
Spindle cell tumor of the flexor tendon sheath of the foot in a young male is a rare entity and should not be misdiagnosed due to its malignant potential. Timely removal and histopathological confirmation are mandatory in the management of these tumors.
Dr. Vivek Maurya, Department of Orthopedics, Suyog Hospital, Nagpur, Maharashtra, India. E-mail: vivek.vom@gmail.com
Abstract
Introduction: Spindle cell tumors are tumors consisting of spindle cells that are long and slender cells when viewed under a microscope. Their incidence is low and usually benign in nature, although it may turn malignant rarely. Histopathological diagnosis is gold-standard for diagnosis although Fine needle aspiration cytology (FNAC) and magnetic resonance imaging (MRI) may help in narrowing down the diagnosis pre-operatively. Complete tumor excision is the mainstay for managing these tumors.
Case Report: A 15-year-old male presented to our outpatient department with complaints of pain and swelling over the plantar aspect of his right foot for 4 months. Overlying skin showed no signs of adherence or local inflammation. An ultrasound-guided FNAC gave a provisional diagnosis of a benign spindle cell tumor. MRI showed a tumor arising from the 3rd flexor digitorum longus tendon sheath. A tumor excision was done and a biopsy confirmed the diagnosis. There have been no signs of recurrence since the past 12 months.
Conclusion: A benign spindle cell tumor arising from the flexor tendon sheath in the foot is a rare soft tissue tumor. However, it should be kept as a differential diagnosis in a benign soft tissue swelling in a young male requiring timely excision. Regular follow-up is needed to rule out recurrence.
Keywords: Spindle cell tumor, flexor digitorum longus, biopsy.
Soft tissue tumors are a highly heterogeneous group of tumors classified by the line of differentiation, according to the tissue they resemble [1]. Their incidence is difficult to estimate with benign tumors being relatively more common than malignant [2]. Spindle cell tumors constitute an important component of soft tissue tumors. They are characterized histologically by a mixture of fat cells and fibroblast-like spindle cells in a matrix of collagen and mucoid material. Morphologically they can be benign, borderline, or malignant and their rarity can be a source of great diagnostic confusion [3]. Across our review of the literature, a limited number of cases have been described in the foot and ankle, and hence reporting of such cases is important for awareness. In this case report, we present a case of Spindle cell tumor arising from the 3rd flexor digitorum longus tendon sheath and its management.
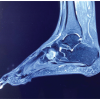
A 15-year-old male presented to our outpatient department with complaints of pain and swelling over the plantar aspect of his right foot for 4 months. Initially, the pain was manageable with non-steroidal anti-inflammatory drugs and the patient didn’t seek any medical attention. However, over the past 2 months, he complained of an increase in the severity of pain as well as the size of his swelling He also complained of having difficulty wearing his footwear and weight bearing on the right limb. Based on the local examination, he had a localized diffuse swelling between the 2nd and 3rd web space. The swelling was tender on palpation with pain elicited on flexion of 3rd toe. A soft tissue tumor was suspected involving the flexor tendon after the initial assessment and the patient was referred for a magnetic resonance imaging (MRI) of the right foot. MRI results showed a soft tissue mass intimately associated with the 3rd flexor digitorum longus tendon with anatomic location and signal characteristics most consistent with a fibroma of the tendon sheath with high suspicion of a Giant Cell Tumor. To confirm the suspicion, a Fine needle aspiration cytology (FNAC) was carried out which showed the presence of a spindle cell tumor. After reviewing the MRI and FNAC with the patient and family, a procedure to excise the tumor was carried out as the patient was in continuous pain. After obtaining all the necessary consents, surgical intervention was carried out.
Surgical technique
Under all aseptic pre-cautions patient’s foot was painted and draped. A supine position was used with the patient under a tourniquet. A lazy S-shaped incision of approximately 7 cm was taken between the 2nd and 3rd digits. Skin and subcutaneous tissue were dissected and soft tissue tumor exposed. Soft tissue mass was well encapsulated and was arising from the flexor digitorum longus tendon sheath of 3rd toe. The vascular leash of the tumor was cauterized and the tumor was meticulously excised off from the tendon sheath without any damage to the underlying tendon. The integrity of flexor digitorum longus tendon was checked and maintained. After a thorough wound wash soft tissue and skin were closed in layers. The excised soft tissue mass was sent for histopathological examination thereafter (Fig. 1-3).


