
Efficient management of spondyloptosis with reduction technique.
Dr. Sukhmin Singh, Department of Orthopaedics, AIIMS Bilaspur, Bilaspur, Himachal Pradesh, India. E-mail: Sukhmin92@gmail.com
Introduction: Acute traumatic spondyloptosis is a rare injury resulting from high-energy impactcreating an unstable injury requiring surgical reconstruction and stabilization. Although rarely described in clinical practice this injury needs to be emphasized due to severe clinical manifestations and poor prognosis due to associated neurological injury.
Case Report: In this paper, we report a rare case of traumatic lumbar spondyloptosis at L2-L3 and the reduction technique. Case was managed with minimally invasive technique with percutaneous fixation and reduction.
Conclusion: These types of rare injuries are a real challenge to manage properly and as the literature is scarce, this marks the further difficulty in their proper management.
Keywords: Spondyloptosis, minimally invasive surgery, percutaneous fixation.
Acute traumatic spondyloptosis (ATS) is a rare injury resulting from high-energy impact creating an unstable injury which requires surgical reconstruction and stabilization. Although rarely described in clinical practice this injury needs to be emphasized due to severe clinical manifestations and poor prognosis. Purpose of this study is to provide the educational insight into the management of the rare injury along with reduction technique for managing such spinal dislocations.
A 34-year-old female presented to us in emergency department with trauma due to a landslide and complaint of multiple injuries over her back and pelvis. Patient had laceration over the sacrum with open sacral fracture along with right sided acetabular central fracture dislocation and ATS of L2/L3 which was diagnosed on X-ray and computed tomography (CT) scan of pelvis and spine (Fig. 1). Focused assessment with sonography in trauma showed no free fluid in pericardial, Morrison’s pouch, supra pubic and splenorenal pouch. On neurological examination, the patient had paraplegia with bowel and bladder involvement. Sensations were intact till L4. Patient had a heart rate of 100/min and blood pressure of 80/60. Four units of whole blood were transfused along with one liter of ringer lactate. Patient was stabilized and blood pressure of 110/80 along with heart rate of 78 was achieved. The severity of spinal injury was graded according to American spinal injury association (ASIA) grading scale as grade A. CT angiography showed no trauma to vessels in front of lumbar spine and in pelvis.

Operative procedure and follow-up
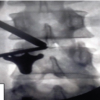
After stabilizing the patient, debridement of the open sacral fracture was done; however, we could not get anesthesia clearance to fix spine simultaneously. As the patient was kept Prone for the debridement with blood pressure on the lower side, simultaneous spine fixation was not possible due to deterioration while debriding the patient. Hence, the decision was taken to stabilize the patient first as the chances of neurological recovery were very less but saving the life of the patient was priority. The patient was again taken for surgery 2 days after the debridement of sacral wound for spine fixation. However, to decrease the blood loss during surgery and duration of the surgery, it was decided to do MIS posterior instrumentation of spine from L1 to L5 without fusion. We were able to achieve reduction at L2-L3 preoperatively by hyperextension and traction maneuver in supine position (Fig. 2); however, the reduction was partially lost when patient was positioned in prone during surgery. Pedicle screws were inserted two levels above and below L3 under C-ARM guidance. Reduction was easily achieved using reduction screws (Figs. 3 and 4). No CSF leak was encountered during surgery. Her pelvic injury was treated conservatively.

Six months postoperatively, the patient regained bowel sensation but there was no motor recovery in bilateral lower limbs. At 1 year follow-up, the status is the same.
The most common site of spondyloptosis is the lumbosacral joint. This type of injury is extremely rare. Thoracolumbar vertebral fractures most commonly affect thoracolumbar junction (T11-L2). Spondyloptosis is associated with severe neurological deficit with 80% of cases leading to complete paraplegia. Usually, higher energy traumas cause traumatic spondyloptosis with multi system collateral damage where multidisciplinary intervention becomes essential. We searched for strings, lumbar spondyloptosis/traumatic spondyloptosis/spondyloptosis, in PUBMED and found 28 cases of lumbar spondyloptosis reported before our case report. All of those cases along with junctional (lumbosacral and thoracolumbar) spondyloptosis are included in Table 1.


The fractures of bilateral pedicles and posterior elements reduce the threat of cord compromise in patients with spondyloptosis. However, prolonged dislocation may result in stasis of blood flow within the vertebral arteries leading to thrombus formation, and subsequent reduction may restore the blood flow and dislodge thrombus leading to ischemic events. We were able to reduce the dislocation preoperatively by hyperextending the lumbar spine. This was achieved by placing a small bolster below the lower back of the patient in supine position. The patient was taken for spine fixation 2 days after the injury.
