
An epidemiological study, which highlights various treatment options in acute hand injury cases.
Dr. Mantu Jain, Department of Orthopaedics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. E-mail: montu_jn@yahoo.com
Objectives: This retrospective observational study was conducted to emphasize on epidemiological demographics and management of patients presenting with acute hand injuries to the Plastic Surgery and Emergency department and study the functional outcome of such injuries post-intervention.
Materials and Methods: The present observational study was conducted on 118 patients who had presented with hand injuries from July 2020 to December 2021 with the objectives to determine their demographic characteristics, their severity using hand injury severity scoring system. Functional outcome assessment was done using two-point discrimination for the sensory, while Purdue Pegboard Test and Jebsen-Taylor hand function test were used for the motor assessment of these patients.
Results: In the present study, males were more affected than females (M: F = 5.5:1), with the majority of the patients sustained multiple injuries involving different components of the hand in 38.1% patients, and with the most common mode of injury being machine cut injuries in 40.7% patients (P < 0.049).
Conclusion: Since it was a prospective study, there was a major correlation between the gender and mode of injury, especially males getting more affected than females. The severity of hand injury showed a significant association with the functional outcome of the hand.
Keywords: Hand injury, observational study, epidemiology, hand function, functional outcome of hand.
Injuries cause major impact on the mortality and morbidity throughout the world [1]. According to the World Health Organization, the Global Health Estimates in 2000-2019, revealed deaths caused due to injuries were estimated to be around 4.4 million and the injury accounted for around 8% of total deaths worldwide [2]. The global burden of disease has been projected to decrease from all causes from 2004 to 2030 but the global number of deaths caused by injuries have increased from 12.3% to 28% between 2004 and 2030 [1,2]. Hand is important to us because we require it to grip objects and perform various tasks both at leisure and at work. This fine sensibility and greater cosmetic importance are very important for hand function in everyday life. Another important aspect of hand function is the difference in dexterity which is often present between the dominant and non-dominant hand. Normal simple tasks, such as using a pen for writing and holding a glass properly becomes difficult immediately post-injury.
The hand, being the terminal segment of the upper limb, is the most crucial part due to its ability to resist, to create powerful gross action, and to perform intricate fine movements in several planes, which reflects the masterful construction of its supporting architecture. Trauma to the hand, therefore, results in impairment to normal daily activity, with sequelae resulting in more serious complications, and patients recover gradually over several months. Thus, management of hand injuries is difficult and requires early and prompt treatment.
They are common in every age group and pertaining to both genders equally. Bearing the complexities, the biological, the behavioral pattern, and the socioeconomic burden associated with hand injuries, can help identify the individuals most at risk and define potential preventive measures to help reduce the incidence of such injuries in our day-to-day life.
There are few studies on epidemiology worldwide [3,4,5,6,7], and from some regions of India, namely, the southern and northern part of India [8,9], but there is paucity of knowledge as far studies from eastern part of India are concerned. We apprehend that change of demographic profile might contribute to change in the injury pattern and final functional outcome that can help policymakers to formulate guidelines.
A prospective, observational study was conducted on 118 patients with history of acute isolated hand injury who attended the Burns and Plastic Surgery/Trauma and Emergency/Orthopedics department from July 2020 to December 2021, of a tertiary care hospital in eastern India. Informed written consent was taken from all the patients included in this study along with the Institutional Ethical Committee (IEC/AIIMS BBSR/2019-20/64) approval before the start of the study. The patient’s demographic profiles were included, such as age, sex, mode of injuries, timing of presentation, type of injury, hand injury severity scoring system (HISS), the treatment (interventions, such as primary suturing of wound, fracture fixation using Kirschner (K) wires/miniplates/pins, repair of tendons and vascular structures, and soft tissue reconstruction using grafts or loco-regional flaps) Chronic wounds, hand injuries that occurred due to infections, burns, amputations were excluded from the study.
All the patients were followed up at regular intervals for a minimum period of three months for assessment of hand function. Two-point discrimination was assessed to evaluate the sensory outcome and motor assessment were done using Purdue Pegboard Test to evaluate manual dexterity and activities of daily living were measured using Jebsen-Taylor Hand function test. The range of motion at the joints was assessed using a goniometer.
