
1. Given that this is one of the rarer presentations associated with brucellosis, it is crucial to place greater emphasis on this aspect, particularly in regions with a significant population of camel herders. 2. It is important to educate patients about the potential consequences of ingesting raw milk, especially for those at higher risk, such as the elderly and immunocompromised individuals. Although rare, this infection can manifest in various parts of the body, and its impact has been documented
Dr. Shahad Khaldi, Department of Emergency Medicine, King Abdulaziz Medical City, Ministry of the National Guard- Health Affairs, Jeddah - 21423, Saudi Arabia. E-mail: shahd1khaldi@gmail.com
Introduction: Bakers (popliteal) cysts are cystic masses that arise from bursae swellings filled with synovial fluid. It is assumed that preceding osteoarthritic or meniscal injuries cause the synovial fluid to extrude and concentrate, forming a gel-like material within a cyst. Clinical presentation is either symptomatic or asymptomatic swelling. The following symptoms are commonly associated with this condition: Knee pain, stiffness, and limited knee range of motion. Based on symptomatology and etiology, the management plan can be divided into conservative versus surgical intervention, by either decompression or excision. In most cases, baker cysts are not associated with infections. However, in our case report, we found that the patient had a positive Brucella culture in a symptomatic baker cyst.
Case Report: This is an 84-year-old gentleman, who is known to have diabetes, hypertension, dyslipidemia, and heart disease presented to the emergency medicine department with complains of knee pain and swelling. The patient mentioned a recent ingestion of unpasteurized milk and a positive history of brucellosis infection years ago. The knee aspiration of the cyst resulted in a positive Brucella culture. The treatment involves eradicating the infection with intravenous antibiotics and then decompressing or excising the cyst, depending on the patient’s clinical symptoms. Regarding our management approach, the patient underwent a conservative management with intravenous antibiotics.
Conclusion: In comparison to other more common organisms, such as Staphylococcus aureus species, Brucella is rarely found in baker’s cysts. However, as demonstrated in our case report, it is important to keep infections, as rare as brucellosis, in the differential diagnosis of baker’s cysts to provide the most appropriate management for patients.
Keywords: Popliteal, baker’s cyst, brucellosis, knee aspiration.
Baker synovial cyst also known as a popliteal cyst is defined as a synovial cyst that occurs due to intra-articular knee disorders, for example, osteoarthritis and meniscus tears [1]. It manifests mainly as a posterior knee mass, pain, and limited knee range of motion (ROM). Baker cysts have two different treatment plans, either to proceed with conservative or surgical management [2]. Asymptomatic small cysts can be managed conservatively, as opposed to large or symptomatic cysts which can be treated by either surgical aspiration or excision [2]. Baker cysts are usually a non-infectious joint effusion that seldom gets infected as a complication, however, the most common organism cultured is Gram-positive cocci, Staphylococcus aureus [3]. Previous studies reported a relationship between popliteal cysts and arthritis that were caused by infections such as Candida, Aspergillus species, and tuberculosis [4-6]. Nevertheless, it is very unusual to have a baker’s cyst as a presentation of brucellosis. Brucellosis is a zoonotic infection transmitted by contact with infected animals and their products such as raw unpasteurized milk [7]. It affects a wide range of angles, such as patients’ well-being, lifestyle, and economic status [8,9]. The severity of brucellosis in KSA is so extreme that it can be used as a gauge of the disease’s widespread prevalence as shown by a study done by Al Shammari et al. [10] Brucellosis frequently manifests as an intra-articular infection through hematogenous spread; the sacroiliac and knee joints are the most involved [11]. Therefore, in this case, we report the rare presentation of cultured Brucella in Baker’s cyst aspiration.
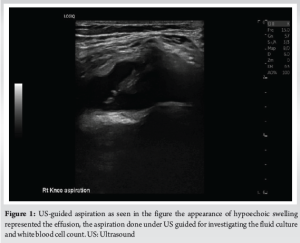
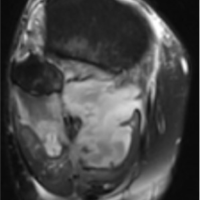
This is an 84-year-old gentleman, who is a known case of diabetes, hypertension, dyslipidemia, non-alcoholic steatohepatitis, irritable bowel syndrome, transient ischemic attack, lung cancer primarily with bone metastasis, and bilateral knee osteoarthritis. He had a positive history of brucellosis 5 years ago which was treated. On August 22, 2023, the patient was brought by his son asking for knee aspiration because his father was complaining of right knee pain and increased back pain. Thus, ultrasound-guided aspiration was performed for his right knee and reported and 80 cc was cultured (Fig. 1). On August 30, 2023, the patient was called and asked to come immediately for admission as the aspirated fluid showed positive results for Brucella species. In addition, the culture was sent for a susceptibility test and found to be sensitive to trimethoprim, ciprofloxacin, tetracycline, and gentamicin. Afterward, the patient was admitted after he was seen in the emergency department, denying a history of trauma, worsening of pain or swelling, or any other complaints.
