
Combining intramedullary nailing with derotation plating provides stable fixation and promotes reliable healing in distal femoral shaft fractures, with minimal complications and good functional recovery.
Ismail Pandor, Department of Orthopedics, Krishna Vishwa Vidhyapeeth, Karad, Maharashtra, India. E-mail:i.pandor07@gmail.com
Introduction: Femoral shaft fractures are highly prevalent. Surgical treatment is the optimal approach for managing them as it greatly decreases the rates of illness and death in injured people. The optimal therapy for these diseases entails the utilization of nail, plates, screws, and external fixation devices. At present, reamed intramedullary nailing is regarded as the optimal approach and universally recognized treatment indicated for fractures occurring in the shaft of the femur.
Experimental procedures and techniques: The study done at Krishna Hospital in Karad between February 2022 and July 2024 included thirty adult Individuals suffering from comminuted fractures of the femoral shaft. The group consisted of 25 males and 5 females. The age range of the participants was between 20 and 45 years.
Results: All 30 patients successfully obtained fracture union. The assessment of fracture healing was conducted by evaluating the formation of callus in the post-operative X-rays. Our analysis revealed no significant disparity in limb length. There were no instances of post-operative wound infection observed in any of the patients. No cases of plate avulsion or loosening were reported in this investigation. No patient experienced any post-operative knee or hip discomfort after undergoing combination fixation using a femur nail with derotation plate.
Discussion: By integrating femur nailing with plate augmentation, we can achieve the benefits of both methods for fixing fractures while minimizing their possible issues and downsides. The femur nail functions as a load-sharing device, counteracting the shear stresses at the fracture site and ensuring the consistent positioning of the fracture. Derotation plate fixation is used to manage excessive movement at the fracture site, ensuring stability and preventing any reduction loss.
Conclusion: A composite implant design, consisting of a combination of nailing and derotation plate, is a practical and rational choice for stabilizing fractures of the femoral diaphysis. It can be considered a viable substitute for interlocking nail fixation. Compared to the utilization of either conventional plating and screws or a solitary nail, this procedure offers a more reliable and steady fixing, hence decreasing the likelihood of reduction loss. Moreover, this approach encounters less issues. Attained stiffness is crucial for allowing prompt weight bearing and helping the recovery of patients with complex fractures.
Keywords: Intra-articular fractures, internal fixation, femur nailing, femur plating.
Fractures of the femur shaft are frequently encountered in the field of orthopedics. Fractures of this nature are commonly caused by high-intensity trauma, such as the impact of missiles or vehicular accidents [1,2]. The femur receives a plentiful blood flow from both the endosteal and periosteal sources. Nutrient arteries typically penetrate the body through the linea aspera of the femur, entering from both the posterior and proximal directions [3]. The inner three-quarters of the cortex receive its blood supply from the endosteal vasculature, while the periosteal vasculature exclusively supplies blood to the outermost quarter of the bone. The periosteal circulation is essential for the healing process of diaphyseal fractures [4]. In a displaced fracture, the blood arteries located in the middle of the bone are harmed, and the blood vessels on the outer surface of the bone take over as the primary source of blood supply to the fracture site during the early healing phase. To ensure proper healing, it is crucial to minimize the removal of periosteum, especially along the linea aspera, during surgical procedures, as it might negatively impact periosteal blood flow [4,5]. At present, femur nailing, with bone entry through the piriformis fossa, is universally recognized as the most effective approach for managing fractures in the midshaft of the femur [6]. Open reduction and internal fixation with plating of acute femur shaft fractures is used only in a limited number of cases due to the high number of complications associated [7]. This study aims to evaluate whether combining intramedullary nailing with derotation plating provides improved rotational stability and fracture healing in femoral shaft fractures where nailing alone may be insufficient.
A prospective observational study was undertaken at Krishna Hospital from February 2022 to July 2024, encompassing a cohort of 30 patients diagnosed with femoral shaft fractures. The sample size of 30 patients was determined based on a convenience sampling method due to the limited availability of eligible patients within the study period. There were a total of 30 individuals, consisting of 25 males and 5females. The age range was from 20 to 45 years. Road traffic incidents were the main factor contributing to the fracture in most instances. Affecting 27 patients, whereas 3 patients experienced fractures due to falls on the ground. There were ten people who had additional injuries, including both damage to their bones and ailments that did not involve their bones.
