a residual improvement in active finger extension. By 4 months, the patient had regained significant mobility in the fifth to the third finger. At 7 months, she had recovered thumb and index finger mobility. A notable improvement was evident 1 year after the operation, with complete recovery of the thumb, finger, and wrist extensions (Fig. 3). Furthermore, there was a modest improvement regarding elbow mobility, with only the last 10° of extension remaining limited.
Non-traumatic PIN palsy can result from supinator muscle compression, benign tumors, rheumatoid arthritis, neuralgic amyotrophy, repetitive motion injuries, or residual radial head dislocation in Monteggia fractures [9-11]. To the authors’ knowledge, only six cases of delayed PIN palsy related to an old, unreduced radial head in Monteggia fractures have been reported in the English literature [4-8]. Table 1 summarizes the case presentation.
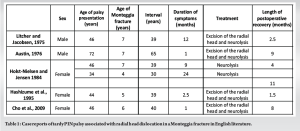
In all previous reports, Monteggia fractures occurred during childhood, with a mean age of 6 years (range 4–7 years). Our case represents the first occurrence in which the initial fracture occurred in adulthood, at 28 years of age. The patient has no recollection of any other previous upper limb trauma, and she affirms that she had normal elbow mobility before this incident. The average period between the initial fracture and the onset of neurological symptoms in previous cases was 42 years, with a mean age of presentation at 48 years old and an average recovery period after surgery of 6 months. In our case, the PIN palsy manifested at 57 years old, with an interval of 29 years between the initial Monteggia fracture, considerably shorter than previously reported cases. This is likely due to the later occurrence of the initial fracture. Curiously, symptoms started so many years after the initial injury. We hypothesize that the development of scar tissue or changes in the position of the PIN relative to surrounding structures may have gradually increased the pressure on the nerve over time, leading to the onset of symptoms many years after the original injury. Repeated microtrauma or overuse may also be associated with symptoms onset. Both Litcher and Austin reported lesions involving manual laborer patients. In the two cases reported by Holst–Nielsen, the first patient was a housewife who had just started working as a maid before the onset of symptoms, and the second one was a secretary who had changed to babysitting. In the case reported by Cho et al., the patient was a housewife whose symptoms developed after strenuous work helping her family prepare for a wedding. In our case, the patient reported increased effort in her job-related tasks and household chores. It is possible, thus, that trauma resulting from strenuous physical activity can exacerbate the formation of scar tissue, aggravate degenerative changes, or cause edema in the affected area, which can increase the pressure on the PIN and trigger the onset of symptoms. For surgical treatment, we opted for radial head excision combined with neurolysis, as the radial head contributed to ongoing nerve compression and deformity. Neurolysis alone may be appropriate when compression arises primarily from soft tissue, as seen in both cases reported by Holst–Nielsen, where the Frohse ligament was the primary cause. In all other reported cases, radial head excision was performed.
Although these lesions are rare, we must be vigilant and maintain a high index of suspicion for the possibility of delayed PIN palsy in patients with old, unreduced Monteggia fractures. It emphasizes the crucial importance of a thorough and accurate medical history to identify potential causes, as injuries that have persisted asymptomatically over the years may manifest symptoms over time.
The treatment of tardy PIN palsy due to persistent radial head dislocation should address the underlying cause, specifically the compression resulting from an old fracture dislocation, all the while ensuring that the function of a patient who has already adapted to this condition is not compromised.
References
- 1.Jessing P. Monteggia lesions and their complicating nerve damage. Acta Orthop Scand 1975;46:601-9. [Google Scholar | PubMed]
- 2.Stein F, Grabias SL, Deffer PA. Nerve injuries complicating monteggia lesions. J Bone Joint Surg Am 1971;53:1432-6. [Google Scholar | PubMed]
- 3.Spinner M, Freundlich BD, Teicher J. Posterior interosseous nerve palsy as a complication of monteggia fractures in children. Clin Orthop Relat Res 1968;58:141-5. [Google Scholar | PubMed]
- 4.Lichter RL, Jacobsen T. Tardy palsy of the posterior interosseous nerve with a monteggia fracture. J Bone Joint Surg Am 1975;57:124-5. [Google Scholar | PubMed]
- 5.Austin R. Tardy palsy of the radial nerve from a monteggia fracture. Injury 1976;7:202-4. [Google Scholar | PubMed]
- 6.Holst-Nielsen F, Jensen V. Tardy posterior interosseous nerve palsy as a result of an unreduced radial head dislocation in monteggia fractures: A report of two cases. J Hand Surg Am 1984;9:572-5. [Google Scholar | PubMed]
- 7.Hashizume H, Nishida K, Yamamoto K, Hirooka T, Inoue H. Delayed posterior interosseous nerve palsy. J Hand Surg Br Eur Vol 1995;20:655-7. [Google Scholar | PubMed]
- 8.Cho CH, Lee KJ, Min BW. Tardy posterior interosseous nerve palsy resulting from residual dislocation of the radial head in a monteggia fracture: A case report. J Med Case Rep 2009;3:9300. [Google Scholar | PubMed]
- 9.Hashizume H, Nishida K, Nanba Y, Shigeyama Y, Inoue H, Morito Y. Non-traumatic paralysis of the posterior interosseous nerve. J Bone Joint Surg Br 1996;78:771-6. [Google Scholar | PubMed]
- 10.Kowalski B, Zarkadis NJ, Harris M, Scanaliato J, Dunn J. Posterior interosseous nerve palsy in rheumatoid arthritis: A systematic review. Hand (N Y) 2024 Jun 22: doi: 10.1177/15589447241260766. [Google Scholar | PubMed | CrossRef]
- 11.Rojc B, Golob P. Posterior interosseous nerve lesion due to lipoma. Review of the literature and rare case presentation. Radiol Oncol 2024;58:480-5. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Neglected Monteggia Fracture-Dislocation in an 8-Year-Old Child with Posterior Interosseous Nerve Palsy: A Case Report
October 1, 2025 Neglected Monteggia Fracture-Dislocation in an 8-Year-Old Child with Posterior Interosseous Nerve Palsy: A Case Report October 1, 2025 Failed Primary Fixation of Monteggia Fractures – A Case Series
October 1, 2025 Failed Primary Fixation of Monteggia Fractures – A Case Series June 1, 2025 Sculpting Solutions: 3D-Printed Models Transform Osteotomy Planning in Monteggia Fractures
June 1, 2025 Sculpting Solutions: 3D-Printed Models Transform Osteotomy Planning in Monteggia Fractures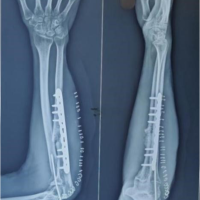 May 10, 2023 Old Monteggia Fracture-Dislocation Treated with Plating and Forearm Fascial Slip Annular Ligament Reconstruction: A Rare Method of Treatment and Review of Literature
May 10, 2023 Old Monteggia Fracture-Dislocation Treated with Plating and Forearm Fascial Slip Annular Ligament Reconstruction: A Rare Method of Treatment and Review of Literature