
Aberrant morphology of the suprascapular neurovascular structures at the level of the suprascapular notch should be considered during posterior shoulder surgery or peripheral nerve blocks to minimize the risk of neurovascular complications.
Dr. Bryan G Beutel, Department of Pathology and Anatomical Sciences, Kansas City University College of Medicine, 1750 Independence Avenue, Kansas City - 64106, Missouri, United States. E-mail: bryanbeutel@gmail.com
Abstract
Introduction: The suprascapular neurovascular structures traverse the suprascapular notch in a variety of morphologies. However, the suprascapular nerve has always been described as coursing under the superior transverse scapular ligament (STSL) at the level of the notch. This report aims to describe a novel variant of suprascapular neurovascular structures found in a cadaver.
Case Report: During the dissection of a cadaveric upper extremity in an 85-year-old Caucasian male, the suprascapular nerve, artery, and vein were found to course above the STSL, with no structures passing through the foramen of the notch itself. A total of 94 upper extremities from 52 different cadavers were subsequently examined for the morphology of the suprascapular nerve, artery, and vein at the level of the suprascapular notch. No other cadavers were found to have this morphology, thereby resulting in an estimated prevalence of 1.1%.
Conclusion: This case study describes this unique unilateral shoulder anomaly, reviews the relevant literature, and discusses the potential clinical significance of this variant, which should be considered during various posterior shoulder surgeries or peripheral nerve blocks wherein aberrant morphology can increase the risk of neurovascular complications.
Keywords: Suprascapular nerve, suprascapular notch, morphology, variant.
The suprascapular foramen is a landmark location for the suprascapular nerve, suprascapular artery, and suprascapular vein. It is formed by the suprascapular notch and the superior transverse scapular ligament (STSL) bridging across it, transforming the notch into a foramen [1]. Classically, the suprascapular artery and suprascapular vein pass above (superior to) the STSL, whereas the suprascapular nerve passes under (inferior to) the STSL [1], but variations have been described and implicated in cases of refractory shoulder pain. The suprascapular artery commonly arises as a branch of the thyrocervical trunk of the subclavian artery, but studies have also reported anomalous branching directly from the subclavian artery distal to the scalene muscles [1]. The suprascapular artery descends laterally across the scalene muscles and phrenic nerve, whereas running posterior to the internal jugular vein and sternocleidomastoid. It then crosses anterior to the subclavian artery and brachial plexus, coursing parallel and posterior to the clavicle, subclavius, and inferior belly of the omohyoid muscle to reach the superior border of the scapula [1]. Often, it passes above the STSL to enter the supraspinous fossa and supply the supraspinatus muscle. It then descends posterior to the scapular neck and passes through the spinoglenoid notch, entering the infraspinous fossa where it supplies the infraspinatus muscle and anastomoses with the circumflex scapular artery and the deep branch of the transverse cervical artery [1]. The suprascapular nerve is a large branch of the upper trunk of the brachial plexus, traversing lateral and deep to the trapezius and omohyoid muscles. It classically enters the supraspinous fossa by passing under the STSL [1]. Subsequently, the nerve runs deep to provide motor innervation to the supraspinatus muscle. The suprascapular nerve then courses with the suprascapular artery through the spinoglenoid notch to enter the infraspinous fossa, where it produces two branches: One that provides motor innervation to the infraspinatus muscle and a sensory branch to the glenohumeral and acromioclavicular joints [1]. In the present case, a novel variation in the suprascapular neurovascular morphology at the suprascapular notch identified during cadaveric dissection is described, along with anatomic measurements of the suprascapular nerve, artery, and vein.
During the dissection of an 85-year-old Caucasian male cadaver, an anatomical variant was discovered at the suprascapular notch. The dissection procedure began with the careful removal of skin and overlying fascia at the level of the bilateral shoulders. The deltoid and trapezius muscles were then reflected to allow access to the scapula. The scapular fascia was then excised to access the supraspinous and infraspinous fossae. Both the supraspinatus and infraspinatus muscles were reflected laterally to provide access to the suprascapular notch and the associated neurovasculature. Blunt dissection was subsequently used to separate the neurovascular bundle and identify the suprascapular nerve, suprascapular artery, and suprascapular vein. Tracing the vessels and nerves from their respective origins to the infraspinatus muscle, the suprascapular artery, suprascapular vein, and suprascapular nerve were all observed running above the STSL in the right shoulder, a variant that has not been previously described in the literature (Fig. 1). This variant was not observed in the left upper extremity, where the suprascapular nerve was found coursing under the STSL with the vessels running above. During subsequent blunt dissection of the supraglenoid fossa, the suprascapular nerve was observed innervating the posterior shoulder capsule on the right.

