
An unfused medial growth plate can lead to an atypical fracture pattern, this additional antero-medial fragment must be fixed appropriately to ensure adequate reduction back to the metaphysis and epiphysis to restore normal ankle anatomy
Dr. Ethan Toner, Department of Trauma and Orthopaedics, Royal Victoria Hospital, Belfast, BT12 6BA, United Kingdom. E-mail: ethantoner@doctors.org.uk
Abstract
Introduction: Triplane fractures represent a complex injury that occur at the distal tibia in the pediatric population and follow a characteristic pattern in keeping with the progressive closure of the physis typically from age 12 to 17. We present a case of a triplane variant where the medial growth plate was unfused leading to an additional mobile antero-medial fracture fragment. The rarity of our case makes this a very interesting one.
Case Report: A 16-year-old Caucasian boy presented to the emergency department after slipping on wet grass and injuring his left ankle. He was unable to weight bear. He sustained an isolated and closed injury. He had no significant medical comorbidities and was otherwise a fit and active teenager. Following initial investigations, a triplane ankle fracture was diagnosed, and he was placed into a short leg cast and referred directly to the orthopedic trauma team for admission.
Conclusion: Atypical triplane variants are rare. The presence of an additional anteromedial epiphyseal fragment separated from the metaphysis and remaining portion of the epiphysis is even rarer. We present the surgical management of such a case in our unit, with a good patient outcome.
Keywords: Pediatric fractures, atypical triplane, surgical management, trauma.
Triplane fractures represent an uncommon and complex injury that occurs at the distal tibia in the pediatric population, typically from age 12 to 17. Of all the ankle injuries affecting this group, triplane injuries account for only 6% [1,2]. Triplane fractures occur within the three planes of the distal tibia; coronally into the metaphysis, sagittally into the epiphysis and axially into the physis. This classical intra-articular fracture pattern represents a salter harris type 4 fracture. These fractures typically follow a characteristic pattern in keeping with the progressive closure of the physis. Starting with closure to the central medial part of the tibia often referred to kump’s bump and continuing laterally to the posterior tibia and finally the anterolateral tibia [3,4]. Tillaux fractures are antero-lateral avulsion fractures with the anterior inferior tibiofibular ligament attached with extension into the physis. These are thought to occur at a later age, due to this advanced closure of the physis, where only the anterolateral part is still open [5]. A Thurston-Holland fracture occurs with the fracture line extending through the physis and exits through the metaphysis. Atypical or variant patterns are rare with few reported in the literature. These atypical patterns include intra-articular fractures, which involve the non-weight-bearing area of the tibial plafond and extra-articular fractures of the medial malleolus [6,7]. However, we present a case of a triplane variant where the medial growth plate was unfused leading to an additional mobile antero-medial fracture fragment. The rarity of our case makes this a very interesting one.
A 16-year-old Caucasian boy presented to the emergency department after slipping on wet grass and injuring his left ankle with a supination inversion force as the suspected mechanism of injury. On examination, he was unable to weight bear, the skin was intact, there was tenderness of both malleoli, and marked swelling and bruising of the ankle and foot. He had no compromise to the soft tissues and was neurovascularly intact. He had no significant medical comorbidities and was otherwise a fit and active teenager. Following initial investigations with X-rays, a triplane ankle fracture was diagnosed, and he was placed into a short leg cast and referred directly to the acute orthopedic trauma team for admission.
Investigations
X-rays of the patient’s left ankle (Fig. 1), and full length tibia and fibula were performed in the ED, as well as check X-rays of the fracture position in cast. Computed tomography (CT) scan (Fig. 2) was performed to further evaluate the fracture pattern and to assist with surgical planning.