Post-operative recovery
The patient was put on a below-knee splint for soft tissue healing and encouraged to weight bear over a walker boot. Suture removal was done at the end of 3 weeks. No complications were noted and the patient was encouraged full weight bearing without the walker boot thereafter. He has been pain-free for the past 12 months with no evidence of recurrence.
Histopathological findings:
- Spindle cell tumor with cells arranged in fascicles. Mitosis was 1/10 hpf
- No evidence of necrosis, atypia, or malignancy
- Features consistent with benign spindle cell tumor (Fig. 4 and 5).

The Fibroma of the tendon sheath arising from the synovium of the tendon sheath is a benign fibroblastic nodular neoplasm [4]. On histological examination, the tendon sheath typically demonstrates layers continuous with the outer fibrous tendon sheath and the inner synovial sheath layer with vessels. The recurrence rate is up to 24% of cases and is predominantly benign. The lesions nearly always originate in the distal portions of the extremities [5-7]. In the study by Maitra et al. and Rekhi et al., spindle cell lesions constituted 62% and 47.2% of all soft tissue tumors, respectively [8,9]. Both spindle cell and giant cell components may be seen in the immunophenotyping of fibroma and stain positive for Vimentin, Leukocyte-common antigen, CD68, HAM56, AACT, and MAC3387 [6,7]. Pathological and immunohistochemical tests are critical for the confirmatory diagnosis. β-Catenin and the application of Ki-67 have an important role in the identification of spindle cell tumors [10,11]. In our case, the diagnosis still requires immunohistochemical confirmation. Spindle cell tumors have a male preponderance seen most commonly between the 3rd and 5th decade of life [6]. Male-to-female incidence ratios of 1.8:1 and 1.3:1 were reported by Rekhi et al [9]. and Tailor et al., [12] respectively. Maximum cases were reported in the upper limb by Tailor et al., in the head-and-neck by Rasool et al., [13] and in the lower limb by Kotwal et al. [14]. Thus there is variable site of occurrence as evident from these studies. These tumors are predominantly benign in nature as seen from studies by Tailor et al. [12] and Kotwal et al. [14] in which incidence was found to be 93.5% and 82.3%, respectively. Rani et al. [15] found schwannoma (30.8%) as the most common spindle cell tumor. Similarly, schwannoma was also the most common spindle cell tumor found in a study by Rasool et al. [13]. Management options include non-operative as well as operative interventions. Non-operative management as primary management would simply treat symptoms. Surgical management is the only way to manage these tumors and delay in their removal may lead to deeper penetration affecting neurovascular structures [4,6]. Malignant transformation though rare is still a theoretical possibility [6]. If the tumor affects the neurovascular bundle urgent removal is mandatory [16]. Unlike other studies, we found a tumor in a rare location over the flexor digitorum longus tendon of the 3rd toe on weight-bearing area which was missed for 4 months. Although MRI showed high suspicion of a giant cell tumor, FNAC, and excisional biopsy confirmed a rare spindle cell tumor as the diagnosis.
This case demonstrates a rare lesion with only a few literature reviews seen in the field of foot and ankle. Timely removal with a biopsy of the specimen is important to rule out malignant neoplasm. A limitation in our study was immunohistochemical typing, which can further strengthen our diagnosis. The learning point of the article is that Spindle cell tumor should be considered as a differential diagnosis in a young male with soft tissue-associated metatarsalgia.
Spindle cell tumor though rare can occasionally occur arising from tendon sheath. FNAC and biopsy should be carried out in all suspected cases as they may rarely turn out to be malignant.