Utilizing a Vernier caliper (Mitutoyo, Takatsu-Ku, Kawasaki, Japan), dimensional measurements were taken of the suprascapular notch, STSL, suprascapular nerve, suprascapular artery, and suprascapular vein on the right (Table 1). The artery, vein, and nerve were measured at the level of the suprascapular notch to maintain a consistent reference point.

To estimate the prevalence of the aforementioned variant morphology in the right shoulder, a total of 94 upper extremities from 52 different cadavers were examined for the morphology of the suprascapular nerve, artery, and vein at the suprascapular notch. No other cadavers exhibited this particular variant morphology, resulting in an estimated prevalence of 1.1% of shoulders.
As this was a study involving a single cadaver, no approval was required by the authors’ institutional biosafety committee.
The suprascapular notch is an area of notable anatomic variability, particularly when describing the course of the suprascapular artery and vein [2]. Classically, the suprascapular nerve has been described as coursing under the STSL [2-5]. However, the suprascapular artery and vein exhibit substantial variability, with some variants having the artery pass above the STSL and others demonstrating it passing under [6,7]. Polguj et al. previously formulated a classification system to describe the arrangement of the suprascapular vessels and nerves in relation to the STSL [2]. This classification includes four types in which the suprascapular nerve runs under the STSL in each variant. We propose a potential fifth variant (Type 5), in which the suprascapular artery, vein, and nerve all course above the STSL (Table 2). While the original Type 4 morphology was intended to include multiple other variants, neither Polguj nor other investigators have described the morphology seen in the present case study, thereby potentially warranting a distinct categorization (Fig. 2).


Suprascapular neuropathy commonly occurs at the suprascapular notch due to the variable size and morphology of the foramen through which the suprascapular nerve often passes [8]. This is particularly evident when there is ossification of the STSL. Suprascapular nerve release is performed at the suprascapular notch to address this condition by sectioning the STSL and decompressing the suprascapular foramen [8]. However, the presence of a Type 5 variant would preclude the typical compressive mechanism for this neuropathy. Nonetheless, with this variation, new mechanisms of neuropathy may emerge. Nearby musculature could impose compressive forces, which may warrant further clinical investigation to correlate these findings with patients presenting with suprascapular neuropathy.
Clinically, this novel variant may pose challenges for clinicians performing procedures in the suprascapular region. The suprascapular notch serves as a landmark for suprascapular nerve injections, whether for treating neuropathies or managing post-operative shoulder pain, particularly from a posterior approach [9]. This new variant could complicate the injection process due to the nerve coursing in an aberrant location. In addition, the nerve fibers found to be supplying the posterior shoulder capsule could contribute to persistent pain following such procedures. Furthermore, the lack of support for the suprascapular nerve from the suprascapular notch could complicate massive rotator cuff repairs. The repair of a supraspinatus tear during this procedure creates tension on the suprascapular nerve, possibly predisposing the patient to suprascapular neuropathy [10-13]. In cases with a Type 5 variation, the lack of support for the suprascapular nerve within the suprascapular notch may place additional tension on the nerve compared to those patients in whom the nerve travels through the notch.
The suprascapular nerve, artery, and vein were all observed coursing above the STSL in an 85-year-old Caucasian male cadaver. This is a variant that has not been previously described in the literature. The aberrant morphology described in this case may increase the risk of neurovascular injury during posterior shoulder surgeries or suprascapular nerve blocks. Surgeons should consider this variant during pre-operative planning and image-guided procedures to avoid iatrogenic complications.
The course of the suprascapular neurovascular structures exhibits notable variability at the level of the suprascapular notch. Among these variants, the suprascapular nerve, artery, and vein may pass above the STSL. This should be considered during posterior shoulder surgeries or peripheral nerve blocks wherein such aberrant morphology can increase the risk of neurovascular complications.
