
Superior acetabular fractures are rare variants that require CT-based assessment and tailored surgical approaches.
Dr. Hunaid Haider, Department of Orthopaedics, Seth G.S. Medical College and KEM Hospital, Mumbai, Maharashtra, India. Email: hzhad98@gmail.com
Introduction: Superior acetabular fractures are extremely rare and poorly covered by existing classifications.
Case Report: A 52-year-old male presented 2½ weeks after a road traffic accident with a superior acetabular fracture involving the roof, iliac wing, and both walls. He was treated through an iliofemoral approach with ASIS osteotomy, reduction using a Schanz pin, and fixation with two cannulated screws. At 6 months, he showed excellent function (Merle d’Aubigné score 17).
Conclusion: Superior acetabular fractures are rare variants requiring computed tomography-based assessment. The iliofemoral approach provides good exposure and favorable outcomes.
Keywords: Acetabular fracture, superior fracture, iliofemoral approach, computed tomography, fracture classification.
Acetabulum fractures, classified by Letournel and Judet [1,2], are renowned for their reproducibility Beaulé et al. [3] and pivotal role in surgical decision-making Laude et al., [4]; Matta, [5]. Upper fractures, a rarity in this classification, were notably absent in 403 cases per Duquennoy and Senegas [6], and only 2 cases were documented among 940 by Letournel and Judet [2]. These fractures, which detach the acetabular roof and part of the anterior iliac wing from the posterior wall, challenge traditional categorization as posterosuperior fractures Letournel and Judet, [2]. This unique observation underscores the surgical complexities posed by such infrequently described acetabular fractures.
Mr. S., aged 52, was found lying beside the road in an inebriated manner, and was referred from multiple centres, leading to a 2½ week delay in treatment. X-rays showed a superior type fracture of the right acetabulum (Fig. 1).,
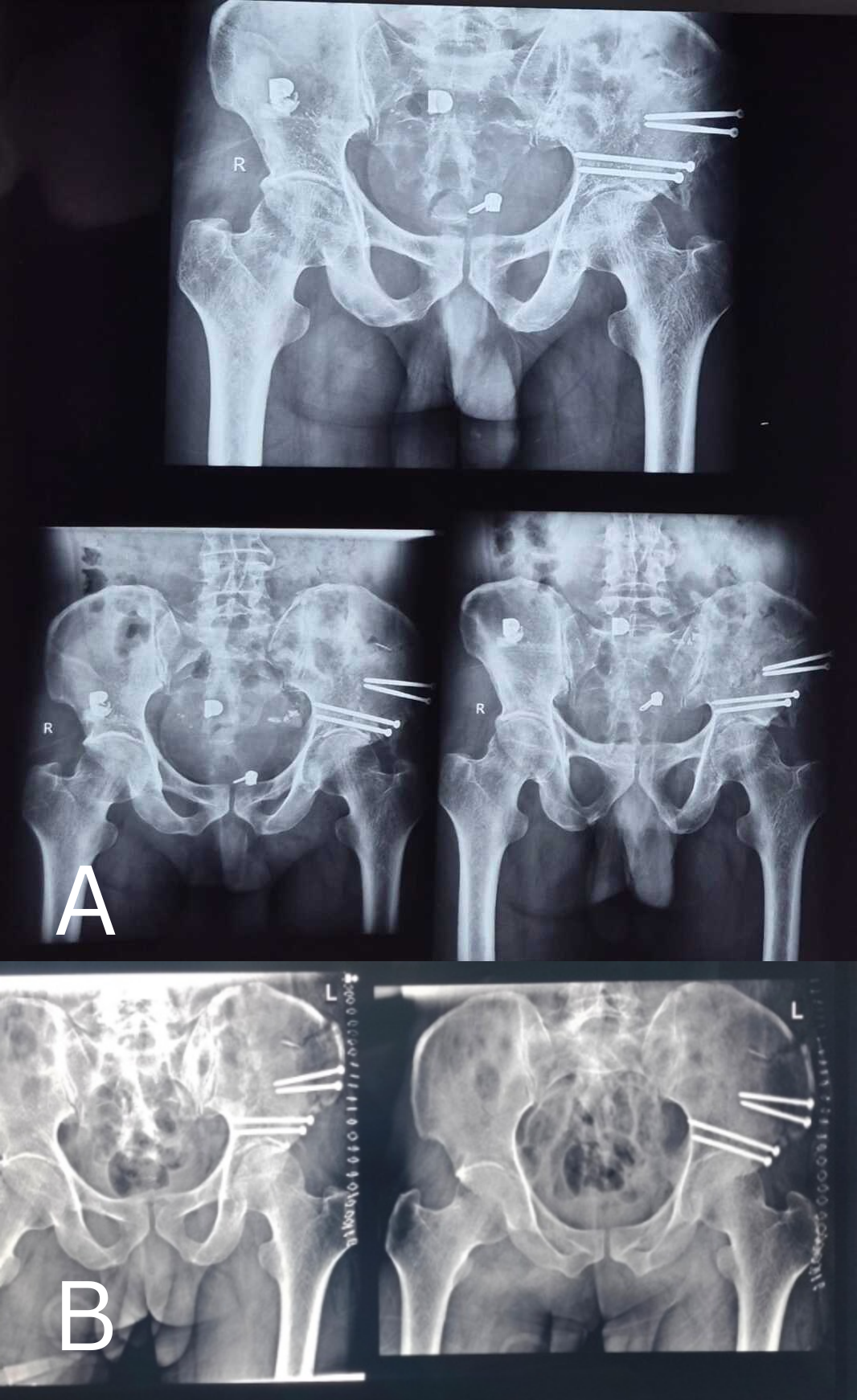
Figure 1: (a) Three months post-operative X-ray of the pelvis (b) Immediate post-operative X-ray of the pelvis.
according to Letournel and Judet [2], detaching the acetabular roof and the adjoining part of the iliac wing while respecting the continuity of the pelvic ring (Fig. 2).
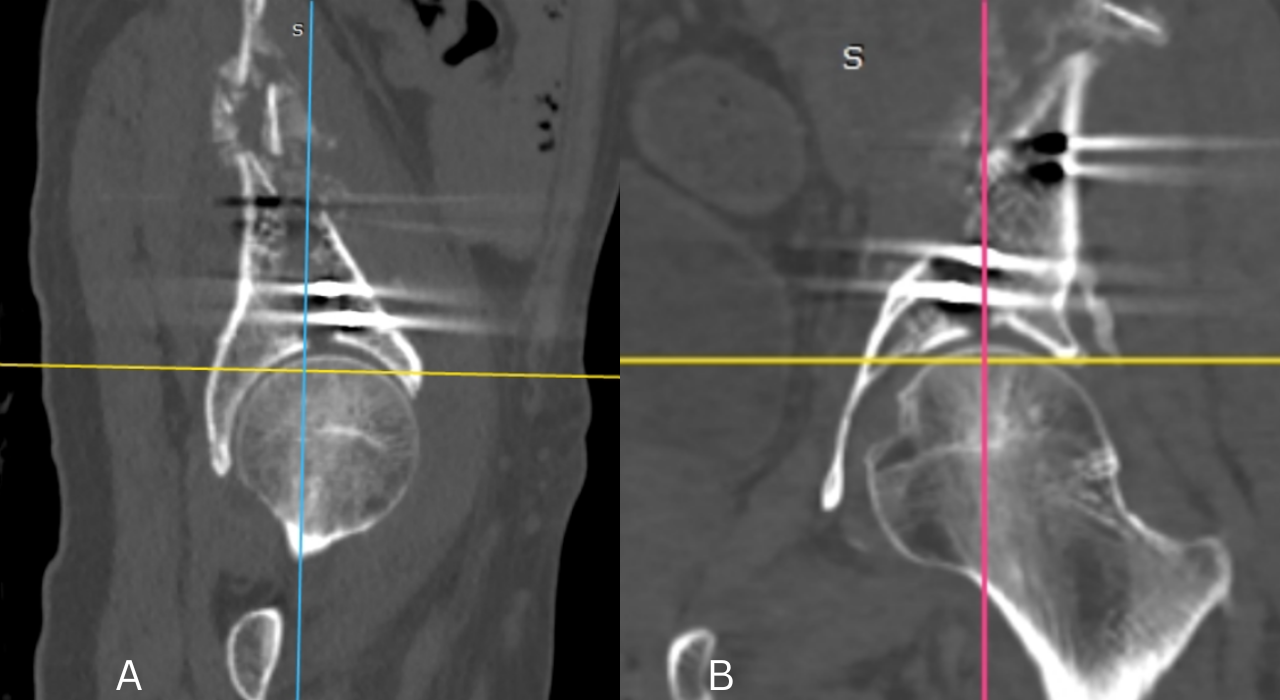
Figure 2: Post-operative computed tomography scan of fracture (a) Sagittal view (b) Coronal view.
