
Understanding that vertebral hemangiomas, though typically asymptomatic, can present aggressively with neurological deficits, and recognizing the importance of early diagnosis, especially in atypical patient populations.
Dr. Daniela da Silveira Gravina, Department of Orthopedic and Trauma Surgery Department, Ecossistema de Saúde Pompeia, Caxias do Sul, RS, Brazil. E-mail: danigravina@gmail.com
Abstract
Introduction: Most vertebral hemangiomas are latent and don’t not require specific treatment; few cases present with symptoms, usually pain. Rarely, they manifest aggressively, causing neurological deficits from spinal cord compression.
Case Report: This case report describes a 13-year-old boy whose gait disturbance investigation revealed an aggressive T6 hemangioma.
Conclusion: Diagnosis is typically determined by imaging changes. Surgical treatment is indicated for cases with neurological deficits. Emergency decompression with laminectomy is required for rapid, progressive deficits, with radiotherapy considered based on extraosseous involvement. Level of Evidence IV. Case report.
Keywords: Hemangioma, spinal fractures, spinal cord compression.
Hemangioma is a benign lesion of the bones, composed of newly formed capillary, cavernous, or venous blood vessels. Some of these lesions are malformations, while others, due to their growth characteristics resembling neoplasms, are considered true benign tumors [1,2]. The term “aggressive hemangioma” refers to hemangiomas with extraosseous extension or significant bone expansion, accounting for approximately 1% of spinal hemangiomas [3]. Diagnosis is typically made through the detection of characteristic changes in imaging studies [4]. On plain radiography, hemangiomas are characterized by vertical trabeculae parallel to the vertebral bodies. Computed tomography (CT) reveals thick trabeculae and radiolucent areas, while magnetic resonance imaging (MRI) shows hyperintense signals on T1 and T2 sequences [5]. Surgical treatment is indicated for all cases with some degree of neurological deficit. Emergency decompression with laminectomy should be performed in all cases of rapid and progressive neurological deficit, with or without the need for adjuvant radiotherapy, depending on the extent of extraosseous involvement [5,6]. We describe a rare case of aggressive hemangioma in a patient that deviates from typical epidemiology.
Male, 13 years old, presenting with gait disturbance noted by the family without complaints of pain, evolving over 7 days. Evaluated by a neurologist, who referred him to an orthopedist. On physical examination, he presented with paraparesis in the lower limbs, classified as grade C according to the American Spinal Injury Association (ASIA) impairment scale (AIS). He denies a history of trauma or constitutional symptoms. On January 30, 2023, he underwent an MRI study (Fig. 1), revealing a lesion at the sixth thoracic vertebra (T6) with circumferential compression. Initially, a biopsy with histopathological examination was indicated (Fig. 2), revealing an aggressive hemangioma of T6.


Surgery for decompression with laminectomy without instrumentation was performed in the same internation, as there were no criteria for instability according to the Spine Instability Neoplastic Score, and the patient presented symptoms of spinal cord compression caused by the hemangioma in need of urgent therapy, without complaints of pain or changes in the height of the vertebral body. The patient was also placed in a SOMI brace and underwent physical therapy. A follow-up MRI (Fig. 3) 3 weeks later showed soft tissue and spinal cord edema. This was discussed in a multidisciplinary round, and 20 sessions of radiotherapy were recommended to prevent the progression of the extra-vertebral tumor.

Following radiotherapy sessions, a subsequent MRI (Fig. 4) 5 months after the laminectomy, revealed vertebral collapse and kyphosis (angle >20°), prompting the indication for thoracic vertebral fusion from the fourth to the eighth vertebra After a 3-month follow-up, the patient showed clinical improvement with no motor or sensory deficits, being classified as grade E according ASIA AIS. Radiological assessment (Fig. 5) demonstrated favorable outcomes, leading to the removal of the brace. The patient continued follow-up with physical therapy for muscle rehabilitation and improved mobility, with no pain complaints.