Statistical analysis
The characteristics of the injury were described using proportions for categorical variables and using Mean ± Standard deviation and median interquartile range (IQR) for continuous variables. 95% confidence interval for important characteristics was also provided. The Statistical Package for the Social Sciences version 25 was used for statistical analysis. Pearson Chi-square test was used to validate associations between independent variables and data documentation of each patient was done using the Microsoft Excel format. A P = 0.05 or low was taken as statistically significant value.
In the present observational study of 118 patients, 84.7% were males, while 15.3% were females (Male: Female ratio = 5.5:1), showing a significant male preponderance. The majority of the patients (37.3%) belonged to 16–30 years of age group, with the least incidence observed in 5.2% patients, whereas the mean age of the study subjects was 33.8 ± 14.4 years. All the study subjects showed right-hand dominance, which inclined them to sustain injury to the functional right hand (55.9%) more as compared to the left hand (43.3%). The majority of the patients sustained multiple injuries involving different components of hand in 38.1% patients and with the most common mode of injury being machine cut injuries in 40.7% patients occurring mostly at the workplace areas (Table 1).
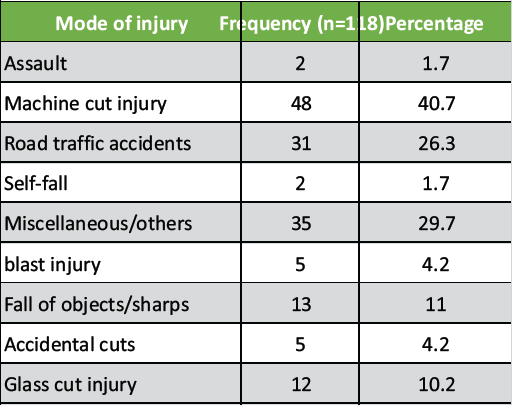
Table 1: Mode of injury of patients
A positive correlation is depicted between the gender and the mode of injury with the P = 0.049. Around 56% patients reported to the hospital within 1–6 h of injury with the median duration being 240 min (4 h) and the median duration of hospitalization was 4.50 days among the admitted patients (Table 2).
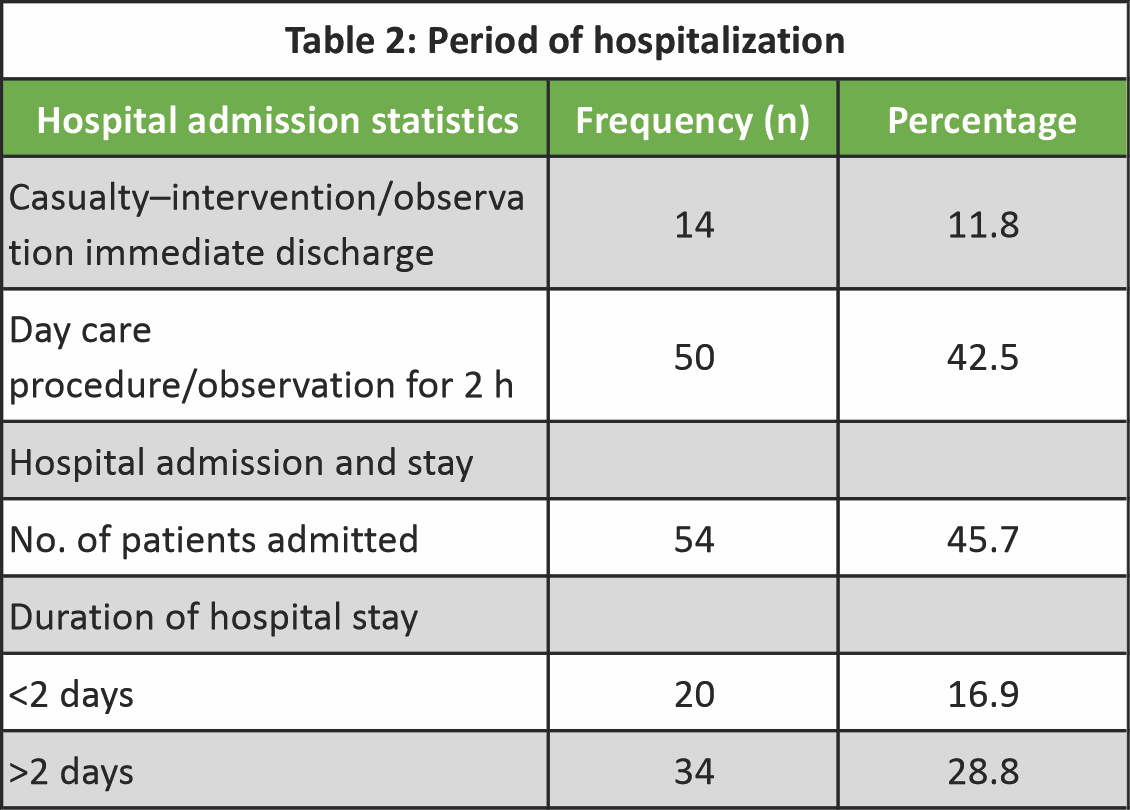
Table 2: Period of hospitalization
96 patients had isolated finger injuries, with the index finger and distal phalanx being most commonly affected followed by other digits. Table 3 enlists the treatment modalities offered to the injured patients.