Besides this elementary displaced lesion, it was observed that the anterior, posterior and medial wall was part of the line (Fig. 3) with it being continuous with the voluminous upper fragment.
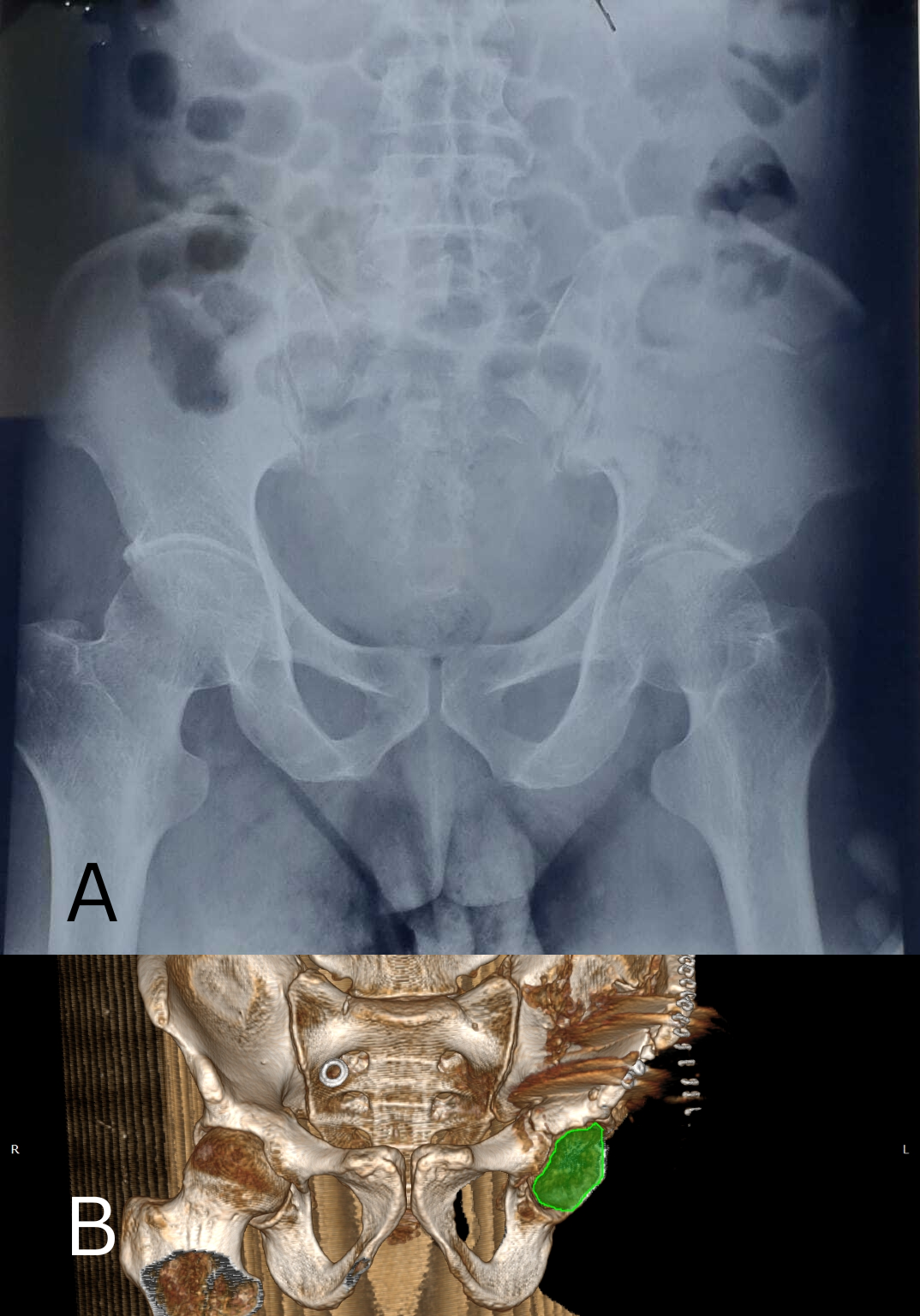
Figure 3: (a) Pre-operative antero-posterior X-ray of the acetabulum showing a superior type fracture of the right acetabulum (b) post operative 3D reconstruction of the pelvis showing superior fracture while respecting continuity of the pelvic ring.
