
This case highlights the rare possibility of non-traumatic peroneal tendon subluxation caused by distal fibular osteochondroma. Both can be addressed by a single surgical approach with an excellent outcome.
Dr. Jagatheesan Dharmarajan, Institute of Foot and Ankle Surgery, Parvarthy Ortho Hospital, Chromepet, Chennai, Tamil Nadu, India. E-mail: dharmarajdr1223@gmail.com
Introduction: The most prevalent benign bone tumor is osteochondroma. It typically manifests around the knee, most frequently in the distal femur, proximal tibia, and proximal fibula. Clinical characteristics vary depending on the site and pressure effects on neighboring structures. The existence of both non-traumatic peroneal tendon subluxation and distal fibula osteochondroma is uncommon. By contributing to the limited literature on distal fibula osteochondroma resulting in peroneal tendon subluxation, this case offers valuable insights into the condition’s clinical manifestation, diagnosis, and treatment. Apart from this case, only one case has been described in the literature.
Case Report: We present a case report of an unusual presentation of distal fibula osteochondroma associated with peroneal tendon subluxation in a 37-year-old male patient with no history of trauma. He presented with pain over the lateral gutter and painful instability of the peroneal tendons in his left ankle. He underwent osteochondroma excision with peroneal groove deepening. Complete resolution of pain and instability was noted in the 1-year follow-up.
Conclusion: The necessity of using osteochondroma as a differential diagnosis for ankle swellings and peroneal tendon subluxation without trauma is highlighted by this case. Distal fibula osteochondroma is rarely the etiology of these conditions. The successful management and follow-up of this patient illustrate the potential for favorable outcomes with appropriate treatment. This case report provides valuable information to the literature, enhancing our understanding of the clinical presentation and management of rare distal fibula osteochondroma causing peroneal tendon subluxation.
Keywords: Osteochondroma, peroneal tendon subluxation or dislocation, exostosis, benign bone tumor, ankle swelling.
Osteochondroma is a non-cancerous growth of cartilage and bone. It is the most common kind of benign bone tumor. An abnormal subperiosteal germ of the fertile cartilage gives rise to this skeletal hamartoma, which mostly grows throughout the skeletal growth period and matures in accordance with normal endochondral ossification [1]. Depending on the structure involved, osteochondromas can be an accidental discovery or manifest as a palpable lump or symptoms brought on by compression of the nearby structures [2]. We present a case of osteochondroma of the left distal fibula with peroneal tendons subluxation.
A 37-year-old male presented at our clinic with a history of pain over the lateral side of the left ankle for 3 months. He had no history of trauma. Physical examination revealed a mild prominence arising from the posterolateral aspect of the distal fibula, and there was demonstrable peroneal tendon instability on ankle movements (Fig 1). Ankle anteroposterior and lateral radiographs showed multiple small calcified lesions near the lateral malleolus (Fig 2).

Figure 1: Clinical photograph showing peroneal subluxation anteriorly.
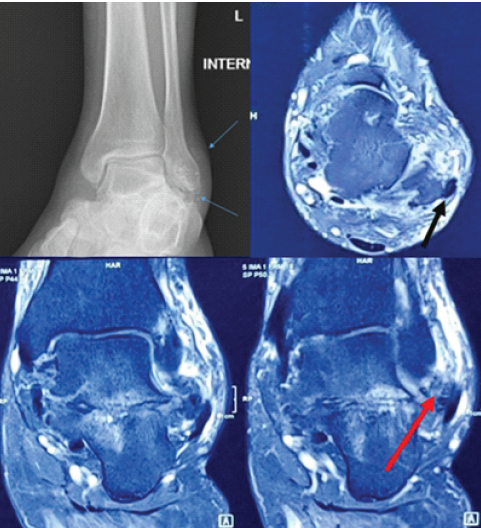
Figure 2: X-ray showing distal fibula lesion. Magnetic resonance imaging shows the osteochondroma (red arrow) and peroneal subluxation (black arrow).
Magnetic resonance imaging revealed peroneal tendon subluxation anteriorly and a bony lesion present in the distal fibula and the lateral aspect of the calcaneum. We proceeded with surgery to explore the bony mass and peroneal tendons. Surgery was performed in the theater. The patient was given intravenous antibiotics, and surgery was carried out under a thigh tourniquet at 300 mmHg. A lateral incision was made over the distal fibula, we found subluxed peroneal tendons with absent superior peroneal retinaculum (SPR) and peroneal groove (Fig. 3). We also uncovered an osteochondroma of size 2.5 × 2.5 × 2 cm at the distal end of fibula and another bony exostosis of size 1.5 × 1.5 × 1.5 from lateral aspect of calcaneum (Fig. 3).