References
- 1.Standring S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. Philadelphia: Elsevier; 2021. p. 890-929. [Google Scholar | PubMed]
- 2.Polguj M, Rożniecki J, Sibiński M, Grzegorzewski A, Majos A, Topol M. The variable morphology of suprascapular nerve and vessels at suprascapular notch: A proposal for classification and its potential clinical implications. Knee Surg Sports Traumatol Arthrosc 2015;23:1542-8. [Google Scholar | PubMed]
- 3.Yang HJ, Gil YC, Jin JD, Ahn SV, Lee HY. Topographical anatomy of the suprascapular nerve and vessels at the suprascapular notch. Clin Anat 2012;25:359-65. [Google Scholar | PubMed]
- 4.Jezierski H, Wysiadecki G, Sibiński M, Borowski A, Podgórski M, Topol M, et al. A quantitative study of the arrangement of the suprascapular nerve and vessels in the suprascapular notch region: New findings based on parametric analysis. Folia Morphol (Warsz) 2016;75:454-9. [Google Scholar | PubMed]
- 5.Gürses İA, Gayretli Ö, Coşkun O, Kale A, Öztürk A. Anatomical relations between anterior coracoscapular ligament and suprascapular neurovascular structures and a proposal for classification. Acta Orthop Traumatol Turc 2015;49:433-7. [Google Scholar | PubMed]
- 6.Naidoo N, Lazarus L, De Gama BZ, Satyapal KS. The variant course of the suprascapular artery. Folia Morphol (Warsz) 2014;73:206-9. [Google Scholar | PubMed]
- 7.Tubbs RS, Smyth MD, Salter G, Oakes WJ. Anomalous traversement of the suprascapular artery through the suprascapular notch: A possible mechanism for undiagnosed shoulder pain? Med Sci Monit 2003;9:BR116-9. [Google Scholar | PubMed]
- 8.Arce G, Calvo A, Golano P. Suprascapular nerve release: Technique based on anatomic landmarks. Arthrosc Tech 2021;10:e469-73. [Google Scholar | PubMed]
- 9.Schoenherr JW, Flynn DN, Doyal A. Suprascapular nerve block. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar | PubMed]
- 10.Albritton MJ, Graham RD, Richards RS 2nd, Basamania CJ. An anatomic study of the effects on the suprascapular nerve due to retraction of the supraspinatus muscle after a rotator cuff tear. J Shoulder Elbow Surg 2003;12:497-500. [Google Scholar | PubMed]
- 11.Cummins CA, Messer TM, Nuber GW. Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-24. [Google Scholar | PubMed]
- 12.Prenaud C, Loubeyre J, Soubeyrand M. Decompression of the suprascapular nerve at the suprascapular notch under combined arthroscopic and ultrasound guidance. Sci Rep 2021;11:18906. [Google Scholar | PubMed]
- 13.Tsikouris G, Antonopoulos I, Vasdeki D, Chrysikos D, Koukakis A, Tsakotos G, et al. Morphometry and contents of the suprascapular notch with potential clinical implications: A cadaveric study. J Brachial Plex Peripher Nerve Inj 2021;16:e31-6. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Intraneural Ganglion of the Suprascapular Nerve with Asymmetric Branch Recovery and Dual-Site Compression: A Case Report
January 1, 2026 Intraneural Ganglion of the Suprascapular Nerve with Asymmetric Branch Recovery and Dual-Site Compression: A Case Report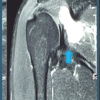 December 1, 2025 Arthroscopic Spinoglenoid Cyst Decompression and Labral Repair -Case Series
December 1, 2025 Arthroscopic Spinoglenoid Cyst Decompression and Labral Repair -Case Series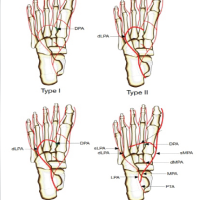 June 1, 2025 Medial Plantar Artery Dominance of the Plantar Arterial Arch: A Unique Anastomosis with Clinical Implications
June 1, 2025 Medial Plantar Artery Dominance of the Plantar Arterial Arch: A Unique Anastomosis with Clinical Implications February 10, 2024 When The Unexpected Happens: The Intriguing Retrieval of a Broken Epidural Catheter
February 10, 2024 When The Unexpected Happens: The Intriguing Retrieval of a Broken Epidural Catheter