References
- 1.Goldblum JR, Folpe AL, Weiss SW. Enzinger and Weiss’s Soft Tissue Tumors, General Considerations. 6th ed., Ch. 1. Philadelphia, PA: Elsevier; 2014. p. 1-10. [Google Scholar | PubMed]
- 2.Akerman M, Domanski HA. Soft tissue tumors-basic information. In: The Cytology of Soft Tissue Tumors. United States: Lippincott Williams and Wilkins. [Google Scholar | PubMed]
- 3.Rosenberg AE. Bones, joints and soft tissue tumors. In: Kumar V, Abbas AK, Fausto N, editors. Robbins and Cotran Pathologic Basis of Disease. 7th ed., Ch. 26. Saunders: Elsevier; 2004. p. 1273-324. [Google Scholar | PubMed]
- 4.Fox MG, Kransdorf MJ, Bancroft LW, Peterson JJ, Fleming DJ. MR imaging of fibroma of tendon sheath. AJR Am J Roentgenol 2003;180:1449-53. [Google Scholar | PubMed]
- 5.Chung EB, Enzinger FM. Fibroma of tendon sheath. Cancer 1979;44:1945-54. [Google Scholar | PubMed]
- 6.Chen CH, Wu T, Sun JS, Lin WH, Chen CY. Unusual causes of carpal tunnel syndrome: Space occupying lesions. J Hand Surg Eur 2011;37:14-9. [Google Scholar | PubMed]
- 7.Maluf HM, DeYoung BR, Swanson PE, Wick MR. Fibroma and giant cell tumor of tendon sheath: A comparative histolog-ical and immunohistological study. Mod Pathol 1995;8:155-9. [Google Scholar | PubMed]
- 8.Maitra A, Ashfaq R, Saboorian MH, Lindberg G, Gokaslan ST. The role of fine-needle aspiration biopsy in the primary diagnosis of mesenchymal lesions. Cancer Cytopathol 2000;90:178-85. [Google Scholar | PubMed]
- 9.Rekhi B, Gorad BD, Kakade AC, Chinoy RF. Scope of FNAC in the diagnosis of soft tissue tumors-a study from a tertiary cancer referral center in India. Cytojournal 2007;4:20. [Google Scholar | PubMed]
- 10.Rakheja D, Molberg KH, Roberts CA, Jaiswal VR. Immunohistochemical expression of beta-catenin in solitary fibrous tumors. Arch Pathol Lab Med 2005;129:776-9. [Google Scholar | PubMed]
- 11.Deyhimi P, Arefian MR, Mahzouni P. Comparative analysis of the histopathologic features, β-catenin, and Ki67 expression between fibromatosis and fibrosarcoma. J Dent (Shiraz) 2019;20:255-63. [Google Scholar | PubMed]
- 12.Tailor HJ, Bhagat VM, Kaptan KB, Italiya SL, Balar HR, Agarwal MP. Diagnostic accuracy of fine needle aspiration cytology in soft tissue tumours: Our institutional experience. Int J Res Med Sci 2013;1:443-7. [Google Scholar | PubMed]
- 13.Rasool Z, Bhat ML, Nuzhat S, Khalil B, Rumana M, Ruby R, et al. Utility of fine needle aspiration cytology in diagnosis of soft tissue lesions with histopathological correlation. Glob J Med Public Health 2013;2:1-7. [Google Scholar | PubMed]
- 14.Kotwal S, Gupta D, Suri J. Role of fine needle aspiration cytology in diagnosis of soft tissue tumors; benefits and limitations: A two year retrospective study. J Evid Based Med Healthc 2016;3:1019-24. [Google Scholar | PubMed]
- 15.Rani D, Rastogi K, Gupta A. Cytomorphological study of mesenchymal spindle cell lesions of soft tissues by fine needle aspiration cytology. Indian J Pathol Oncol 2018;5:542-7. [Google Scholar | PubMed]
- 16.Lu H, Chen Q, Shen H, Shen X, Wu S. Fibroma of tendon sheath in planta. SpringerPlus 2016;5:575. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management
May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management April 1, 2025 Soft Tissue Sarcoma Masquerading as Chronic Hematoma: A Case Report and Literature Review
April 1, 2025 Soft Tissue Sarcoma Masquerading as Chronic Hematoma: A Case Report and Literature Review October 1, 2024 Novel Technique for Biopsying Osteofibrous Dysplasia Using a Vacuum-assisted Bone Harvester: A Case Report
October 1, 2024 Novel Technique for Biopsying Osteofibrous Dysplasia Using a Vacuum-assisted Bone Harvester: A Case Report March 10, 2020 Unusual Presentation of a Swelling in the Achilles Tendon After an Acute Rupture: A Case Report
March 10, 2020 Unusual Presentation of a Swelling in the Achilles Tendon After an Acute Rupture: A Case Report