Figure 3: Intraoperative photograph showing the peroneal tendon subluxation and osteochondroma.
We thoroughly excised the lesion and created the peroneal groove using punch and mallet and tendons were stabilized in the groove. Reassessed stability and found the ankle joint and peroneal tendons were stable without any subluxation. Postoperatively, a below-knee plaster was applied, and the patient’s leg was put in a non-weight-bearing cast for 6 weeks. Full weight bearing permitted at 10 weeks. Histology confirmed osteochondroma with no malignant change. American Orthopedic Foot and Ankle Score (AOFAS) hind-foot score was collected clinically before operation, which was scored at (~65), including pain 20, function 35; however, alignment was 10. The post-operation showed significantly improved morbidity, including pain (30) and functional activities (50); there was no change to the alignment (10), which sets a higher score of 80. The wound healed well, and there was no recurrence of exostosis and peroneal tendon subluxation after 1 year of follow-up (Fig. 4).
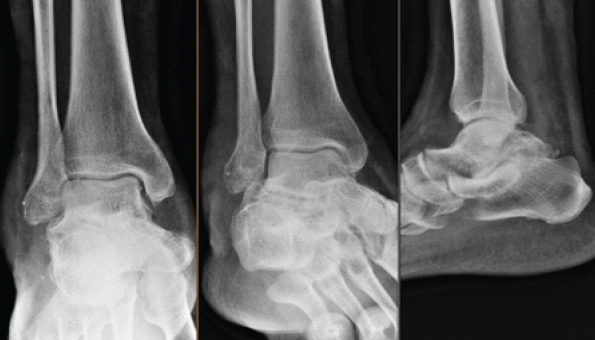
Figure 4: 1-year follow-up radiograph.
Osteochondroma, also known as exostosis, is the most common benign bone tumor, comprising approximately 10% to 15% of all bone tumors. These tumors primarily present in the growing skeleton, often before the age of 20 years, and are frequently located at the distal femur, proximal tibia, and proximal fibula [2,3]. However, the occurrence of osteochondromas in the distal fibula is relatively rare, making this case report particularly noteworthy. Osteochondromas can be asymptomatic or present with symptoms depending on the location and their relationship with surrounding structures. In many cases, patients may remain unaware of the osteochondroma until incidental imaging reveals the lesion, especially if it does not impinge on critical structures. When symptoms are present, they are often related to the mechanical effects of the tumor, such as local pain, swelling, or restriction of movement due to compression or impingement on adjacent tendons, nerves, or joints [4]. In this case, the patient exhibited pain and instability around the lateral aspect of the left ankle due to peroneal tendon subluxation, a complication rarely associated with osteochondromas. The relationship between osteochondromas and peroneal tendon subluxation is uncommon. Peroneal tendon dislocation was first described by Monteggia in 1803 and is typically attributed to trauma, such as sudden dorsiflexion and eversion of the foot, often seen in sports injuries [5]. However, in the case presented here, no trauma was reported, which is consistent with the rare occurrence of atraumatic peroneal tendon subluxation caused by an osteochondroma. This suggests that the growth of the osteochondroma may have created mechanical instability in the peroneal tendons, exacerbating their tendency to subluxate, especially due to the lack of the SPR and an underdeveloped peroneal groove. In a study by Saglik et al., only six of 382 patients with osteochondromas had tumors located on the fibula (1.6%), and all of these lesions arose in the proximal fibula [6]. This highlights the rarity of osteochondromas arising from the distal fibula. Furthermore, Perisano et al. observed in their review of distal fibular tumors that these lesions were exceedingly rare and most patients had excellent outcomes after surgical excision, which is consistent with the positive outcome observed in our patient [7]. The clinical importance of this case lies in the recognition that distal fibula osteochondromas can cause atypical presentations, such as peroneal tendon subluxation, even in the absence of trauma. Peroneal tendon subluxation, which is a well-known cause of lateral ankle pain, typically arises from a traumatic event where the tendons slip out of place in the peroneal groove. However, when an osteochondroma causes anatomical changes or impingement around the lateral malleolus, it can contribute to such instability, as was seen in our patient. Regarding the management, the treatment approach for peroneal tendon dislocation due to an osteochondroma generally involves a combination of osteochondroma excision and stabilization of the peroneal tendons. Several surgical techniques, including peroneal groove deepening, SPR reconstruction, and tendon rerouting, are employed depending on the extent of the tendon instability [8,9]. In our case, we performed a groove-deepening procedure and re-stabilized the tendons, resulting in successful resolution of symptoms and prevention of further dislocation. This outcome is consistent with the literature, where surgical excision of the osteochondroma and peroneal tendon stabilization leads to good functional recovery [10,11]. It is also important to note the potential for malignant transformation in osteochondromas, although this is extremely rare. Malignant change is more commonly associated with hereditary multiple exostoses rather than solitary osteochondromas [12]. However, in the present case, histology confirmed that the osteochondroma was benign with no signs of malignancy.
