
Large osteochondral fracture fixed with an innovative technique.
Dr. Chiranjeevi .K.P Department Of Orthopaedics, Apollo Hospital, Plot #13, Parsik Hill Road, off Urban Road, opp.Nerul Wonder park, sector 23, CBD Belapur, Navi Mumbai, Maharashtra-400614,India. Email: chiranjeevipirabhu@gmail.com
Introduction: Osteochondral fractures of the patella are rare injuries that can result from trauma or patellar dislocation, often affecting adolescents involved in sports.
Materials and Methods: This is the case report of a 15-year-old male presented on May 5, 2023 with a large osteochondral fracture of the patella. The patient was followed up for 2 years post-fixation.
Discussion: We describe a case of a 15-year-old male who had sustained a large medial facet patellar osteochondral fracture while playing. The diagnosis was made with the help of an X-ray, MRI, and CT scan. Fracture fixation was done with a innovative technique of extra-articular K-wires and absorbable sutures.
Conclusion: Early diagnosis and operative fixation can give excellent functional outcomes.
Keywords: Osteochondral fracture, medial facet of patella, internal fixation.
Osteochondral fractures (OCFs) of the patella are uncommon but clinically important injuries, often associated with acute trauma such as direct impact or lateral patellar dislocation. These injuries typically involve the articular cartilage and underlying subchondral bone, with the potential to cause joint incongruity, instability, and accelerated degeneration if left untreated. They are most frequently encountered in adolescents and young adults, particularly those involved in contact sports. Timely diagnosis, often aided by radiological investigations such as X-ray and computed tomography scan is essential to guide appropriate management. This report presents a case of a traumatic large patellar OCF (3.5 cm) involving almost the whole of the medial patellar facet in a healthy adolescent male, with successful surgical fixation and recovery.
A 15-year-old healthy male and an active footballer, presented to the emergency department with acute right knee pain and swelling after a non-contact twisting injury during a Football game. At the time of injury he felt a “snap”, followed by severe pain and inability to bear weight. On clinical examination, there was marked effusion, tenderness over the medial patella, and a restricted range of motion. Ligamentous testing was limited due to pain but showed no obvious instability. No previous history of patellar dislocation. Initial radiographs of the knee revealed an osseous fragment adjacent to the medial femoral condyle, raising suspicion for an intra-articular loose body (Fig. 1) .CT scan of the knee confirmed a 3.5 cm OCF originating from the medial facet of the patella (Fig. 2). The medial patellofemoral ligament was sprained as confirmed with MRI knee and cruciate ligaments were intact.

Surgical technique
- under LMA
- A pneumatic tourniquet was applied.
- A midline longitudinal skin incision was made above the patella .medial parapatellar approach. No ovious tears were noted in MPFL. Hematoma evacuated. Clots at the fracture ends were debrided and the fracture pattern was visualized.
- Patella everted, bed cleared, and cleaned (Fig. 1).
- Fracture fragment of size 3.5 cm seen as a loose body (Fig. 2 and 3).

- The fracture bed and fracture fragment were made rough by drilling multiple times using 2 mm K wire for 1 to 2 mm depth (Fig. 4).
- Fracture fragment was reduced with digital pressure and fixed with 3 extraarticular K wires (2 K-wire from post-inferior margin to antero superior and 1 from postero superior to anteroinferior margin in the coronal plane) (Fig. 5).
- Wire entry taken on the extra-articular margin and made exit from the anterior extra-articular surface.
- One drill hole was made through the lateral facet and direct double vicryl 2-0 tied (Fig. 6).
- Vicryl no 2 was put in the figure of 8 fashion along with k wire (Fig. 7).
- All 3 extra-articular K-wires – bent and cut over ant surface.so can be easily removed without arthrotomy if required.
- Wound wash was given. (Fig.8).
- Fixation was found to be satisfactory under C-arm and stable during flexion and extension. The extrarticular K wires were bent and cut. Medial parapatellar arthrotomy wound closed.(Fig. 9).

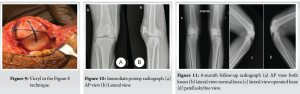
Postoperative radiographs were satisfactory (Fig. 10a and b) Immediate postoperatively, the patient was placed in a long knee brace with early initiation of passive range of motion. Knee Flexion up to 90° for 2 weeks followed by the full range of motion. Partial weight-bearing was initiated at 4 weeks followed by full weight-bearing by 6th week. The patient was regularly followed up. At the 6-month follow-up, the post-operative X-rays were satisfactory (Fig. 11a-d). However, mild patellar tilt was noted in the skyline radiograph, and the patient was advised MPFL reconstruction if symptomatic in the future. The patient clinically had no instability. The patient went on to have a full recovery and had resumed low/moderate-impact physical activity, and sports without restriction or complaints by 9 months. The knee ROM at the final follow-up was from 0° to 140° and he is completely pain-free (Fig. 12a-d). 2 year followup radiograph (Fig. 13a and b).