Treatment
The patient underwent surgical stabilization through an open reduction internal fixation 4 days following his injury. This was performed with an anterolateral approach, where the Tillaux fragment was first mobilized. Intraoperatively, it was noted the medial growth plate was open and with a separate mobile anteromedial fragment. The Tillaux fragment was reduced onto the distal tibia with a K-wire, followed by the anteromedial fragment being reduced onto the Tillaux fragment before being stabilized to the metaphysis using an oblique partially threaded cancellous screw across the physis. The posterior Thurston-Holland fragment was reduced with the ankle in dorsiflexion and held and an anterior-posterior screw inserted. A transverse screw distal to the physis was inserted from medial to lateral to compress the sagittal split. An additional 2nd screw was inserted into the anteromedial fragment across the physis obliquely. A long screw was passed to address the fibula fracture, intramedullary from the tip. We utilized five Stryker 4 mm ASNIS screws in total for fixation, all partially threaded cannulated cancellous screws. The post-operative check X-ray is found in Fig. 3.

Outcome and follow-up
The patient was placed into a short leg cast and immobilized non-weight bearing for a total of 4 weeks with subsequent fracture clinic follow-up. There were no initial post-operative complications.
At the 4 week stage, he was referred to physiotherapy. He was allowed to mobilize as able in an air cast boot, and to come out of the boot for basic ankle range of motion exercises for a further 2 weeks. At the 6 week stage, he was weaned from the boot into normal footwear and could weight bear as normal. Physiotherapy exercises gradually progressed from week 6.
Our case is unique as firstly the antero-medial portion of the tibial physis remained open, leaving this predisposed to separation from the metaphysis and secondly an additional fracture fragment. This anteromedial epiphyseal fragment had separated from the metaphysis and was also detached from the remaining portion of the epiphysis, making this a rare atypical triplane fracture. There was also an associated distal fibular fracture in our case. The literature suggests an associated fibular fracture which can occur in up to 50% of triplane fractures, with prevalence increasing through the use of CT scanning [8,9]. Classic fracture configurations have been described in the literature as either 2 or 3 part fractures. The lateral 2 part involves a posterolateral fragment, from the posterolateral epiphysis and posterior metaphysis, detaching from the anteromedial epiphysis which remains intact and attached to the tibia [2,5,10]. The lateral sided triplane is the most common as the lateral physis is the weakest and is also the site for the insertion of the anterior inferior tibiofibular ligament. A supination external rotation force is the typical mechanism of injury [11]. The medial 3 part involves separation of physis at kump’s bump leading to one free anterolateral epiphyseal fragment, one fragment that involves rest of epiphysis and posterior metaphysis and one main fragment off the remaining tibial metaphysis and shaft [2,5,10]. Typically, these involve an adduction force as the mechanism of injury and are less common than lateral-sided injuries [12]. In a 3 part without detachment at kump’s bump, there is one fragment of posterior epiphysis, posterior metaphysis, and a separate anterolateral epiphyseal fragment, with the antero-medial epiphysis still attached to the tibial metaphysis [2,5,10]. With our case, this separated anteromedial epiphyseal fragment as described, has been reported in some of the literature as extremely rare or regarded as non-existent [7,13-17]. The presence of a persistent open growth plate antero-medially may explain this presentation. However, the separation from both metaphysis and the remaining epiphysis of the anteromedial fragment in our patient would challenge earlier findings from Kleiger and Mankin, and similarly, Clement and Worlock, who reported on a variant in cases with an open growth plate, stating that the medial hump stabiles the anteromedial part of the epiphysis in a manner similar to the partial anteromedial fusion [3,4]. A more recent study by Prijs et al., utilizing CT scans to determine fracture patterns in triplane injuries challenged this theory on the medial hump, suggesting that the deltoid ligament or medial fusion may lead to greater variations in a medial fracture line and may not solely be related to the weakness of the physis [18].
Atypical triplane variants are rare. The presence of an additional anteromedial epiphyseal fragment separated from the metaphysis and remaining portion of the epiphysis is even rarer. This could be due to possible weakness associated with an unfused medial growth plate. This fragment should be appropriately reduced intraoperatively to restore normal ankle anatomy. We present the surgical management of such a case in our unit, with a good patient outcome.
Overall making surgical decisions in such a case can be challenging. We advocate the use of CT scanning for pre-operative planning. Intraoperative findings of an unfused medial growth plate should lead to consideration of an additional fracture fragment. Each element of a triplane injury should be assessed and undergo appropriate reduction and surgical fixation to restore congruity of the articular surface and to optimize outcomes.