Various reduction techniques have been suggested by different authors. Tang et al. [1] reported traumatic lumbosacral spondyloptosis with locked inferior articular process of L5 in a 33 year old man presenting with ASIA grade C which improved to ASIA grade D, 6 months postoperatively. Authors suggest removing the bilateral inferior articular processes if found locked preoperatively on radiology and then perform reduction during surgery. Li et al. [2] have published operative technique to reduce spondylosis in which they stated that operative strategies have usually employed open posterior approaches using distraction between pedicle screws in the sagittal plane and cantilevering anteriorly dislocated vertebrae back into alignment by applying reducers to screw heads, as well as intradiscal distraction with spreaders have also been described. Maneuvers such as manual abdominal pressure have proved effective in selected cases. Corpectomy through either the trans pedicular or thoracotomy route has also been utilized especially if initial reduction maneuvers fail. Despite these strategies, complete realignment could not be achieved in approximately 25% of cases. Transversely oriented rods have been employed for fracture reduction thoracolumbar junction but not in context of spondyloptosis or within the rigid thoracic spine. The technique of multiple horizontal rods placed in parallel to enable additional surgeon recruitment has relatively high success rates of both closed and open reduction of cervical fracture dislocations whether approached anteriorly or posteriorly the same is not true for thoracic dislocations, due to the remoteness of potential proximal and distal fixation points for traction and difficulties directly assessing the thoracic spine from ventrolateral approaches. However, in our case, we used reduction screws and distraction to reduce L2-3 spondyloptosis. Halder et al. [3] reported a case of spondyloptosis at L1-L2 in a 33 year old male patient following a road traffic accident with paraparesis who developed abdominal distension vomiting and gardening on day 4 of injury. Contrast-enhanced computed tomography of abdomen and pelvis revealed tethering of proximal jejunal loop between interface of translated L1-L2 vertebrae and resultant dilation of stomach and duodenum with splenic injury and hemoperitoneum. Patient was managed by doing exploratory laparotomy during which the jejunal loops were successfully freed and resection and anastomosis of the involved segment was done. However, the patient developed septic shock with acute respiratory distress syndrome and succumbed to it on day 14. In our case, we did not find any associated vascular and bowel injury. However, our patient had associated open pelvi-acetabular injury.
ATS of lumbar spine is rare and unstable Injury. About 50% of these patients present with complete neurologic injury. However, the aim of surgery should be to stabilize the spine and to decompress the neural structures as early as possible without risking injury to other vital structures. However, it is also essential to give priority to associated life threatening injuries that need multidisciplinary intervention.
Managing spondyloptosis is challenging as intensive care with comprehensive team of trauma is required. Reducing spondyloptosis is difficult but achievable with proper technique.
References
- 1.Tang T, Liu Y, Cao J, Wu T, He D, Cheng X, et al. Case report: Traumatic lumbosacral spondyloptosis with locked L5 inferior articular process. Front Surg 2023;10:1174169. [Google Scholar | PubMed]
- 2.Li Y, Huang M, Manzano G. Traumatic dorsal spondyloptosis of upper thoracic spine: Case report and novel open reduction technique. Br J Neurosurg 2020;8:1-5.doi: 10.1080/02688697.2020.1828277. [Google Scholar | PubMed | CrossRef]
- 3.Halder K, Sarjare D, Anand A. Small bowel obstruction secondary to traumatic incarceration between vertebral fracture: A case report in a tertiary care hospital in central india. Indian J Radiol Imaging 2023;33:249-52. [Google Scholar | PubMed]
- 4.Akesen B, Mutlu M, Kara K, Aydinli U. Traumatic lumbosacral spondyloptosis: A case report and review of the literature. Global Spine J 2014;4:59-62. [Google Scholar | PubMed]