Younger age group are at more at risk of developing Traumatic OCF of the patella [1]. The medial facet of the patella is reported to be the most common area of patellar OCF in these patients [2]. Adolescent patients Most of the time, AP and lateral radiograph views of the knee are sufficient for reaching a diagnosis as in this case [3]. MRI-based study in patients with acute patellar dislocations showed OCF occurred in 76% of patients [4]. Advanced imaging like CT scan is often necessary for detailed visualization, and measurements of fracture fragments. Furthermore, MRI offers detailed visualization of both bony and cartilaginous components. Lee et al. did a diagnostic arthroscopy and if the fragment was big enough it was fixed with bioabsorbable pins and headless screws and if the fragment was small it was simply excised [5]. The decision between conservative versus surgical management depends on the size, location, and displacement of the fragment. Headless screws carry a risk of causing local friction and irritation and concluded that absorbable or adhesive fixation methods should be considered as alternatives [6]. Hsu et al. also had to remove headless screws as the patient could not squat and dur to implant irritation at 1 year [7]. Nuelle et al. alternatively used 3 biodegradable suture anchors [8]. Alosaimi et al. used suture anchors in the treatment of isolated OCF of patella in a 11-year-old and achieved good functional outcome [1]. The use of “hybrid techniques” as advised by Weber CD et al. propses it may increase the amount of hyaline cartilage and native subchondral bone [9]. We used an open technique over arthroscopy because of a large fracture fragment. With our technique of open fixation with k wires and figure of ‘8’ vicryl sutures anatomical reduction is maintained. The idea behind using an absorbable suture was that after the fracture is fused the sutures will be absorbed and won’t affect or erode the joint surface. The K wires used are extra-articular and can be removed in the future if indicated. We’ve managed to get a satisfactory result with this fixation. Postoperative rehabilitation must balance protection of the repair site with early mobilization to prevent stiffness. Our patient demonstrated a favorable outcome, reinforcing the importance of timely intervention and structured rehabilitation. Chances of a trivial trauma causing an OCF should be kept in mind in young adults with hemarthrosis and knee pain [10].
Patellar OCFs, although rare, require a high index of suspicion following acute knee trauma. Prompt imaging and appropriate surgical management can lead to excellent outcomes, particularly in young, active individuals. Early diagnosis and intervention are key to preserving knee function and preventing degenerative changes. Our innovative technique is cost-effective and easily reproducible while also achieving good functional outcome.
Early diagnosis and operative fixation with our innovative technique which is is cost effective and easily reproducible can give excellent functional outcomes in these cases.
References
- 1.Alosaimi MN, Almutairi MM, Alshahrani SM, Alqahtani MN, Alghamdi AS. Osteochondral fracture of the patella without soft tissue injury and with no dislocation: A case report. Int J Surg Case Rep 2021;78:48-53. [Google Scholar | PubMed]
- 2.Keshkar S, Dey N, Kumar R. Osteochondral fracture of patella. J Orthop Traumatol Rehabil 2014;7:91. [Google Scholar | PubMed]
- 3.Unal M, Tatari H. The largest osteochondral fracture of patella, case report. Austin J Orthopade Rheumatol 2014;1:2. [Google Scholar | PubMed]
- 4.Seeley MA, Knesek M, Vanderhave KL. Osteochondral injury after acute patellar dislocation in children and adolescents. J Pediatr Orthop 2013;33:511-8. [Google Scholar | PubMed]
- 5.Lee BJ, Christino MA, Daniels AH, Hulstyn MJ, Eberson CP. Adolescent patellar osteochondral fracture following patellar dislocation. Knee Surg Sports Traumatol Arthrosc 2013;21:1856-61. [Google Scholar | PubMed]
- 6.Aydoğmuş S, Duymuş TM, Keçeci T. An unexpected complication after headless compression screw fixation of an osteochondral fracture of patella. Case Rep Orthop 2016;2016:7290104. [Google Scholar | PubMed]
- 7.Hsu TL, Lin SM, Chang CH, Lan TY. Neglected pediatric osteochondral fracture dislocation of the patella. Case Rep Orthop 2019;2019:2904782. [Google Scholar | PubMed]
- 8.Nuelle CW, Nuelle JA, Balldin BC. Open reduction internal fixation of a traumatic osteochondral lesion of the patella with bioabsorbable screw fixation. Arthrosc Tech 2019;8:e1361-5. 9. Weber CD, Migliorini F, Hildebrand F. Reconstruction of large osteochondral lesions in the knee: Focus on fixation techniques. Life (Basel) 2021;11:543. [Google Scholar | PubMed]
- 9.Bhatt J, Montalban AS, Wang KH, Lee HD, Nha KW. Isolated osteochondral fracture of the patella without patellar dislocation. Orthopedics 2011;34:54. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report
February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report February 1, 2026 Medial Epicondyle Fractures Treated with Diverse Fixation Techniques: A Case Series
February 1, 2026 Medial Epicondyle Fractures Treated with Diverse Fixation Techniques: A Case Series December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis
December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System