Computed tomography (CT) showed separation of the anterior wall of the cranial fragment by a slightly displaced split line (Fig. 4 and 5).
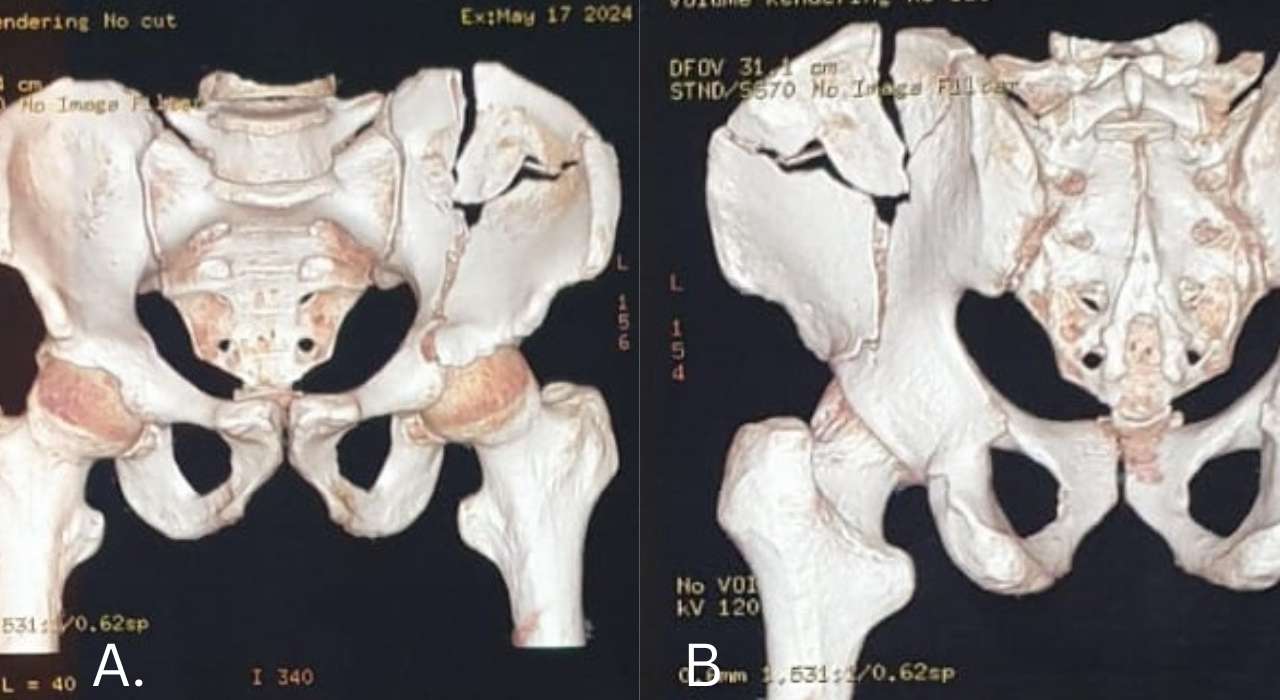
Figure 4: 3D model reconstruction of superior acetabular fracture (a) Anterior view (b) Posterior view.
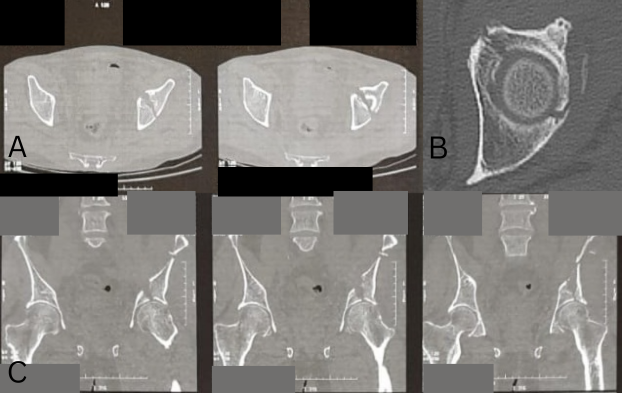
Figure 5: Pre-operative computed tomography scan (a) Sagittal view (b) Axial view (c) Coronal view.