Vertebral hemangioma is typically asymptomatic and discovered incidentally, with reported incidences of 11% in autopsy series, but symptomatic cases are much rarer at 0.9–1.2%. When symptomatic, these hemangiomas commonly affect the thoracic spine, with a noted epidemiological preference for young women around the age of 40 [1,2]. The patient, in this case, being male and adolescent, deviates from this typical epidemiology found in the literature. Few cases evolve with symptoms, which often manifest as pain. However, in rare instances, hemangiomas can be aggressive, showing significant vertebral expansion, extraosseous components with epidural extension, blood flow disturbances, and occasionally compression fractures, leading to spinal cord and/or nerve root compression [3,7,8]. Diagnosis is typically made through characteristic imaging findings. On plain radiography, lesions in the spine may appear as vertical parallel striations formed by the dissociation of bone trabeculae without widening of the vertebral body, which is considered pathognomonic, as described by Deetz in 1901. CT can show sparse bony trabeculae alternating with hypertransparent areas on axial slices. MRI demonstrates hyperintense signals in the affected vertebral bodies due to fatty substitution [4,5]. Cases associated with back pain and without neurological deficits may be managed with periodic observation and clinical treatment, with refractory cases referred to exclusive radiotherapy or vertebroplasty [5,9]. Hemangiomas causing pain or spinal cord compression are associated with moderate-to-intense hypervascularization. If the feeding vessel also supplies the anterior spinal artery, assessed by arteriography, it can potentially be embolized as a preoperative adjunct or ligated during surgery, reducing the risk of severe intraoperative hemorrhage [6]. Surgical treatment is indicated for all cases with some degree of neurological deficit. Emergency decompression with laminectomy should be performed in all cases of rapid and progressive neurological deficit, with or without the need for adjuvant radiotherapy, depending on the extent of extraosseous involvement [5,6]. In cases where the vertebral body is involved with extraosseous tumor extension into the spinal canal, causing spinal cord compression and neurological deficit, a more radical surgery such as corpectomy or intralesional spondylectomy with anterior reconstruction and posterior fixation has been advocated [9,10]. There is no formal consensus on the ideal technique. However, the literature suggests that for asymptomatic cases without neurological deficits, minimally invasive procedures are effective. In contrast, for symptomatic cases, a combination of techniques such as preembolization, posterior decompression, subtotal resection, and vertebroplasty may offer greater benefit [11-13].
An accurate and early diagnosis is crucial in cases that deviate from the described epidemiology to achieve the best possible outcomes. This is particularly true for benign lesions with potential aggressiveness, impacting survival rates, complications, and overall quality of life for patients.
Our case highlights the importance of early diagnosis and multimodal treatment, including laminectomy and radiotherapy, for managing aggressive vertebral hemangiomas with spinal cord compression. It outlines the management of the case and highlights the favorable outcome achieved for the patient.
