
This case highlights the challenges of managing Failed AC joint reconstruction, Proper surgical technique, careful planning, and secure fixation are crucial in ensuring a patient's excellent functional recovery.
Dr. Rahul Patel, Department of Orthopedics, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India. E-mail: rahulpatel1610922@gmail.com
Introduction: Acromioclavicular joint (ACJ) injuries are prevalent among young, active individuals and account for a significant proportion of shoulder girdle and collision sports injuries. The Rockwood classification system categorizes these injuries from Type I to VI, guiding treatment from conservative management to surgical intervention. Despite various surgical techniques, including the Fiber-loop Endobutton method, failure rates, and complications remain a concern, particularly in cases of post-operative instability.
Case Report: A 50-year-old male presented with persistent right shoulder pain and deformity following an initial Type-V ACJ injury from a road traffic accident. The patient had undergone surgical stabilization with a Fiber-loop Endobutton construct. However, 17th days post-surgery, he experienced a recurrence of pain and deformity, with radiographs revealing the failure of the initial repair. Subsequent imaging indicated a mal-positioned Endobutton and potential coracoid blowout, likely due to inadequate drill hole placement. Three weeks later, the patient underwent revision surgery using a double figure-of-8 autogenic loop reconstruction with FiberTape and hamstring tendon graft. The procedure involved removing the failed hardware, drilling new holes in the clavicle, and securing the ACJ with FiberTape and a hamstring graft. The graft was looped around the coracoid and clavicle in a figure-of-8 manner to replicate acromioclavicular ligament anatomy and ensure both horizontal and vertical stability. At 6 weeks, follow-up radiographs demonstrated near-anatomic alignment of the ACJ and coracoclavicular. The patient reported minimal pain and regained a near-full range of motion. By 6 months, while slight radiographic changes were noted, the patient remained asymptomatic with excellent functional outcomes and minimal limitations.
Conclusion: This case highlights the challenges of managing post-operative instability in ACJ injuries. The successful use of a dual figure-of-8 graft technique provides a viable solution for revision surgery, offering satisfactory stability and functional recovery. Further research is needed to optimize salvage techniques for complex cases.
Keywords: Revision acromioclavicular joint surgery, suspension fixation failure, loop endobutton, acromioclavicular joint.
Injuries to the acromioclavicular joint (ACJ) are frequent among young, active individuals and makeup approximately 9% of all shoulder girdle injuries and nearly 40% of all shoulder injuries in collision sports, such as football, hockey, and kabaddi. [1, 2]. The ACJ is crucial for the natural movement of the upper arm, offering multi-directional stability to the shoulder. Thus, any trauma to the ACJ should be well evaluated and treated accordingly else it can leave patients in significant pain and discomfort. The Tossy-Rockwood classification system is the most commonly used classification system, as only plain radiographs are needed to describe the degree of soft tissue involvement and joint dislocation [3]. Scores range from Type I-VI with increasing severity. General consensus exists that Rockwood types I-II should be managed conservatively, while surgical intervention is indicated for Rockwood types IV-VI. Management of Rockwood type III injuries remains controversial. There is no consensus on the best surgical treatment for ACJ injuries that warrant surgical intervention, there are more than 60 techniques being discussed in the literature [4]. However, most surgeons will agree that achieving both horizontal and vertical stability is key to ensuring the best long-term results. Among the various surgical options, the Fiber-loop Endobutton, which employs an open surgical approach for acute ACJ dislocation, has demonstrated effectiveness in replicating coracoclavicular (CC) ligament anatomy, thus providing satisfactory stability. Nevertheless, failure rates for ACJ repair, indicated by recurring dislocations, vary between 16.9% and 25.2% [5]. If complications occur, revision surgery may become necessary. However, instability of the ACJ can be exacerbated by factors such as bone loss at the clavicle and coracoid from prior tunnel placements, hardware removal, and inflammation from multiple procedures, which can further elevate the risk of complications. At present, there is a lack of literature describing the best salvage techniques for post-operative ACJ instability following failed suspension fixation devices used in the initial surgery. Here, we present a case report of a patient with failed ACJ/CC reconstruction using a FiberWire loop and Endobuttons and later revised with a duo figure-of-8 FiberTape (Arthrex, Naples, FL, USA) augmented autogenic graft wrapping technique.
