
Obturator-type hip dislocation is a rare clinical entity and an orthopedic emergency, as it requires urgent atraumatic reduction ideally under anesthesia and fixation of the trochanteric fracture to preserve vascularity of the femoral head. This article demonstrates unique management approach to such a case.
Dr. Pankaj Kumar Sharma, Department of Orthopaedics, All India Institute of Medical, Sciences, Bathinda, Punjab, India. E-mail: dr.pankajkristwal@gmail.com
Introduction: Anterior hip dislocations are less common in orthopedic casualties than posterior and are associated with concurrent injuries such as acetabulum fracture, femoral head fracture, or unstable pelvic injuries. Rarer still, is the obturator dislocation of the hip, with only a handful cases described in the literature with no established treatment protocols.
Case Report: We treated a young male injured in a car accident and sustained an anterior hip dislocation (obturator type) with a concomitant fracture of the ipsilateral greater trochanter. This type of injury is rare and there is no consensus in medical literature regarding the mechanism and treatment of such an entity. The initial close relocation of the hip under anaesthesia and open reduction and internal fixation with cancellous screws produced outstanding results over a follow-up period of 3 years. The abductor mechanism was intact and in continuity with the shattered greater trochanter as well as the vastus lateralis muscle intra-operatively.
Conclusion: At the 3-year follow-up, the patient had an outstanding functional hip joint with no chronic morbidity, such as avascular necrosis or arthritic alterations. A review of the literature was done evaluate the proposed mechanism and management of such a rare injury.
Keywords: Hip dislocation, obturator, greater trochanter, flip separation, abductor mechanism, avascular necrosis, arthritis, hip, prevention.
Traumatic hip dislocation is becoming more common as a result of increased road traffic accidents and accompanying high-energy trauma. Most dislocations are posterior, with anterior dislocations accounting for <10–15% of all incidents [1-3]. Superior anterior dislocations occur when the femoral head is moved into the iliac or pubic region, while inferior dislocations occur when it is displaced into the obturator region. Many studies have found a link between hip dislocation and acetabular fractures or fractures of the head, neck, or shaft of the femur [1-5]. However, the combination of anterior hip dislocation with ipsilateral greater trochanter fracture is highly unusual with only a few cases reported earlier and most often they are associated with other injuries or are open injuries [6-11]. We documented the mechanism and treatment of such rare presentation of anterior-inferior dislocation of the hip (obturator type) and consummated ipsilateral greater trochanter fracture with intact abductor mechanism and lateral soft-tissue sleeve, a new variation of the obturator-type dislocation.
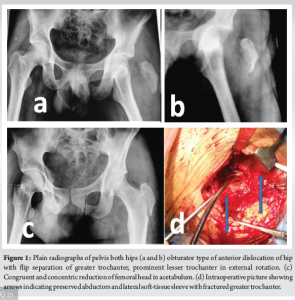
A 30-year-old male biker was involved in a road traffic accident after colliding head-on with an automobile. He was taken to the emergency room within an hour of the incident, suffering from significant hip pain and limb deformity. He was extensively evaluated, and his vitals were stabilized in accordance with established advanced trauma life support protocols. The left lower limb was found to be in external rotation, abduction, and flexion at the hip joint during the assessment. There were superficial abrasions on the left breast, ipsilateral knee, and hip, but the distal neurovascular condition was normal. There was painful swelling in the left inguinal and hip region, which was considered to be a palpable femoral head due to synchronous movement with the left lower limb. The limb movements were excruciatingly uncomfortable. Plain radiographs taken of bilateral hip with pelvis which revealed an anterior kind of hip dislocation of the left femoral head, along with an ipsilateral fracture of the greater trochanter. Within 4 h post-trauma, dislocation was reduced under sedation and skeletal traction was applied through Steinmann pin passed through the upper tibia. Closed relocation of the hip was done with standard maneuver, while keeping the limb in extension and axial traction was maintained, the femoral head was reduced manually in the acetabulum, thereafter limb was positioned in flexion, internal rotation and adduction for stabilization. As the patient was not fit to be taken for surgery due to chest condition, the fractured greater trochanter was not fixed at the same time. Status of reduction was assessed by post-manipulation radiographs, which revealed a reduced femoral head with fracture of the greater trochanter and no intra-articular extension. Dislocation of the femoral head with ipsilateral fracture greater trochanter and relocation of the head in acetabulum with reduced fractured trochanter and intact abductors, after manipulation, are shown in Fig. 1. Elective surgery was planned after 4 days of injury under spinal anaesthesia with patient positioned supine in operation theatre under all aseptic precautions.