References
- 1.Alves M, Ziegler M, Dannebrock FA, De Abreu Zardo E, Severo CM. Aggressive diffuse intraosseous hemangioma: Case report. Rev Bras Ortop (Sao Paulo) 2023;58:e952-6. [Google Scholar | PubMed]
- 2.Oliveira RP, Rodrigues NR, França AF, Galvão PE, De Campos MJ, Bello CD, et al. Report of four cases of vertebral column hemangioma with atypical evolution. Rev Bras Ortop 1996;31:119-24. [Google Scholar | PubMed]
- 3.Cloran FJ, Pukenas BA, Loevner LA, Aquino C, Schuster J, Mohan S. Aggressive spinal hemangiomas: Imaging correlates with clinical presentation, treatment algorithm analysis, and clinical outcomes. Br J Radiol 2015;88:20140771. [Google Scholar | PubMed]
- 4.Gala RB, Dhar SB, Kale SY, Ganesh R, Dahapute AA. Aggressive vertebral hemangioma causing recurring myelopathy- a rare case report and review of literature. J Orthop Case Rep 2021;11:19-22. [Google Scholar | PubMed]
- 5.Castro DG, Lima RP, Maia MA, Novaes PE, Fogaroli RC, Ferrigno R, et al. Symptomatic vertebral hemangioma treated with exclusive radiotherapy: Case report and literature review. Radiol Bras 2002;35:179-81. [Google Scholar | PubMed]
- 6.Acosta FL Jr., Sanai N, Chi JH, Dowd CF, Chin C, Tihan T, et al. Comprehensive management of symptomatic and aggressive vertebral hemangiomas. Neurosurg Clin N Am 2008;19:17-29. [Google Scholar | PubMed]
- 7.Schrock WB, Wetzel RJ, Tanner SC, Khan MA. Aggressive hemangioma of the thoracic spine. J Radiol Case Rep 2011;5:7-13. [Google Scholar | PubMed]
- 8.Aich RK, Deb AR, Banerjee A, Karim R, Gupta P. Symptomatic vertebral hemangioma: Treatment with radiotherapy. J Cancer Res Ther 2010;6:199-203. [Google Scholar | PubMed]
- 9.Fox MW, Onofrio BM. The natural history and management of symptomatic and asymptomatic vertebral hemangiomas. J Neurosurg 1993;78:36-45. [Google Scholar | PubMed]
- 10.Delabar V, Bruneau M, Beuriat PA, Zairi F, Fuentes S, Riva R, et al. Interest of a multimodal management of symptomatic vertebral hemangiomas: A report of 27 cases and literature review. Neurochirurgie 2017;63:458-67. [Google Scholar | PubMed]
- 11.Mousavi SR, Akbari S, Rasekhi A, Kazeminezhad A, Shahpari Motlagh MA, Taherpour S. A less aggressive approach to the treatment of aggressive vertebral hemangioma of the thoracic spine: A case report and literature review. Int J Surg Case Rep 2023;105:108027. [Google Scholar | PubMed]
- 12.Tafti D, Cecava ND. Spinal Hemangioma. StatPearls; 2023. Available from: https://www.statpearls.com/articlelibrary/viewarticle/30422590 [Last accessed on 2025 Mar 23]. [Google Scholar | PubMed]
- 13.Sharma S, Kamal R, Rathi AK. Vertebral hemangioma - the current radiation therapy perspective. Rep Pract Oncol Radiother 2023;28:93-101. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Synovial Hemangioma of Knee in 4-Year-Old Girl Child – A Case Report
May 1, 2025 Synovial Hemangioma of Knee in 4-Year-Old Girl Child – A Case Report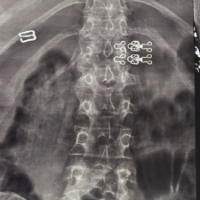 November 1, 2024 Pregnancy and Lactation Associated Osteoporosis in a 24-Year-Old Presenting with Multiple Fragility Fractures in the Dorsolumbar Spine: A Case Report and Review of Literature
November 1, 2024 Pregnancy and Lactation Associated Osteoporosis in a 24-Year-Old Presenting with Multiple Fragility Fractures in the Dorsolumbar Spine: A Case Report and Review of Literature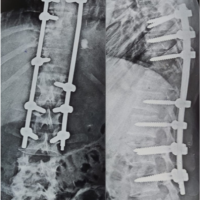 June 10, 2022 Unusual Presentation of Aggressive Hemangioma of Thoracic Vertebrae–A Case Report
June 10, 2022 Unusual Presentation of Aggressive Hemangioma of Thoracic Vertebrae–A Case Report June 27, 2021 Hemangioma of First Extensor Compartment of the Wrist– A Rare Case Report
June 27, 2021 Hemangioma of First Extensor Compartment of the Wrist– A Rare Case Report