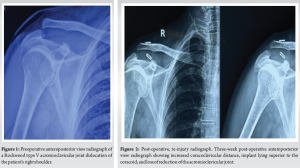
This is a 50-year-old healthy male who presented to our outpatient department (OPD) with chief complains of pain in the right shoulder region and recurrence of a deformity which was treated 3 weeks ago somewhere in another hospital. After taking a detailed history and going through the medical records available with him, it was found that he had Type-V ACJ injury post-fall from a bike in a road traffic accident (Fig. 1) for which he underwent surgical stabilization of the ACJ 3 days after the injury using a continuous FiberWire loop and double Endobutton construct. After 17–18 days of the surgery, the patient was lifting a heavy shutter with his left hand (normal) by bending forward. It was at this very moment he heard a popping sound and pain started in the right shoulder region. He visited our OPD and he was advised of plain radiographs of the right shoulder which reflected failed post-surgery ACJ dislocation (Fig. 2). The Endobutton passed through the coracoid base was lying superior to the base of the coracoid, which should be lying inferior to it indicating that the Endobutton had blown out of the coracoid drill hole. Non-contrast computed tomography was done to confirm the drill hole position in the coracoid base. A drill hole was not well visualized indicating the primary surgeon might have made an anterior, much superficial drill hole in the tip of the coracoid (Fig. 3).
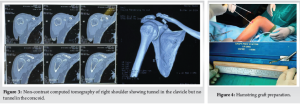
Non-operative versus operative management options were discussed with the patient, and ultimately, he was planned to undergo revision ACJ reconstruction using double figure-of-8 autogenic loop reconstruction (hamstring tendon graft) of ACJ and augmentation with FiberTape.
Revision surgery
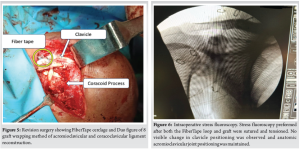
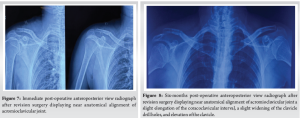
Three weeks after the initial operation, the patient was again taken to the operating room for revision ACJ and CC reconstruction. Intraoperative findings showed a maintained position of suspension buttons over the clavicle but loosening of the construct and coracoid Endobutton was lying superior and lateral to the process due to coracoid blow-out. The hole was drilled in the clavicle for passing the Endobutton at 20 mm from the lateral end of the clavicle and only one limb was used (lateral or trapezoid). The drill hole through the base of the coracoid process appeared blown out. The entire FiberWire and loop system was removed, and revision fixation was performed. Two drill holes of 4 mm diameter in the clavicle, medial at 35 mm and lateral at 20 mm from the distal end of the clavicle were made. A 4 mm semitendinosus hamstring autograft was harvested for reconstruction of acromioclavicular (AC) and CC ligament and passed along with FiberTape through the clavicle tunnel and looped around the coracoid in a figure-of-8 manner to complete the vertical figure-of-8 graft wrapping and FiberTape was tensioned manually and 3 knots were applied over the superior surface of the clavicle and the graft was sutured over the superior surface of the clavicle for the fixation (Fig. 5). The long tail of the remaining graft length was adjusted by passing it laterally and looped in a figure-of-8 manner around the acromion process and over the superior surface of the clavicle and reconstructed superior and inferior slings of AC ligament and to complete the horizontal figure-of-8 graft wrapping. The FiberTape was used to augment the fixation of a reconstructed ligament. Radiographs were obtained intraoperatively to check the adequacy of the loop and to verify the reduced position of the distal clavicle against the acromion (Fig. 6). After the final suturing of the graft, the stress test was performed with the weight of the arm and traction pulled showing no change in position or reduction (Fig. 7).
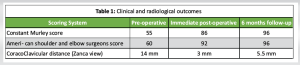
Constant Murley score, American Shoulder and Elbow Surgeons (ASES) score were calculated pre and post-operatively for clinical scoring and Coracoclavicular distance (Zanca view) was calculated.