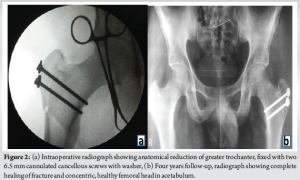
 Intraoperatively, it was observed that the abductor muscles were attached to the separated greater trochanter and in continuity with vastus lateralis sleeve, thus preserving the abductor mechanism. The fracture was reduced under the image intensifier and fixed with two cancellous lag screws with washer. Post-operative period was uneventful, and the patient was discharged after 2 days with complete recovery. Fixation of fractured trochanter in place intra-operatively and 3 years follow-up are illustrated in Fig. 2. Patient was immobilized postoperatively by skeletal traction for 2 weeks as ample precaution due to concerns that he may dislocate again, especially due to the fact that for rural patients who may struggle with adherence to immobility instructions due to various factors, skeletal traction serves as an effective means of ensuring stability, managing pain, facilitating healing, and preventing complications during their recovery process. After that, partial weight bearing was allowed, while full weight bearing was started after 1 month postoperatively. At 1 month of follow-up, Trendelenburg sign was positive on the left hip; but at 3 months, there were no more abductor lurch and pain-free movements at the hip joint (130° flexion, 35° internal rotation, 40° external rotation, and adduction – abduction of 45° each). At the 3 years of final follow-up, neither myositis ossificans nor avascular necrosis of femoral head was observed with full and functional pain-free hip movements. The Harris Hip Score was 96 at 3-year assessment with good patient satisfaction and acceptance.
Intraoperatively, it was observed that the abductor muscles were attached to the separated greater trochanter and in continuity with vastus lateralis sleeve, thus preserving the abductor mechanism. The fracture was reduced under the image intensifier and fixed with two cancellous lag screws with washer. Post-operative period was uneventful, and the patient was discharged after 2 days with complete recovery. Fixation of fractured trochanter in place intra-operatively and 3 years follow-up are illustrated in Fig. 2. Patient was immobilized postoperatively by skeletal traction for 2 weeks as ample precaution due to concerns that he may dislocate again, especially due to the fact that for rural patients who may struggle with adherence to immobility instructions due to various factors, skeletal traction serves as an effective means of ensuring stability, managing pain, facilitating healing, and preventing complications during their recovery process. After that, partial weight bearing was allowed, while full weight bearing was started after 1 month postoperatively. At 1 month of follow-up, Trendelenburg sign was positive on the left hip; but at 3 months, there were no more abductor lurch and pain-free movements at the hip joint (130° flexion, 35° internal rotation, 40° external rotation, and adduction – abduction of 45° each). At the 3 years of final follow-up, neither myositis ossificans nor avascular necrosis of femoral head was observed with full and functional pain-free hip movements. The Harris Hip Score was 96 at 3-year assessment with good patient satisfaction and acceptance.
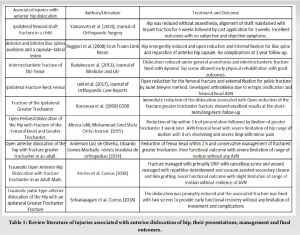
Due to its spheroidal shape and strong congruence between the femoral head and acetabulum supported by the capsule, related ligaments, and surrounding soft tissues, the hip joint is exceptionally stable [1,2]. Hip dislocation necessitates a significant amount of directed force. The third decade of life accounts for 35% of all traumatic hip dislocations, with a male-to-female ratio of 3:1 [1-5]. The ratio of posterior hip dislocation to anterior hip dislocation ranges from 1:10 to 1:19 [1-3]. Mechanism of injury in the case of anterior hip dislocation is posterior directed force which drives the hip in abduction and external rotation or fall from a considerable height or blow from back while in squatting position [2,4-6]. These are classified according to the Epstein classification and may be anteroinferior (obturator type, hip in flexion) or anterosuperior (pubic type, hip in extension) depending on the attitude of the hip at the time of impact [1]. The hip remained abducted and externally rotated, with palpable swelling inferiorly in obturator type while femoral head presented as groin swelling superiorly in pubic type dislocation. Plain radiographs are the first and most used investigation to diagnose the type of dislocation, wherein abnormal position of femoral head outside the acetabulum and lesser trochanter becoming more prominent than normal one with external rotated attitude of limb. Anterior hip dislocations are often open and can be associated with other injuries including femoral head fracture, acetabular fractures or associated neurovascular injuries around hip [4-13]. Some of the concomitant injuries with their review reported in the literature are listed in Table 