Distal fibula osteochondroma and atraumatic peroneal tendon subluxation are both rare. This case management elaborates on the re-stabilized tendons through groove-dependent procedure benefits, with the resolution of symptoms and prevention of dislocation of the peroneal tendon. Surgical management consists of osteochondroma resection with peroneal tendon stabilization procedures. Timely intervention results in excellent outcomes using the AOFAS hind-foot score.
This case report emphasizes the rare occurrence of distal fibula osteochondroma causing peroneal tendon subluxation. This report gives awareness that atraumatic peroneal subluxation with or without swelling around the ankle should be evaluated for bony growths. The surgical step well defines where the groove was created to stabilize the peroneal tendon through it, which gives mechanical stability in the peroneal tendons. This report provides valuable insights into the clinical presentation, imaging characteristics, and management strategies for distal fibula osteochondroma causing peroneal tendon subluxation.
References
- 1. Campanacci M, Bertoni F, Bacchini P, editors. Solitary exostosis: Synonyms: Osteocartilaginous exostosis, osteochondroma. In: Bone and Soft Tissue Tumors. Berlin: Springer; 1990. [Google Scholar] [PubMed]
- 2. Bottner F, Rodl R, Kordish I, Winklemann W, Gosheger G, Lindner N. Surgical treatment of symptomatic osteochondroma. A three- to eight-year follow-up study. J Bone Joint Surg Br 2003;85:1161-5. [Google Scholar] [PubMed]
- 3. Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46. [Google Scholar] [PubMed]
- 4. Florez B, Monckeberg J, Castillo G, Beguiristain J. Solitary osteochondroma long-term follow-up. J Pediatr Orthop B 2008;17:91-4. [Google Scholar] [PubMed]
- 5. Espinosa N, Maurer MA. Peroneal tendon dislocation. Eur J Trauma Emerg Surg 2015;41:631-7. [Google Scholar] [PubMed]
- 6. Saglik Y, Altay M, Unal VS, Basarir K, Yildiz Y. Manifestations and management of osteochondromas: A retrospective analysis of 382 patients. Acta Orthop Belg 2006;72:748-55. [Google Scholar] [PubMed]
- 7. Perisano C, Marzetti E, Spinelli MS, Graci C, Fabbriciani C, Maffulli N, et al. Clinical management and surgical treatment of distal fibular tumours: A case series and review of the literature. Int Orthop 2012;36:1907-13. [Google Scholar] [PubMed]
- 8. Heckman DS, Reddy S, Pedowitz D, Wapner KL, Parekh SG. Operative treatment for peroneal tendon disorders: Review. J Bone Joint Surg Am 2008;90:404-18. [Google Scholar] [PubMed]
- 9. Wang CC, Wang SJ, Lien SB, Lin LC. A new peroneal tendon rerouting method to treat recurrent dislocation of peroneal tendons. Am J Sports Med 2009;37:552-7. [Google Scholar] [PubMed]
- 10. Shazadeh Safavi K, Ratnasingam S, Janney CF. Chronic peroneal tendon dislocation: A case report. Mil Med 2020;185:e1882-6. [Google Scholar] [PubMed]
- 11. Klos K, Vag T, Gras F, König V, Hofmann GO, Mückley T. Distal peroneal tendon dislocation: A case report. Foot Ankle Int 2011;32:314-8. [Google Scholar] [PubMed]
- 12. Bovée JV. Multiple osteochondromas. Orphanet J Rare Dis 2008;3:3. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report
February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling
October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling January 1, 2025 Solitary Osteochondroma in Uncommon Sites- A Rare Case Report
January 1, 2025 Solitary Osteochondroma in Uncommon Sites- A Rare Case Report December 1, 2024 Challenges and Solutions in Managing Recurrent Distal Tibia Interosseous Osteochondroma: A Case Study and Review of Literature
December 1, 2024 Challenges and Solutions in Managing Recurrent Distal Tibia Interosseous Osteochondroma: A Case Study and Review of Literature