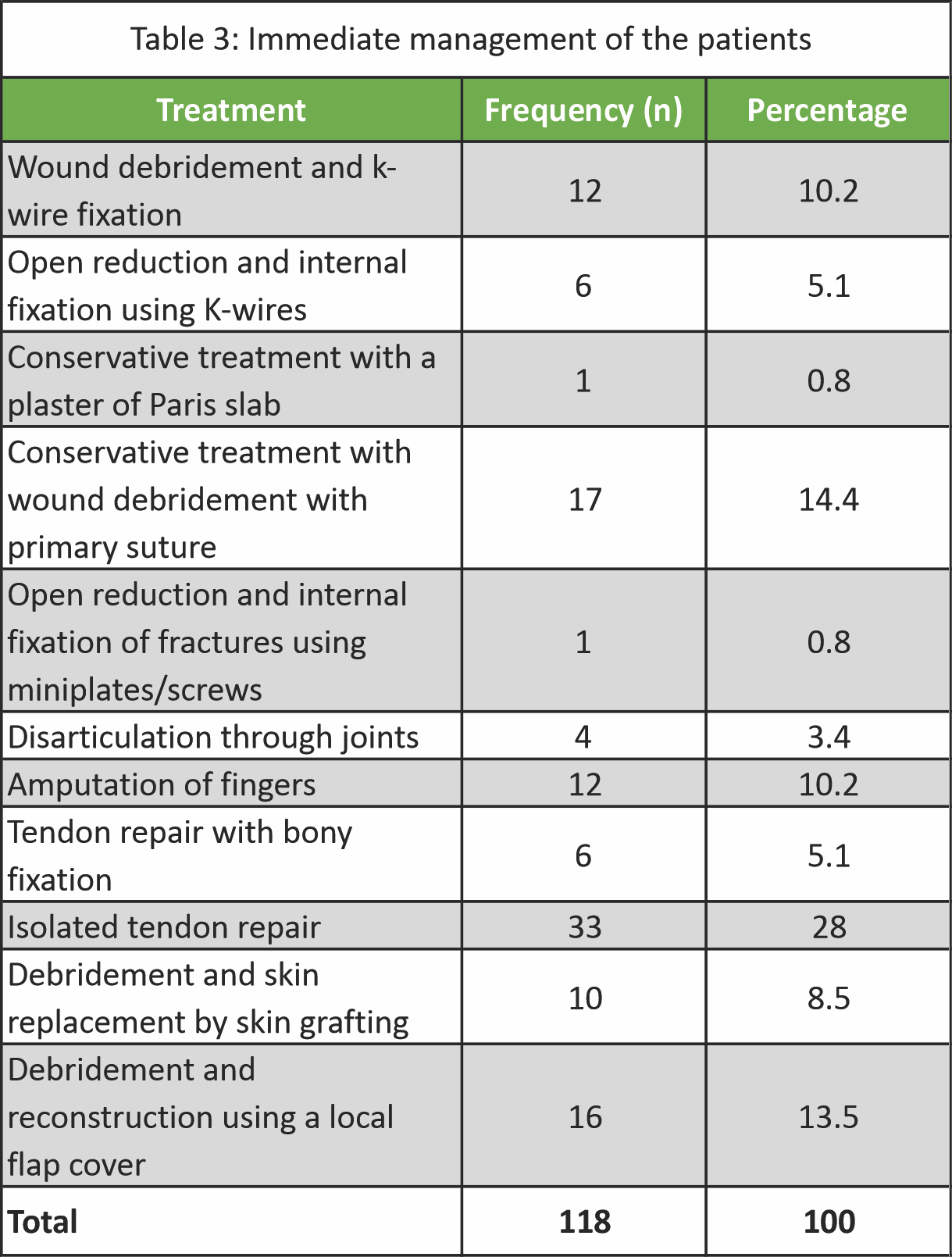
Table 3: Immediate management of the patients
The major complication reported in the study was flap necrosis, while joint stiffness, wound dehiscence, swelling and hypertrophic scar were also reported in few patients in the study but majority (97%) of patients did not complain of any post-operative complication. Out of the 118 patients, forty-six patients were under the influence of alcohol at the time of injury. Fourteen patients were hypertensive, seven being diabetic and eight patients had both the co-morbidities in the study. The severity scoring of the patients using the anatomical HISS system revealed that majority (38 patients) had moderate scores followed by 32 patients who reported major scores of >101, 27 patients of <20 minor score value and 26 patients had severe scores, resulting in median IQR level of 50 (21–114.75).