- 5.Amesiya R, Orwotho N, Nyati M, Mugarura R, Mwaka ES. Traumatic spondyloptosis of the lumbar spine: A case report. J Med Case Rep 2014;8:453. [Google Scholar | PubMed]
- 6.Baek DH, Choi BW, Kim JW. Treatment of traumatic lumbosacral spondyloptosis combined with unstable pelvic ring injury. J Orthop Sci 2015;20:776-80. [Google Scholar | PubMed]
- 7.Barwar N. Post-traumatic L4-L5 spondyloptosis with cauda equina syndrome: A case report. Trauma Case Rep 2021;33:100475. [Google Scholar | PubMed]
- 8.Bellew MP, Bartholomew BJ. Dramatic neurological recovery with delayed correction of traumatic lumbar spondyloptosis. Case report and review of the literature. J Neurosurg Spine 2007;6:606-10. [Google Scholar | PubMed]
- 9.Braithwaite J, Gruber J, Fakhoury J, Katsigiorigis G, Grewal K. Acute traumatic spondyloptosis: A case report. Cureus 2023;15:e36457. [Google Scholar | PubMed]
- 10.Cabrera JP, Yankovic W, Luna F, Torche E, Valdes G, Lopez E, et al. Traumatic spondyloptosis of L3 with incomplete neurological involvement: A case report. Trauma Case Rep 2019;24:100248. [Google Scholar | PubMed]
- 11.Cheng L, Qiu C, Liu XY, Sang XG. Treatment strategy on traumatic mid-lumbar spondyloptosis with concomitant multiple injuries: A case report and literature review. Chin J Traumatol 2023;26:33-40. [Google Scholar | PubMed]
- 12.Chandrashekhara SH, Kumar A, Gamanagatti S, Kapoor K, Mukund A, Aggarwal D, et al. Unusual traumatic spondyloptosis causing complete transection of spinal cord. Int Orthop 2011;35:1671-5. [Google Scholar | PubMed]
- 13.Xu F, Tian Z, Fu C, Yao L, Yan M, Zou C, et al. Mid-lumbar traumatic spondyloptosis without neurological deficit: A case report and literature review. Medicine (Baltimore) 2020;99:e19578. [Google Scholar | PubMed]
- 14.Yamaki VN, Morais BA, Brock RS, Paiva WS, De Andrade AF, Teixeira MJ. Traumatic lumbosacral spondyloptosis in a pediatric patient: Case report and literature review. Pediatr Neurosurg 2018;53:263-9. [Google Scholar | PubMed]
- 15.Wangtaphan W, Oo M, Paholpak P, Wang Z, Sakakibara T, Kasai Y. Traumatic lumbosacral spondyloptosis treated five months after injury occurrence: A Case report. Spine (Phila Pa 1976) 2012;37:E1410-4. [Google Scholar | PubMed]
- 16.Garg M, Kumar A, Sawarkar DP, Singh PK, Agarwal D, Kale SS, et al. Traumatic lateral spondyloptosis: Case series. World Neurosurg 2018;113:e166-71. [Google Scholar | PubMed]
- 17.Mishra A, Agrawal D, Gupta D, Sinha S, Satyarthee GD, Singh PK. Traumatic spondyloptosis: A series of 20 patients. J Neurosurg Spine 2015;22:647-52. [Google Scholar | PubMed]
- 18.Zhou TH, Tang X, Xu YQ, Zhu YL. Traumatic spondyloptosis of L4. Spine (Phila Pa 1976) 2010;35:E855-9. [Google Scholar | PubMed]
- 19.Verhelst L, Ackerman P, Meirhaeghe JV. Traumatic posterior lumbosacral spondyloptosis in a six-year-old: A case report and review of the literature. Spine (Phila Pa 1976) 2009;34:E629-34. [Google Scholar | PubMed]
- 20.Jindong Z, Qing L. Traumatic lateral spondyloptosis of L2 with complete neurological deficit: A case report. Trauma Case Rep 2020;29:100339. [Google Scholar | PubMed]
- 21.Yadla S, LeBude B, Tender GC, Sharan AD, Harrop JS, Hilibrand AS, et al. Traumatic spondyloptosis of the thoracolumbar spine. J Neurosurg Spine 2008;9:145-51. [Google Scholar | PubMed]
- 22.Francis T, Steinmetz M, Moore T. Traumatic spondyloptosis of the lumbar spine: Closed reduction and internal fixation. Spine (Phila Pa 1976) 2013;38:E1636-40. [Google Scholar | PubMed]
- 23.Daniels AH, Deodhar AA, Hart RA. Traumatic spondyloptosis resulting from high-energy trauma concurrent with a tonic-clonic seizure. Spine J 2009;9:e1-4. [Google Scholar | PubMed]
- 24.Koruga N, Koruga AS, Hecimovic I, Kondza G, Bakran Z, Zubcic V, et al. Lumbar spondyloptosis after severe polytrauma: A case report. Acta Clin Croat 2020;59:555-9. [Google Scholar | PubMed]
- 25.Goni V, Gopinathan NR, Saini UC, Kantharajanna SB. Traumatic L5 over S1 spondyloptosis without neurological involvement managed nonoperatively: A case report. Chin J Traumatol 2013;16:178-81. [Google Scholar | PubMed]
- 26.Gabel BC, Curtis E, Gonda D, Ciacci J. Traumatic L5 posterolateral spondyloptosis: A case report and review of the literature. Cureus 2015;7:e277. [Google Scholar | PubMed]