Follow-up
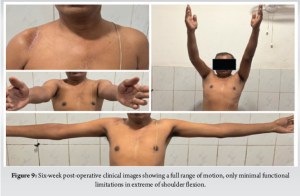
At the 6-week follow-up after revision fixation, radiographs of the right shoulder showed near-anatomic alignment of the ACJ and CC. The patient experienced minimal pain and was able to perform gentle movements in flexion, extension, abduction, and both internal and external rotation. By the 6-month follow-up, additional radiographs (Fig. 8) revealed a slight elongation of the CC interval, a slight widening of the clavicle drill holes, and elevation of the clavicle, though the patient was asymptomatic. Clinical and radiological outcomes were calculated and compared. Constant Murley score and ASES showed significant improvement in immediate post-operatively and in follow-up (Table 1). The patient reported almost full range of motion, excellent strength, and only minimal functional limitations in extreme of shoulder flexion (Fig. 9).
Injuries to the ACJ account for approximately 10% of all shoulder injuries. Despite being a common type of shoulder injury, there is still no consensus on the optimal surgical technique for treating these injuries. Clinical and anatomical studies are ongoing to develop more anatomically accurate reconstruction methods. The original Weaver-Dunn technique [6], introduced in 1972, involves excision of the distal clavicle, detachment of the coracoacromial ligament from its acromial attachment, and its transfer to the distal clavicle. However, recent biomechanical studies have shown that anatomical reconstruction using free grafts offers greater stability compared to other ligament transfer techniques. Maintaining the clavicle in a reduced position is typically sufficient for primary reconstruction, using methods such as tension bands and K-wires through the ACJ or extra-articular Bosworth screws. These straightforward techniques depend on the natural healing of the CC ligaments [7]. However, these are non-dynamic fixation methods, which can lead to implant failure [8]. It has been reported that CA ligament transfer, hook-plate fixation, AC K-wire fixation, and CC screw fixation may be biomechanically insufficient [9]. In addition, multiple drill holes in the clavicle can create stress risers, increasing the risk of implant cut-out [10]. Other complications include acromial osteolysis, fractures, ACJ osteoarthritis, subacromial impingement, and rotator cuff tears. The necessity for a second surgery to remove implants is another drawback, which can result in late fractures of the distal clavicle after low-energy trauma [11]. A more recent technique, the TightRope (Arthrex, Naples, FL, USA) or Loop Endobutton, is currently one of the most widely used methods. This system consists of a double metallic button with FiberWire strands. While it offers a shorter rehabilitation period and quicker return to daily activities, some controversy remains. Compared to other methods, some patients may require longer rehabilitation. In addition, this technique is not as cost-effective as open procedures, despite being a single surgery. Osteolysis around the tunnels and Endobuttons is another potential complication during the follow-up period. In this case, the loop Endobutton/TightRope device was selected as the fixation method based on the surgeon’s discretion, as it has demonstrated satisfactory stability and high tensile strength in cadaveric studies and has been effective in treating patients with AC dislocations [3, 12, 13]. The surgical technique is straightforward, does not require a graft, has not been associated with major complications, and does not necessitate material removal. However, a potential drawback of this device is the risk of coracoid fracture or tunnel blowout, as the device’s failure load may exceed the coracoid bone’s failure threshold. In cases of surgical failure or complications, opting for non-operative management may be a reasonable choice for patients with low activity levels. Therefore, indications for ACJ reoperation can vary depending on the patient population [5]. Recurrent ACJ instability after failure presents significant surgical challenges, as there is no “gold standard” technique for revision stabilization. ACJ revision procedures require careful preoperative planning and identification of the cause of reinjury to ensure proper surgical strategy and patient education. Adherence to post-operative protocols is crucial, as non-compliance can significantly impact surgical outcomes [14]. The double loop figure-of-8 graft wrapping technique, combined with a FiberTape tensioning system, offers several advantages. It allows the surgeon to precisely control the reduction, facilitating accurate anatomic repair or reconstruction of the AC and CC ligaments [15]. When performed correctly, this technique provides stable anatomic fixation, with a low risk of device migration and improve clinical outcomes [16].
The case presented here is one of the few reported examples of a failure of the loop Endobutton device for ACJ reconstruction. This case highlights the challenges of managing failed ACJ reconstruction. This patient, initially treated with the FiberWire loop Endobutton method resulted in post-operative failure due to coracoid blowout and improper drill hole positioning. Revision surgery using the duo figure-of-8 FiberTape augmented autogenic hamstring graft wrapping technique provides effective reconstruction of both the ACJ and CC, restoring stability and functionality. This case underscores the importance of precise revision surgical technique and suggests that a combination of FiberTape and autograft can offer a viable salvage option for recurrent ACJ instability for improving patient outcomes.