The correlation between the anatomical HISS scoring values and the post-operative Purdue Pegboard test, which showed statistically significant values in the left hand with P = 0.017 at 1 week and 0.005 at 1 month. The P value in combined right, left, and both hands were 0.015 in 1 week and 0.002 at 1 month (Table 4).
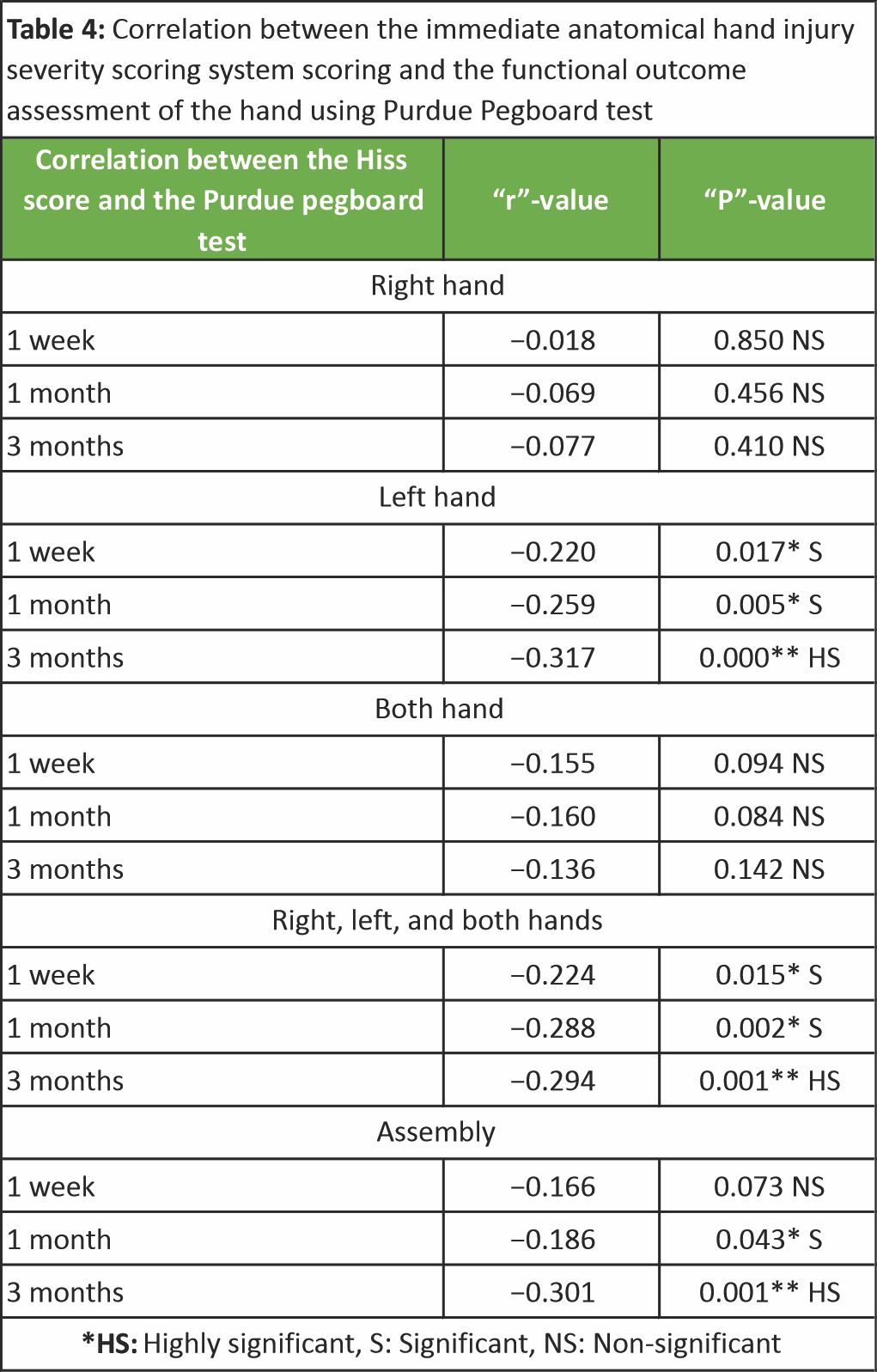
Table 4: Correlation between the immediate anatomical hand injury severity scoring system scoring and the functional outcome assessment of the hand using Purdue Pegboard test
The test helped in evaluating the function and manual dexterity of the injured hand especially at each follow-up visit. A negative association existed between HISS score and Jebsen hand function test and 2PD values which did not affect the rehabilitation protocol.