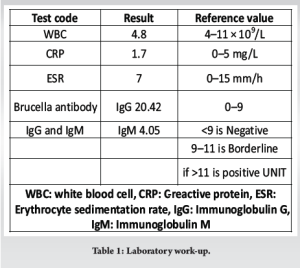
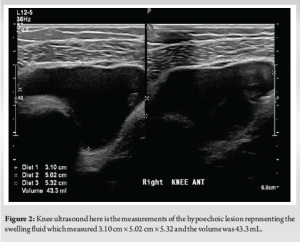
On physical examination, the patient was alert, conscious, and oriented; and was vitally stable and afebrile. Posterior mass was appreciated in his right knee with a size of 5 × 10 cm, soft in consistency, fluctuating, and non-tender, no inflammatory signs were apparent such as erythema, hotness, or discharges. In addition, cautery signs on his bilateral knees were found with full ROM and intact distal neurovascular examination. His work-up results showed low white blood cell count levels while the erythrocyte sedimentation rate (ESR) level was high as shown in Table 1. On right knee ultrasound, findings showed moderate to large joint effusion with no definite synovial thickening (Fig. 2).
The patient was given an antibiotic course of 100 mg gentamicin Q24 IV, 400 mg ciprofloxacin Q12 IV, and 100 mg doxycycline Q12 PO. On daily round follow-up, the patient was seen complaining of mild redness without itchiness that started on the 2nd day of admission involving forearms and lower limbs bilaterally and ciprofloxacin was stopped by the infectious disease (ID) team while continuing on doxycycline and gentamycin. Later, the patient was doing well with no active issues, continued antibiotics for 7 days IV/PO, and was discharged home on September 06, 2023, doing well with doxycycline 100 mg Q12 PO for 90 days and his regular medication refill and a follow-up appointment with orthopedics and ID in 1 week and 2 weeks, respectively.
As mentioned previously, the focal presentation of brucellosis involves joint manifestation, in which the commonly reported part was the knee [7]. Nevertheless, insufficient reported cases were found. One case was reported in 1996, where a medically free 60-year-old male presented with a 5-month history of fever, night sweats, and popliteal swelling and tenderness after drinking raw milk. Patients reported to have elevated (ESR) in contrast to our case in which it was a normal level. The computed tomography and US showed the presence of a popliteal cyst. After aspiration of the cyst and culturing, the synovial fluid showed to have Brucella abortus [12]. Thus, the patient was managed by streptomycin and doxycycline and then discharged. Later follow-up showed the disappearance of his effusion and Baker’s cyst. However, after 10 days, the patient was readmitted due to a flare-up of his manifestation. Open drainage and resection of his Baker’s cyst were needed and then antibiotics were maintained. Later after 4 months, the patient was asymptomatic and imaging results of his right knee were normal [12]. In another more recent case reported in 2015, a 55-year-old diabetic male presented with a history of fever and left knee pain for 7 days along with tenderness in the left popliteal fossa, redness, and swelling [11]. Furthermore, the patient had elevated ESR levels while other laboratory findings were normal. Fluid aspiration and analysis of the cyst were performed and revealed the presence of Brucella species [11]. Management was started by giving ciprofloxacin, gentamicin, and doxycycline. The patient was discharged after 7 days of admission and then on a follow-up appointment he was afebrile, and his swelling had resolved. Nonetheless, both previous examples showed infectious signs and symptoms in the form of fever, night sweats, redness, and tenderness, respectively, before being diagnosed with brucellosis, as opposed to our case in which the patient’s only symptoms at the time of aspiration were pain, swelling, and he was completely asymptomatic and electively admitted at the time of the diagnosis.