Criteria for inclusion
- The femur is fractured, specifically in the middle and lower portions of the bone.
- Individuals between the ages of 18 and 45
- Patients who do not have any impairments in the nerves or blood vessels in the extremities.
Criteria for exclusion
- Fractures of the femur that involves many bone fragments.
- Patients with polytrauma
- Patients experiencing distal neurovascular impairment
- Individuals diagnosed with segmental femur fractures
- Patients with preexisting abnormalities in the fractured limb
- Individuals who have had previous surgery for femur fracture.
- Patients diagnosed with pre-existing osteomalacia, a condition characterized by weakened bones.
The surgery was carried out within a time window of 3–11 days after the accident. The patient had surgery in the lateral decubitus position while under spinal anesthetic on a normal operating table. The posterolateral approach was used. A minuscule quantity of periosteum is excised on both sides of the fracture. No dissection was carried out near the linea aspera. A small quantity of reaming is conducted on the medullary canal, utilizing manual reamers. The femur nail is inserted using interlocking techniques. A dynamic compression plate is affixed to either the side or front of the femur. The average length for finishing the surgery varied between 90 and 120 min.
The investigation revealed that new comminuted fractures were a particularly prevalent kind of fracture reported, accounting for 18 patients (60%).
All 30 patients had successful fracture union. On X-ray examination, a well-defined callus was noted in operated patients within a timeframe of 3–6 months following the surgical procedure.
The post-operative assessment revealed an alignment with <5° of varus/valgus, 5° of internal rotation, 10° of external rotation, <5° of antecurvatum, and <1 cm of shortening. No cases of infection were observed among the patients. The present investigation did not document any occurrences of plate avulsion or loosening. This study did not find any notable difference in limb length (Tables 1 and 2).
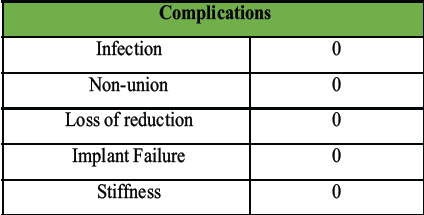 Table 1: Showing post-operative complications
Table 1: Showing post-operative complications
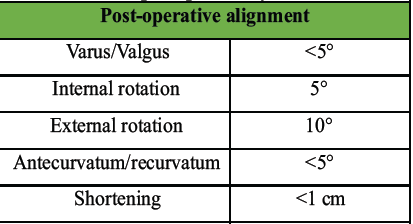 Table 2: Showing alignment of femur postoperatively
Table 2: Showing alignment of femur postoperatively
None of the patients experienced post-operative knee or hip stiffness after undergoing combination fixation with an intramedullary nail and derotation plate. X-rays of the patient with follow-ups at 3 months and 6 months(Fig. 1, 2, 3, 4).
 Figure 1: Showing pre-operative X-rays.
Figure 1: Showing pre-operative X-rays.
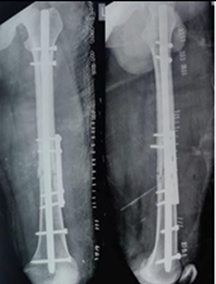 Figure 2: Showing immediate post-operative X-rays.
Figure 2: Showing immediate post-operative X-rays.
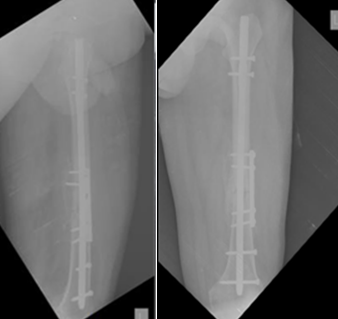 Figure 3: POD 3-month X-rays.
Figure 3: POD 3-month X-rays.