A few cases are illustrated in the Figs. 1, 2, 3, 4.

Figure 1: A-30 year/male with injury to distal phalanx of right middle finger and ring finger – caused by entrapment in cycle chain (a and b), Wound debridement (c), Raw area coverage full-thickness skin graft (groin) in (d), post-operative wound: Good take up by graft (e).

Figure 2: A 45 years male with crush injury following road traffic accidents with injuries to multiple components of hand involving interphalangeal and metacarpophalangeal. Wound debridement and primary suturing done in emergency room.

Figure 3: 25/M with Blast injury with multiple injuries (a). Immediate treatment: Wound debridement + Primary suturing (b and c) Soft tissue coverage – Groin flap (d), Flap detachment – Day 21 (e), Follow-up visit – at 3 months (f).
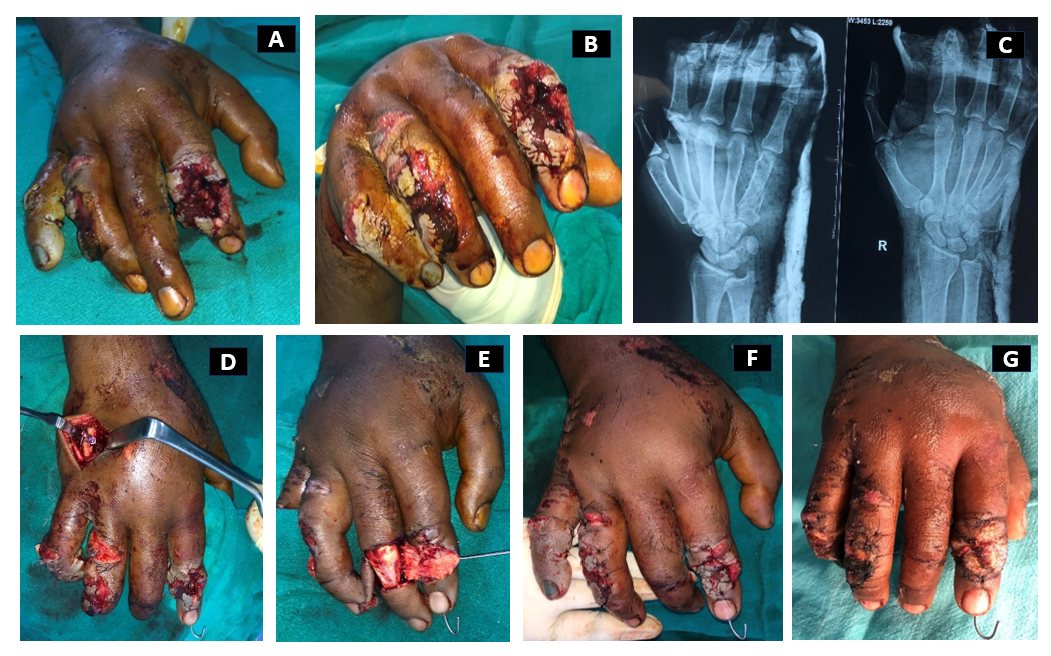
Figure 4: A 32 year male patient with crush injury following road traffic accidents involving multiple digits (a and b), X-ray – fracture middle phalanx of index finger (IF) and shaft of 5th metacarpal (MC) (c), Treatment: Wound debridement + open reduction internal fixation and K-wire fixation of IF + Miniplate screw fixation of 5th MC + local flap (cross finger flap cover) over raw area (IF) (d), Follow-up (1 month): K wire in situ + division of cross finger flap with follow-up (e-g).