Although brucellosis is rare to be found in baker cyst fluid aspiration, it is highly crucial to keep in mind that it could be one of the differential diagnoses. Therefore, physicians are recommended to be aware of this possibility, especially since brucellosis has been increasing in developing countries such as Saudi Arabia.
Healthcare practitioners should maintain a high index of suspicion when treating camel herders, as this population may have an elevated risk of infection manifesting in various body parts. A thorough management plan is essential for these rare cases, encompassing appropriate antibiotic therapy, clear indications for surgical intervention, and scheduled follow-up appointments. Although these infections are uncommon, they have been well-documented and require careful consideration in clinical practice.
References
- 1.Frush TJ, Noyes FR. Baker’s cyst: Diagnostic and surgical considerations. Sports Health 2014;7:359-65. [Google Scholar | PubMed]
- 2.Leib AD, Roshan A, Foris LA, Varacallo M. Baker’s Cyst. Treasure Island, FL: StatPearls Publishing; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/nbk430774. Last accessed [September 30, 2023]. [Google Scholar | PubMed]
- 3.Drees C, Lewis T, Mossad S. Baker’s cyst infection: Case report and review. Clin Infect Dis 1999;29:276-8. [Google Scholar | PubMed]
- 4.Cuende E, Barbadillo C, E-Mazzuchelli R, Isasi C, Trujillo A, Andreu JL. Candida arthritis in adult patients who are not intravenous drug addicts: Report of three cases and review of the literature. Semin Arthritis Rheum 1993;22:224-41. [Google Scholar | PubMed]
- 5.Austin KS, Testa NN, Luntz RK, Greene JB, Smiles S. Aspergillus infection of total knee arthroplasty presenting as a popliteal cyst. Case report and review of the literature. J Arthroplasty 1992;7:311-4. [Google Scholar | PubMed]
- 6.Ellis ME, El-Ramahi KM, Al-Dalaan AN. Tuberculosis of peripheral joints: A dilemma in diagnosis. Tuber Lung Dis 1993;74:399-404. [Google Scholar | PubMed]
- 7.Madkour M. Madkour’s Brucellosis. Berlin: Springer; 2001. Available from: https://books.google.com.sa/books?id=Kanraaaamaaj [September 30, 2023]. [Google Scholar | PubMed]
- 8.Corbel M. Brucellosis in Humans and Animals. FAO, OIE, WHO; 2006. Available from: https://www.who.int/csr/resources/publications/brucellosis.pdf [September 30, 2023]. [Google Scholar | PubMed]
- 9.World Health Organization. The Control of Neglected Diseases: A Route to Poverty Alleviation; 2006. Available from: https://www.who.int/zoonoses/Report_Sept06.pdf [September 30, 2023]. [Google Scholar | PubMed]
- 10.Al-Shammari SH, Al-Shehri SA, Alshehri SS. Epidemiology of Brucella infection in the human, livestock and wildlife interface in Saudi Arabia. 2022;11:53. [Google Scholar | PubMed]
- 11.Shaya OA, Amin MR, Benmeakel M. Unusual presentation of brucellosis in Baker’s cyst. J Med Cases 2015;6:450-2. [Google Scholar | PubMed]
- 12.Blanco R, Gonzalez-Gay MA, Varela J, Monte R, Sanchez-Andrade A, Gonzalez-Vela C. Baker’s cyst as a clinical presentation of brucellosis. Clin Infect Dis 1996;22:872-3. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2023 Infection of Baker’s Cyst without Bacteremia, Sepsis, or Extraneous Source: A Case Report
January 10, 2023 Infection of Baker’s Cyst without Bacteremia, Sepsis, or Extraneous Source: A Case Report September 10, 2022 An Uncommon Case of Brucellar Spondylodiscitis: A Case Report
September 10, 2022 An Uncommon Case of Brucellar Spondylodiscitis: A Case Report May 10, 2021 Ruptured Popliteal Cysts Mimicking Deep Vein Thrombosis in Well-Functioning Total Knee Replacements: Report of Two Cases and Review of Literature
May 10, 2021 Ruptured Popliteal Cysts Mimicking Deep Vein Thrombosis in Well-Functioning Total Knee Replacements: Report of Two Cases and Review of Literature November 10, 2018 Infected Baker’s Cyst: A New Classification, Diagnosis and Treatment Recommendations
November 10, 2018 Infected Baker’s Cyst: A New Classification, Diagnosis and Treatment Recommendations