1. Anterior dislocation of hip with closed ipsilateral fracture trochanter was managed with closed reduction and POP Spica cast in a case reported in past, but the patient remained non-ambulatory for 2 months with cast and functional outcome was not good over a year follow-up [6]. Close reduction of anterior dislocation and conservative management of ipsilateral fracture trochanter and associated vessel injury (external iliac artery) was done in an adult male with high energy trauma, reported poor functional outcome with decreased range of movements of hip [7]. Similarly, Atchi et al. managed a case having open fracture of the greater trochanter and iliac wing with anterior dislocation of ipsilateral hip with joint relocation, wound debridement and conservative means, resulting poor outcomes with associated avascular necrosis of head and secondary osteoarthritis of joint as sequelae at the 1-year follow-up period [11]. Freitas et al. reported an open case of anterior dislocation with fracture trochanter, which managed as primary fixation of fracture using two cancellous screws and adequate repetitive debridement of wound with vacuum-assisted secondary closure of the wound with skin grafting at the lateral aspect of the thigh over the 6 weeks [12]. Soft-tissue insult is highly appreciated with the high velocity and impact of these traumas, so we observed soft tissues of affected limb meticulously for 2 weeks in the present case. The medical literature revealed that most of the injuries were managed by conservative method and meticulous soft-tissue handling, resulting as variable poor to average outcome in form of decreased range of movements, avascular necrosis of head or osteoarthritis of hip joint. We followed the principle of early relocation of hip joint but open fixation of the fracture trochanter, which allowed the patient to early mobilization and gained excellent healing and functional outcome. According to recent research, the obturator dislocation is actually an inferior (rather than anterior) hip dislocation in which the acetabulum impinges on the superior rather than the posterior portion of the femoral head [14-16]. There is no universal mechanism accepted for such kind of dislocation with fracture ipsilateral trochanter. Fracture of the greater trochanter may be due to impaction injury with an iliac blade, while force of impact driven over the hip joint keeping it in external rotation, flexion/extension and abduction position [2-4]. The present case has peculiarity of its association with fracture of the ipsilateral greater trochanter along with maintained abductor mechanism and lateral soft-tissue sleeve. This can be explained by the fact that sudden force led to abrupt contraction of abductor muscles along with impaction by ilium leading to avulsion fracture of greater trochanter with minimum displacement. There may be different mechanism, if force directed in inverted femur with inferior placement of head in acetabulum, while knee is flexed and femur remains in abduction and external rotation [12]. However, flip separation of the greater trochanter is not explained by any mechanism. There were no other associated injuries. One-third of hips with anterior dislocation have a poor prognosis [1,16]. Hip dislocation is an orthopedic emergency that must be treated as soon as possible, preferably under general anaesthesia, to prevent and minimize sequelae [16,17]. Avascular necrosis of the femoral head, which can contribute to hip osteoarthritis later in life, heterotopic ossification surrounding the hip joint, and sciatic nerve damage are all possible complications after hip dislocation. Avascular necrosis is the most feared of all problems since a delay in the reduction of more than 6 h increases the risk of AVN from 10 to 40% and the incidence of AVN increased with depression of the femoral head detected on post-reduction roentgenograms [16-19]. We reduced the dislocation within 4 h of injury without insulting any soft tissue, so gained excellent functional outcome without any mentioned complications at 4 years follow-up. In this case, anatomic fixation of the greater trochanter minimized post-operative bed immobilization, provided adequate hip joint stability, and shortened the post-traumatic period of abductor lurch. Patients with vascular injuries also exhibit open dislocations or pubic or iliac dislocations [8-12]. These should be handled as quickly as possible with good wound care and head repositioning.
Management of these complex injuries requires a multidisciplinary approach to identify other associated injuries after stabilization of the patient. Early reduction of the dislocations is the key to minimize complications and rehabilitation of the patients in the long term.
Management of this unique and previously under-studied presentation of hip fracture/dislocations can result in excellent functional results for the patient if appropriately managed despite the high-velocity insult causing it.