The double figure-of-8 autogenic loop reconstruction with FiberTape and hamstring tendon graft offers a reliable solution for managing revision ACJ reconstruction, providing enhanced stability and excellent functional outcomes.
References
- 1.Mazzocca AD, Arciero RA, Bicos J. Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med 2007;35:316-29. [Google Scholar]
- 2.Ruiz Ibán MA, Sarasquete J, Gil De Rozas M, Costa P, Tovío JD, Carpinteiro E, et al. Low prevalence of relevant associated articular lesions in patients with acute III-VI acromioclavicular joint injuries. Knee Surg Sports Traumatol Arthrosc 2019;27:3741-6. [Google Scholar]
- 3.Cano-Martinez JA, Nicolas-Serrano G, Bento-Gerard J, Picazo-Marin F, Andres-Grau J. Acute high-grade acromioclavicular dislocations treated with triple button device (MINAR): Preliminary results. Injury 2016;47:2512-9. [Google Scholar]
- 4.Clavert P, Meyer A, Boyer P, Gastaud O, Barth J, Duparc F, et al. Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation. Prospective multicenter study of 116 cases. Orthop Traumatol Surg Res 2015;101:S313-6. [Google Scholar]
- 5.Gowd AK, Liu JN, Cabarcas BC, Cvetanovich GL, Garcia GH, Manderle BJ, et al. Current concepts in the operative management of acromioclavicular dislocations: A systematic review and meta-analysis of operative techniques. Am J Sports Med 2019;47:2745-58. [Google Scholar]
- 6.Weaver JK, Dunn HK. Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am 1972;54:1187-94. [Google Scholar]
- 7.Kienast B, Thietje R, Queitsch C, Gille J, Schulz AP, Meiners J. Mid-term results after operative treatment of grade III-V acromioclavicular joint dislocations with an AC-hook-plate. Eur J Med Res 2011;16:52-6. [Google Scholar]
- 8.Graupe F, Dauer U, Eyssel M. Late results of surgical treatment of tossy III acromioclavicular joint separation with the balser plate. Unfallchirurg 1995;98:422-6. [Google Scholar]
- 9.Jari R, Costic RS, Rodosky MW, Debski RE. Biomechanical function of surgical procedures for acromioclavicular joint dislocations. Arthroscopy 2004;20:237-45. [Google Scholar]
- 10.Frank RM, Trenhaile SW. Arthroscopic-assisted acromioclavicular joint reconstruction using the tightrope device with allograft augmentation: Surgical technique. Arthrosc Tech 2015;4:e293-7. [Google Scholar]
- 11.Nadarajah R, Mahaluxmivala J, Amin A, Goodier DW. Clavicular hook-plate: Complications of retaining the implant. Injury 2005;36:681-3. [Google Scholar]
- 12.Cano-Martinez JA, Nicolas-Serrano G, Bento-Gerard J, Marin FP, Grau JA, Anton ML. Chronic acromioclavicular dislocations: Multidirectional stabilization without grafting. JSES Int 2020;4:519-31. [Google Scholar]
- 13.Ladermann A, Gueorguiev B, Stimec B, Fasel J, Rothstock S, Hoffmeyer P. Acromioclavicular joint reconstruction: A comparative biomechanical study of three techniques. J Shoulder Elbow Surg 2013;22:171-8. [Google Scholar]
- 14.Guy DK, Wirth MA, Griffin JL, Rockwood CA Jr. Reconstruction of chronic and complete dislocations of the acromioclavicular joint. Clin Orthop Relat Res 1998;347:138-49. [Google Scholar]
- 15.Youn GM, Chakrabarti MO, McGahan PJ, Chen JL. Acromioclavicular joint repair using a suture cerclage tensioning system. Arthrosc Tech 2019;8:e1555-60. [Google Scholar]
- 16.Sobhy MH. Midterm results of combined acromioclavicular and coracoclavicular reconstruction using nylon tape. Arthroscopy 2012;28:1050-7. [Google Scholar]