The hand, being the most intricate and important tool used for performing daily activities, trauma to the hand, therefore, requires utmost attention for understanding the demographic outline, the causes, and characteristics of injury.
In our observational study based on 118 patients with a hand injury, young adults were more commonly affected between the age group of 16–30 years, with the mean age being 33.8 ± 14.4 years. Young adult males due to their recklessness, impatience while working or driving, history of alcohol or substance abuse and with significant lesser experience at work, were more prone for machine cut injuries and road traffic accidents (RTA). In our study, 55.9% had dominant (right) hand affected as compared to 43.3% incidence in non-dominant (left) hand, while only one patient had both (0.8%) hands affected.
Higher risk occurrence has been noted above the age of 35 years in the studies conducted by Rosberg et al. 2005, Trybus et al. and Sorock et al., implying that the middle age groups were more prone to get injured [7,10,11]. Two of the Indian studies, by Desai et al. and Bajracharya and Shrestha, concluded that 88% and 85.5% incidence of male patients who presented with hand injuries, respectively, showed right hand dominance, correlated with our study findings [12,13].
Power-drilled machines, grinding, or wood splinters are often the main culprits in the occupational setup. Machine cut injuries were the major contributors in 40.7% patients, followed by RTA in 26.3% patients in our study. Occupational injuries constituted 80% of cases in the study conducted in Chennai compared to 60% in the Denmark group and around 40% in the Turkish group [8,14,15]. Fractures constituted the major type of injury in a study in India (42%) and Iran (18%), projecting their incidence globally [13,16]. Fingertip injuries (82.16%) were the commonest entity in a study conducted in Foshan city, China [8].
Index finger and thumb were the commonest digits involved, around 16.9% and 15.3% involvement, respectively, with the distal phalanx (22.9%) being commonly involved in our study. Desai et al., suggested multiple digits (48.5%) were involved in their study [12]. According to study conducted by Al Zahrani et al., the distal phalanx was most commonly involved which correlated with our results [17]. De Jong et al., mentioned in their study that zone 2 extensor tendon injuries were most common among their cases unlike in our study where the predominance of zone 1 flexor tendon injuries were relatively more [18].
In 2018, Poudel et al., conducted a similar study in Nepal, which corroborated with our demographic results [19]. However, according to Moellhoff N et al., nearly half of the patients reported within 2 h of injury whereas in the study conducted by Desai et al., suggested that 54 (27%) patients reported within 1 h of injury, 125 patients (62.5%) reported within 1–6 h of injury and 21 patients (10.5%) reported after 6 h of injury [12,20]. The median duration of hospital stay was 4.50 days, while the median duration of time-lapse since presentation to hospital was 4 h (240 min) in our study population. This has not been reported earlier in any study as per the literature search. In contrast to our findings, where conservative management was employed to 17 patients (14.4%), Desai et al., suggested 35.5% of patients required conservative management in the form of wound debridement, primary suturing and plaster of Paris slab [12].
In our study, though the machine cut injuries and RTA were the main causes, domestic injuries increased during the COVID period as major decline was noticed in workplace injuries and RTA. The “Do-It-Yourself” injuries that were common during that period reported in the study conducted in Sydney during the pandemic shutdown [21].