- 27.Sandquist L, Paris A, Fahim DK. Definitive single-stage posterior surgical correction of complete traumatic spondyloptosis at the thoracolumbar junction. J Neurosurg Spine 2015;22:653-7. [Google Scholar | PubMed]
- 28.Sekhon LH, Sears W, Lynch JJ. Surgical management of traumatic thoracic spondyloptosis: Review of 2 cases. J Clin Neurosci 2007;14:770-5. [Google Scholar | PubMed]
- 29.Wilkinson JS, Riesberry MA, Mann SA, Fourney DR. Traumatic lateral expulsion of the L-4 vertebral body from the spinal column. J Neurosurg Spine 2011;14:508-12. [Google Scholar | PubMed]
- 30.Kaplan SS, Wright NM, Yundt KD, Lauryssen C. Adjacent fracture-dislocations of the lumbosacral spine: Case report. Neurosurgery 1999;44:1134-7. [Google Scholar | PubMed]
- 31.Hilibrand AS, Urquhart AG, Graziano GP, Hensinger RN. Acute spondylolytic spondylolisthesis. Risk of progression and neurological complications. J Bone Joint Surg Am 1995;77:190-6. [Google Scholar | PubMed]
- 32.Saiki K, Hirabayashi S, Sakai H, Inokuchi K. Traumatic anterior lumbosacral dislocation caused by hyperextension mechanism in preexisting L5 spondylolysis: A case report and a review of literature. J Spinal Disord Tech 2006;19:455-62. [Google Scholar | PubMed]
- 33.Van Savage JG, Dahners LE, Renner JB, Baker CC. Fracture-dislocation of the lumbosacral spine: Case report and review of the literature. J Trauma 1992;33:779-84. [Google Scholar | PubMed]
- 34.Meneghini RM, DeWald CJ. Traumatic posterior spondyloptosis at the lumbosacral junction. A case report. J Bone Joint Surg Am 2003;85:346-50. [Google Scholar | PubMed]
- 35.Stanger JK. Fracture-dislocation of the thoracolumbar spine; with special reference to reduction by open and closed operations. J Bone Joint Surg Am 1947;29:107-18. [Google Scholar | PubMed]
- 36.Abdel-Fattah H, Rizk AH. Complete fracture-dislocation of the lower lumbar spine with spontaneous neurologic decompression. Clin Orthop Relat Res 1990;251:140-3. [Google Scholar | PubMed]
- 37.Chatani K, Yoshioka M, Hase H, Hirasawa Y. Complete anterior fracture-dislocation of the fourth lumbar vertebra. Spine (Phila Pa 1976) 1994;19:726-9. [Google Scholar | PubMed]
- 38.Chen WC. Complete fracture-dislocation of the lumbar spine without paraplegia. Int Orthop 1999;23:355-7. [Google Scholar | PubMed]
- 39.Suomalainen O, Paakkonen M. Fracture dislocation of the lumbar spine without paraplegia. A case report. Acta Orthop Scand 1984;55:466-8. [Google Scholar | PubMed]
- 40.Chavda DV, Brantigan JW. Technique of reduction and internal fixation of thoracolumbar fracture-dislocation using pedicle screws and variable screw placement plates. Orthop Rev 1994;Suppl:25-31. [Google Scholar | PubMed]
- 41.Finkelstein JA, Hu RW, Al-Harby T. Open posterior dislocation of the lumbosacral junction. A case report. Spine (Phila Pa 1976) 1996;21:378-80. [Google Scholar | PubMed]
- 42.Gertzbein SD. Posterior dislocation of the lumbosacral joint: A case report. J Spinal Disord 1990;3:174-8. [Google Scholar | PubMed]
- 43.Cohn SL, Keppler L, Akbarnia BA. Traumatic retrolisthesis of the lumbosacral junction. A case report. Spine (Phila Pa 1976) 1989;14:132-4. [Google Scholar | PubMed]
- 44.Jackson RH, Quisling RG, Day AL. Fracture and complete dislocation of the thoracic or lumbosacral spine: Report of three cases. Neurosurgery 1979;5:250-3. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study
January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study November 1, 2025 Arthroscopic Fixation of an Atraumatic Osteochondral Defect of the Knee: A Case Report
November 1, 2025 Arthroscopic Fixation of an Atraumatic Osteochondral Defect of the Knee: A Case Report June 1, 2025 Intramedullary Fibular Nail Fixation in an Elderly Patient with a Comminuted Weber C Ankle Fracture: A Case Report
June 1, 2025 Intramedullary Fibular Nail Fixation in an Elderly Patient with a Comminuted Weber C Ankle Fracture: A Case Report March 1, 2025 Titanium Elastic Nail System for Middle One-Third Clavicle Fractures: Impact on Functional Recovery
March 1, 2025 Titanium Elastic Nail System for Middle One-Third Clavicle Fractures: Impact on Functional Recovery