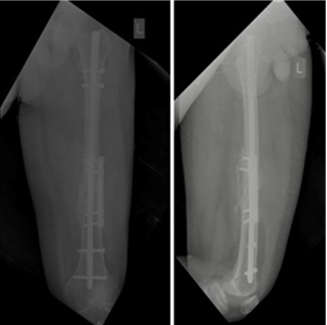 Figure 4: POD 6-month X-rays.
Figure 4: POD 6-month X-rays.
At present, surgery is the most optimal approach to treating shaft femur fractures since it has a high success rate in bone healing, minimal incidence of complications, and the capability to promptly stabilize the fracture. This early stabilization helps decrease the occurrence of illness and mortality in patients. The selection of treatment options for all patients should be ascertained. By a comprehensive assessment of the patient’s health status upon arrival, the level of urgency for the required treatment, the availability of materials, and the surgeon’s specific expertise. Different types and techniques of surgical fixation were utilized.
Thorensen et al. [8] performed a method that involved placing nails in 48 patients. The average discrepancy in them was smaller than 10°. Our analysis revealed that the average malalignment among a sample of 30 patients was smaller than 5°.
Apivatthakakul and Chiewcharntanakit [9] performed plating procedures on a total of 34 patients. The average varus/valgus incorrect alignment in the individuals was smaller than 10°. The mean varus/valgus incorrect alignment in our patients who underwent femur nailing with derotation plating decreased below 5°.
Broos and Reynders [10] conducted an experiment where they placed fifty individuals and measured the range of flexion, which ranged from 0 to 90°. Out of our sample of thirty patients, the maximum range of motion varied from 0 to 120°.
Ricci et al. [11] performed a retrospective analysis of 104 diaphyseal femur fractures that underwent medical intervention retrograde intramedullary nailing, comparing them to 94 fractures that were treated with antegrade intramedullary nailing. Each group had a unionization rate of 6%. The incidence of nonunion varies dramatically with traditional plate fixation. Böstman and Rokkanen [12] observed a nonunion rate of 5% in their patients, but Seligson et al. [13] documented a significantly higher nonunion rate of 46.7% in their study. The study discovered a non-union rate of 0%, which aligns with the findings of previous investigations that employed a single fixation approach.
Research on femoral fractures has demonstrated that interlocking nailing is associated with a decreased infection rate of <1%, in contrast to a higher rate of 7% for deep-seated infections when traditional plate and screws are utilized 16. The study found that the infection rate was 0% after using a combination fixation strategy; this finding aligns with prior research that exclusively employed a single fixation approach.
The study did not document any occurrences of failure of the implant or loose of the derotation plate. In contrast to prior studies that exclusively utilized traditional plate and screws for the treatment of diaphyseal femoral fractures, which revealed implant failure rates in the range of 3.5–12% (including plate loosening, avulsion, or breaking), our approach differs. We suggest that by integrating both intramedullary nails and plate augmentation techniques, the benefits of both treatments for stabilizing fractures can be obtained, while simultaneously reducing their potential drawbacks and disadvantages. The femur nail functions as a load-sharing device. Derotation plate fixation is a successful method for managing excessive movement at the fracture site, guaranteeing rigidity, and preventing any loss of reduction. By employing shorter derotation plates, the surgical method becomes considerably less invasive compared to the traditional plate technique. This method successfully circumvents the disadvantages linked to traditional plating, such as extended surgical duration, extensive hemorrhaging. When doing this combined fixation, it is crucial to highlight multiple factors. The present concern is whether the simultaneous utilization of femur nail and a reinforcement plate will potentially impede the blood circulation to the fractured femur. Paying meticulous attention to precise technical aspects is necessary for minimizing harm to the blood veins that provide blood to the femur during this surgical technique. It is imperative to handle the tissue with utmost caution, refraining from any superfluous trauma.
A composite implant design, consisting of a combination of nailing and derotation plate, is a practical and rational choice for stabilizing Fractures of the femoral diaphysis. It can be considered a viable substitute for interlocking nail fixation. Compared to the utilization of either conventional plating and screws or a solitary nail, this procedure offers a more reliable and steady fixing, hence decreasing the likelihood of reduction loss. Moreover, this approach encounters less issues. The attained stiffness is crucial for allowing prompt weight bearing and helping the recovery of patients with complex fractures.