Out of the 118 patients, the majority of the patients, 33 (28%), had a moderate level of severity, followed by a major level of severity in 32 (27.1%) patients and a minor score in 27(22.9%) patients. The median IQR level using HISS score in our study was 50 (21–114.75), respectively. Our study correlated with another study by Dębski and Noszczyk where moderate scoring was recorded in 28.6% of patients, 26.5% of cases had major scores, 25.5% with severe scores, and minor scores in 19.4% cases [22]. Our study compared males and females with HISS score with a chi-square value of (χ2 = 1.453, df = 3) at P < 0.05 level, which was statistically insignificant, thus implying the negative association between the variables. Similar findings have not been reported in any other study as yet. The correlation between HISS scoring system and Purdue Pegboard test has been done using Pearson correlation. Out of the 5 subsets, 3 subsets were positively associated with initial HISS scores, which denoted that (P < 0.005), otherwise implying statistically significant. This further clarifies that based on the anatomical scoring; hand function had fairly improved post-recovery. A similar correlation study between HISS scores and the Purdue Pegboard test has been conducted in a single study by Lee et al., They reported a negative association between the two variables [23]. As per the Pearson correlation in our study, there was a negative association between the anatomical HISS Score system and Jebsen-Taylor Hand Function test with a statistically insignificant (P > 0.05) in every follow-up visit. There has been no direct correlation study between the HISS system and the Jebsen hand function test as per the literature search. The median IQR values of two-point discrimination were reported and compared between each injured and non-injured finger in this study. There was no major difference in the values reported in our study. The data analysis done by Boesch et al., strongly supported the reliability of 2PD for assessing the hand function [24].
Limitations
There were certain limitations in our study. First, treatment bias differed for each patient according to the time lapse before presentation. Hence, the outcome of each patient differed. Second, the functional outcome assessment was very short due to the total timeline of the study period and the ongoing COVID-19 pandemic.
Young active males are predominantly affected and the mode of injury is most commonly machine cuts. There is a major correlation between the gender and mode of injury and finally, the functional outcome of the hand showed a significant association with the severity of hand injury.
The article highlights the importance of hand injuries and the understanding of their epidemiology, which has a significant impact on function, productivity, and quality of life.
References
- 1. Lindqvist A, Gerdin B. Hand injury from powered wood splitters. Scand J Plast Reconstr Surg Hand Surg 2008;42:246-52. [Google Scholar] [PubMed]
- 2. World Health Organization. Global Health Estimates: Leading Causes of Death. Geneva: World Health Organization; 2019. [Google Scholar] [PubMed]
- 3. Rosberg HE, Dahlin LB. Epidemiology of hand injuries in a middle‐sized city in southern Sweden: A retrospective comparison of 1989 and 1997. Scand J Plast Reconstr Surg Hand Surg 2004;38:347-55. [Google Scholar] [PubMed]
- 4. Wu Z, Guo Y, Gao J, Zhou J, Li S, Wang Z, Huang S, Huang S, Li Y, Chen J, He M. The epidemiology of acute occupational hand injuries treated in emergency departments in Foshan City, South China. Ulus Travma Acil Cerrahi Derg. 2018;24(4):303-310. [Google Scholar] [PubMed]
- 5. Kringstad O, Dahlin LB, Rosberg HE. Hand injuries in an older population – a retrospective cohort study from a single hand surgery centre. BMC Musculoskelet Disord 2019;20:245. [Google Scholar] [PubMed]
- 6. Junqueira GD, Lima AL, Boni R, Almeida JC, Ribeiro RS, Figueiredo LA. Incidence of acute trauma on hand and wrist: A retrospective study. Acta Ortop Bras 2017;25:287-90. [Google Scholar] [PubMed]
- 7. Rosberg HE, Carlsson KS, Dahlin LB. Prospective study of patients with injuries to the hand and forearm: costs, function, and general health. Scand J Plast Reconstr Surg Hand Surg. 2005;39(6):360-9. [Google Scholar] [PubMed]