References
- 1.Cooperman DR, Spiegel PG, Laros GS. Tibial fractures involving the ankle in children. The so-called triplane epiphyseal fracture. J Bone Joint Surg Am 1978;60:1040-6. [Google Scholar | PubMed]
- 2.Cancino B, Sepúlveda M, Birrer E. Ankle fractures in children. EFORT Open Rev 2021;6:593-606. [Google Scholar | PubMed]
- 3.Kleiger B, Mankin HJ. Fracture of the lateral portion of the distal tibial epiphysis. J Bone Joint Surg Am 1964;46-A:25-32. [Google Scholar | PubMed]
- 4.Clement DA, Worlock PH. Triplane fracture of the distal tibia. A variant in cases with an open growth plate. J Bone Joint Surg Br 1987;69-B:412-5. [Google Scholar | PubMed]
- 5.Dias LS, Giegerich CR. Fractures of the distal tibial epiphysis in adolescence. J Bone Joint Surg Am 1983;65-A:438-444. [Google Scholar | PubMed]
- 6.Yung CS, Kuong EE, Chow W. A previously unreported type of extra-articular triplane fracture: A revised classification system. J Orthop Surg (Hong Kong) 2019;27:2309499019828500. [Google Scholar | PubMed]
- 7.Nel JH, Nel CF. Atypical triplane fracture-anteromedial epiphyseal sleeve avulsion pattern. Cureus 2021;13:e17934. [Google Scholar | PubMed]
- 8.Ertl JP, Barrack RL, Alexander AH, VanBuecken K. Triplane fracture of the distal tibial epiphysis. Long-term follow-up. J Bone Joint Surg Am 1988;70:967-76. [Google Scholar | PubMed]
- 9.Jones S, Phillips N, Ali F, Fernandes JA, Flowers MJ, Smith TW. Triplane fractures of the distal tibia requiring open reduction and internal fixation. Pre-operative planning using computed tomography. Injury 2003;34:293-8. [Google Scholar | PubMed]
- 10.Brown SD, Kasser JR, Zurakowski D, Jaramillo D. Analysis of 51 tibial triplane fractures using CT with multiplanar reconstruction. AJR Am J Roentgenol 2004;183:1489-95. [Google Scholar | PubMed]
- 11.Kay RM, Matthys GA. Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-78. [Google Scholar | PubMed]
- 12.Wuerz TH, Gurd DP. Pediatric physeal ankle fracture. J Am Acad Orthop Surg 2013;21:234-44. [Google Scholar | PubMed]
- 13.Feldman F, Singson RD, Rosenberg ZS, Berdon WE, Amodio J, Abramson SJ. Distal tibial triplane fractures: Diagnosis with CT. Radiology 1987;164:429-35. [Google Scholar | PubMed]
- 14.Denton JR, Fischer SJ. The medial triplane fracture: Report of an unusual injury. J Trauma 1981;21:991-5. [Google Scholar | PubMed]
- 15.Seitz WH Jr., LaPorte J. Medial triplane fracture delineated by computerized axial tomography. J Pediatr Orthop 1988;8:65-6. [Google Scholar | PubMed]
- 16.Karrholm J. The triplane fracture: Four years of follow-up of 21 cases and review of the literature. J Pediatr Orthop B 1997;6:91-102. [Google Scholar | PubMed]
- 17.Ogden J. Distal Epiphyseal and Physeal Injuries. New York: Springer Verlag; 2000. [Google Scholar | PubMed]
- 18.Prijs J, Rawat J, Ten Duis K, IJpma FF, Doornberg JN, Jadav B, et al. Triplane ankle fracture patterns in paediatric patients. Bone Joint J 2023;105-B:1226-32. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report
August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report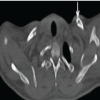 July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report
July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report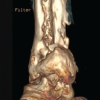 July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report
July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report March 1, 2026 Double Whammy: Rare in-Tandem Impalement Injuries to Ipsilateral Knee and Ankle in a Rural Farmer – A Case Report
March 1, 2026 Double Whammy: Rare in-Tandem Impalement Injuries to Ipsilateral Knee and Ankle in a Rural Farmer – A Case Report