References
- 1.Epstein HC, Harvey JP Jr. Traumatic anterior dislocations of the hip: Management and results. An analysis of fifty-five cases. J Bone Joint Surg Am 1972;54:1561-2. [Google Scholar | PubMed]
- 2.Duygulu F, Karaoglu S, Kabak S, Karahan OI. Bilateral obturator dislocation of the hip. Arch Orthop Trauma Surg 2003;123:36-8. [Google Scholar | PubMed]
- 3.Toms AD, Williams S, White SH. Obturator dislocation of the hip. J Bone Joint Surg Br 2001;83:113-5. [Google Scholar | PubMed]
- 4.Jain SK, Aggarwal P, Yadav A. Obturator dislocation of hip with ipsilateral fracture neck femur-a case report. J Orthop Case Rep 2017;7:16-9. [Google Scholar | PubMed]
- 5.Selvanayagam R, Tiwari V, Das S, Trikha V. Traumatic pubic-type anterior dislocation of the hip with an ipsilateral greater trochanter fracture: Case report and review of literature. Cureus 2018;10:e3287. [Google Scholar | PubMed]
- 6.Maruoka A, Naka N, Saito M, Toma Y. Pubic-type dislocation of the hip combined with fracture of the ipsilateral greater trochanter. A case report. Arch Orthop Trauma Surg 1993;112:299-301. [Google Scholar | PubMed]
- 7.Granahan A, McAuley N, Ellanti P, Hogan N. Traumatic anterior dislocation of the hip. BMJ Case Rep. 2016 Sep 2;2016:bcr2016216629. doi: 10.1136/bcr-2016-216629. [Google Scholar | PubMed | CrossRef]
- 8.Schwartz DL, Haller JA Jr. Open anterior hip dislocation with femoral vessel transection in a child. J Trauma 1974;14:1054-9. [Google Scholar | PubMed]
- 9.Jalili A, Zarei M. Open perineal dislocation of the hip with fracture of the femoral head and greater trochanter: A case report. Shafa Ortho J 2015;2:e1157. [Google Scholar | PubMed]
- 10.De Oliveira AL, Machado EG. Open anterior dislocation of the hip in an adult: A case report and review of literature. Rev Bras Ortop 2014;49:94-7. [Google Scholar | PubMed]
- 11.Atchi W, Anani A, Yannick D, Gamal A, Assang D. Open anterior dislocation of the hip in Togo. Clin Orthop Surg 2016;8:214-7. [Google Scholar | PubMed]
- 12.Freitas A, Giordano Neto V, Godinho PF, Macedo SL, Ribeiro De Oliveira VF, Montano GA, et al. Correction: Traumatic open anterior hip dislocation in an adult male: A case report. Cureus 2019;11:c16. [Google Scholar | PubMed]
- 13.Singh R, Sharma SC, Goel T. Traumatic inferior hip dislocation in an adult with ipsilateral trochanteric fracture. J Orthop Trauma 2006;20:220-2. [Google Scholar | PubMed]
- 14.Korovessis P, Droutsas P, Spastris P, Christodoulou G. Anterior dislocation of the hip associated with fracture of the ipsilateral greater trochanter. A case report. Clin Orthop Relat Res 1990;253:164-7. [Google Scholar | PubMed]
- 15.Singh AP, Singh AP, Mittal V. Traumatic inferior hip dislocation with ipsilateral open subtrochanteric fracture: A rare case. Injury Extra 2008;39:384-5. [Google Scholar | PubMed]
- 16.Bhagwat KR, Garg B, Aggarwal S, Dhillon MS. Bilateral inferior dislocation of the hip---a case report. Chin J Traumatol 2012;15:121-3. [Google Scholar | PubMed]
- 17.Radulescu R, Badila A, Japie I, Papuc A, Manolescu R. Anterior dislocation of the hip associated with intertrochanteric fracture of the femur - case presentation. J Med Life 2013;6:336-9. [Google Scholar | PubMed]
- 18.El Hajj Moussa M, Tawk C, Hoyek F, Lahoud JC. Traumatic inferior hip dislocation: A rare adult case with ipsilateral bifocal hip fracture. J Surg Case Rep 2016;2016:rjw056. [Google Scholar | PubMed]
- 19.Sahin V, Karakaş ES, Aksu S, Atlihan D, Turk CY, Halici M. Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-9. [Google Scholar | PubMed]
- 20.Bastian JD, Turina M, Siebenrock KA, Keel MJ. Long-term outcome after traumatic anterior dislocation of the hip. Arch Orthop Trauma Surg 2011;131:1273-8. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Salvaging Femur Head in a Pipkin Type III Femoral Head Fracture with Open Reduction and Internal Fixation Using Herbert Screw Fixation: A Rare Case Report
October 1, 2025 Salvaging Femur Head in a Pipkin Type III Femoral Head Fracture with Open Reduction and Internal Fixation Using Herbert Screw Fixation: A Rare Case Report June 10, 2023 Acute COVID-Related Hip Arthritis. Case Report and Literature Review
June 10, 2023 Acute COVID-Related Hip Arthritis. Case Report and Literature Review February 1, 2026 Case Report of Post-Traumatic Monoarticular Tuberculosis of the Knee in a Healthy Young Adult: Diagnostic and Therapeutic Challenges in a Non-Endemic Setting
February 1, 2026 Case Report of Post-Traumatic Monoarticular Tuberculosis of the Knee in a Healthy Young Adult: Diagnostic and Therapeutic Challenges in a Non-Endemic Setting February 1, 2026 A Rare Case: Septic Arthritis of The Wrist
February 1, 2026 A Rare Case: Septic Arthritis of The Wrist