- 8. Prasad R, Bhamidi A, Rajeswaran A, Muthukumar S, Kothandaraman P, Sivaraj M. Epidemiology and sequelae of workplace hand injuries at a tertiary trauma care centre. Surg Sci 2014;5:150-8. [Google Scholar] [PubMed]
- 9. Gupta R, Mahajan S, Dewan D, Gupta R. Pattern of hand injuries reported in a tertiary care setting of North India. Int J Res Med Sci 2017;5:880-4. [Google Scholar] [PubMed]
- 10. Trybus M, Lorkowski J, Brongel L, Hladki W. Causes and consequences of hand injuries. Am J Surg 2006;192:52-7. [Google Scholar] [PubMed]
- 11. Sorock GS, Lombardi DA, Peng DK, Hauser R, Eisen EA, Herrick RF, et al. Glove use and the relative risk of acute hand injury: A case-crossover study. J Occup Environ Hyg 2004;1:182-90. [Google Scholar] [PubMed]
- 12. Desai B, Makwana H, Shah D, Patel PR. Epidemiology of hand injuries in adults presenting to a tertiary trauma care centre: A descriptive study. Int J Orthop Sci 2018;4:434-8. [Google Scholar] [PubMed]
- 13. Bajracharya S, Shrestha S. Epidemiology of hand injuries in a tertiary care center. J Univ Coll Med Sci 2018;5:35-9. [Google Scholar] [PubMed]
- 14. Larsen CF, Mulder S, Johansen AM, Stam C. The epidemiology of hand injuries in The Netherlands and Denmark. Eur J Epidemiol. 2004;19(4):323-7. [Google Scholar] [PubMed]
- 15. Serinken M, Karcioglu O, Sener S. Occupational hand injuries treated at a tertiary care facility in Western Turkey. Ind Health 2008;46:239-46. [Google Scholar] [PubMed]
- 16. Mirzaie M, Parsa A, Salehi M, Dahmardehei M, Moghadam MH, Mirzaie N. Epidemiology of hand injuries in children presenting to an orthopedic trauma center in southeast of Iran. Arch Bone Jt Surg 2014;2:225-31. [Google Scholar] [PubMed]
- 17. Al Zahrani S, Ikram M, AL-Qattan M. Predisposing factors to industrial hand injuries in Saudi Arabia. J Hand Surg 1997;22:131-2. [Google Scholar] [PubMed]
- 18. De Jong JP, Nguyen JT, Sonnema AJ, Nguyen EC, Amadio PC, Moran SL. The incidence of acute traumatic tendon injuries in the hand and wrist: A 10-year population-based study. Clin Orthop Surg 2014;6:196-202. [Google Scholar] [PubMed]
- 19. Poudel M, Bhandari R, Uprety S, Baral D, Gupta P. Epidemiological study of road traffic accident cases in emergency department of tertiary care centre of Eastern Nepal. Asian Pac J Health Sci 2018;5:179-82. [Google Scholar] [PubMed]
- 20. Moellhoff N, Throner V, Frank K, Benne A, Coenen M, Giunta RE, Haas-Lützenberger EM. Epidemiology of hand injuries that presented to a tertiary care facility in Germany: a study including 435 patients. Arch Orthop Trauma Surg. 2023 Mar;143(3):1715-1724. [Google Scholar] [PubMed]
- 21. Ho E, Riordan E, Nicklin S. Hand injuries during COVID-19: Lessons from lockdown. J Plast Reconstr Aesthet Surg 2021;74:1408-12. [Google Scholar] [PubMed]
- 22. Dębski T, Noszczyk BH. Epidemiology of complex hand injuries treated in the Plastic Surgery Department of a tertiary referral hospital in Warsaw. Eur J Trauma Emerg Surg 2020;47:1607-12. [Google Scholar] [PubMed]
- 23. Lee CL, Wu MY, Chang JH, Chiu HY, Chiang CH, Huang MH, et al. Prediction of hand function after occupational hand injury by evaluation of initial anatomical severity. Disabil Rehabil 2008;30:848-54. [Google Scholar] [PubMed]
- 24. Boesch CE, Fuchsberger T, Beutler K, Bender D, Daigeler A, Medved F. Value of the two-point discrimination test: Evaluation of 238 isolated finger nerve injuries. J Hand Surg Asian Pac Vol 2019;24:477-82. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Bridge Plating of Second and Third Carpometacarpal Fracture Dislocations: A Case Report of Rare Injury
January 1, 2026 Bridge Plating of Second and Third Carpometacarpal Fracture Dislocations: A Case Report of Rare Injury December 1, 2025 Trends in Rheumatoid Arthritis Mortality in the United States, 1999–2020
December 1, 2025 Trends in Rheumatoid Arthritis Mortality in the United States, 1999–2020 October 10, 2022 Needle Cap External Fixator for Proximal Phalanx Fracture – A Case Report
October 10, 2022 Needle Cap External Fixator for Proximal Phalanx Fracture – A Case Report December 1, 2025 Unusual Case of Lateral Knee Pain: Magnetic Resonance Imaging Evidence of Isolated Lateral Patellotibial Ligament Enthesopathy
December 1, 2025 Unusual Case of Lateral Knee Pain: Magnetic Resonance Imaging Evidence of Isolated Lateral Patellotibial Ligament Enthesopathy