Combined fixation using intramedullary femur nailing with a derotation plate provides enhanced stability and reliability in managing comminuted femoral shaft fractures. This technique leverages the load-sharing benefits of nailing and the rotational control of plating, promoting early weight bearing, consistent fracture alignment, and a lower risk of complications. It serves as a viable and effective alternative to conventional interlocking nailing or plating alone in femoral shaft fractures.
References
- 1. Fakhry SM, Rutledge R, Dahners LE, Kessler D. Occurrence, treatment, and results of femoral shaft fractures in a rural area. J Trauma 1994;37:255-60. [Google Scholar] [PubMed]
- 2. Luedtke LM, Flynn JM, Ganley TJ, Hosalkar HS, Pill SG, Dormans JP. A perspective from the orthopedist: Conditions such as bone tumors, scoliosis, and trauma. Radiol Clin North Am 2001;39:803-21. [Google Scholar] [PubMed]
- 3. Ashcroft GP, Evans NT, Roeda D, Dodd M, Mallard JR, Porter RW. Utilizing positron emission tomography (PET) to measure blood flow in patients with tibial fractures. J Bone Joint Surg Br 1992;75:673-7. [Google Scholar] [PubMed]
- 4. Momberger N, Stevens P, Smith J, Santora S, Scott S, Anderson J. Use of intramedullary nailing for femoral fractures in teenagers. J Pediatr Orthop 2000;20:482-4. [Google Scholar] [PubMed]
- 5. Alonso J, Geissler W, Hughes JL. External fixation for femoral fractures: Indications and constraints. Clin Orthop 1989;241:83-8. [Google Scholar] [PubMed]
- 6. Starr AJ, Bucholz RW, Heckman JD. Femoral shaft fractures. In: Rockwood CA, Bucholz RW, Heckman JD, Rockwood DP, editors. Rockwood and Green’s Fractures in Adults. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001. [Google Scholar] [PubMed]
- 7. Smrke D, Princic J. The use of plates and screws for fixing femoral shaft fractures: Analysis of complications. Unfallchirurg 2000;103:110-4. [Google Scholar] [PubMed]
- 8. Thorensen BO, Alho A, Ekeland A, Strømsøe K, Follerås G, Haukebø A. Interlocking intramedullary nailing in femoral shaft fractures. J Bone Joint Surg 1985;67A:1313-20. [Google Scholar] [PubMed]
- 9. Apivatthakakul T, Chiewcharntanakit S. Minimally invasive plate osteosynthesis (MIPO) in the treatment of the femoral shaft fracture where intramedullary nailing is not indicated. Int Orthop 2009;33:1119-26. [Google Scholar] [PubMed]
- 10. Broos PL, Reynders P. The use of the unreamed AO femoral intramedullary nail with spiral blade in nonpathologic fractures of the femur: experiences with eighty consecutive cases. J Orthop Trauma 2002;16:150-4. [Google Scholar] [PubMed]
- 11. Ricci WM, Bolhofner BR, Loftus T, Cox C, Mitchell S, Borrelli J Jr. Indirect reduction and plate fixation, without grafting, for periprosthetic femoral shaft fractures about a stable intramedullary implant. J Bone Joint Surg Am 2005;87:2240-5. [Google Scholar] [PubMed]
- 12. Böstman O, Rokkanen P. The management of diaphyseal fractures of the long bones in Finland: A nation-wide survey. Ann Chir Gynaecol 1986;75:333-6. [Google Scholar] [PubMed]
- 13. Seligson D, Mulier T, Keirsbilck S, Been J. Plating of femoral shaft fractures. A review of 15 cases. Acta Orthop Belg 2001;67:24-31. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report
February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report February 1, 2026 Medial Epicondyle Fractures Treated with Diverse Fixation Techniques: A Case Series
February 1, 2026 Medial Epicondyle Fractures Treated with Diverse Fixation Techniques: A Case Series December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis
December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System