In addition, the patient had an non-displaced C1 fracture, which was not associated with any neurodeficit and was conserved. To better control the reduction of all the features, particularly of the anterior wall, an enlarged iliofemoral approach according to Judet and Letournel [1] was performed with partial elevation of the iliacus. Anterior superior iliac spine osteotomy was done for better visualisation of the anterior column and wall and for garnering adequate angulation for osteosynthesis. The callus at the fracture line extending intraarticularly was removed, and reduction was achieved via pressure over the iliac blade and attachment of a Schanz pin to the iliac crest to use in a joystick manner. Osteosynthesis using two 4.5 mm fully threaded cannulated screws was performed with iliac blade fixation (Fig. 1). In the post-operative course, hip mobilization was started as soon as the pain subsided and continued at the patient’s residence. No ossification prophylaxis was performed apart from abundant washing of the wound with isotonic serum throughout the procedure. At 6 months after the trauma, the Merle d’Aubigné functional score was, a reliable predictor of hip function, [7] was 17.
Superior fractures of the acetabulum are exceptionally rare and pose a unique challenge in classification within the Letournel and Judet’s framework, which traditionally categorizes fractures into five elementary and five complex types [1,2]. These fractures do not neatly fit into these defined categories, constituting a distinct entity due to their specific anatomical characteristics. Letournel and Judet identified a subgroup among posterior acetabular fractures known as postero-superior fractures, which anatomically detach the upper sector of the acetabulum, including the roof, while typically leaving the lower part of the posterior wall intact [2]. They described cases where extension of the fracture line to the upper sector of the acetabulum was present, detached along with the anterior part of the iliac wing, yet respecting the innominate line [2]. This classification highlights the unique detachment pattern of these fractures compared to fractures of the posterior wall [2]. These fractures, involving detachment of the roof and variable engagement of the posterior wall, are akin to a variant of the pure upper fractures reported by Letournel and Judet [2]. The AO classification (Tile classification), which generally categorizes them as type A1 due to posterior wall involvement, does not fully capture the nuanced detachment of the upper acetabulum [8]. Letournel and Judet’s classification offers a more precise description, facilitating accurate clinical depiction and reproducibility in therapeutic decision-making, particularly in choosing the optimal surgical approach [3,4]. For fractures involving the upper acetabulum while respecting the posterior wall, an ilioinguinal approach is typically recommended to preserve muscle integrity [2]. However, in cases where the posterior wall is extensively detached, as observed, a dual approach or iliofemoral approach may be necessary for comprehensive fracture reduction and stable fixation [9]. In the clinical scenario presented, despite initial concerns about potential complications such as ectopic ossification associated with the iliofemoral approach, this surgical method was selected to ensure precise reduction and facilitate early post-operative recovery without notable adverse effects [10,11]. While the iliofemoral approach has drawn criticism for its potential overexposure and associated risks, it proved effective in achieving optimal reduction and enabling swift rehabilitation [12]. A similar fracture was described by Berton et al, but with only a posterior wall extension without an anterior wall involvement [13].
Superior acetabulum fractures present challenges in both classification and surgical management, underscoring the importance of a classification system that accurately reflects their anatomical complexity for improved treatment planning and patient outcomes.
Superior acetabular fractures are rare and easily missed in standard classifications. Pre-operative CT defines the fracture, and a tailored iliofemoral approach enables precise reduction and favorable functional recovery.
References
- 1. Letournel E, Judet R, editors. Fractures of the Acetabulum. 2nd ed. Berlin: Springer-Verlag; 1993. p. 740 [Google Scholar] [PubMed]
- 2. Letournel E, Judet R. Fractures of the Acetabulum. Berlin: Springer-Verlag; 1993. [Google Scholar] [PubMed]
- 3. Beaule PE, Dorey FJ, Matta JM. Letournel classification for acetabular fractures. Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 2003;85:1704-9. [Google Scholar] [PubMed]
- 4. Laude F, Puget J, Martimbeau C. Fractures du cotyle. In: Encyclopedia Médico-Chirurgicale. Appareillocomoteur. Vol. 14. Paris: Elsevier; 1999. p. 73. [Google Scholar] [PubMed]
- 5. Matta JM. Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 1996;78:1632-45. [Google Scholar] [PubMed]
- 6. Duquennoy A, Senegas J, Angereau B, Copin G, Delcour JP, Durandeau A, et al. Acetabular fractures: Results after more than 5 years. Revue de Chirurgie Orthopédique et Réparatrice de l’Appareil Moteur. 1982;68:45–82. [Google Scholar] [PubMed]
- 7. Ugino FK, Righetti CM, Alves DP, Guimarães RP, Honda EK, Ono NK. Evaluation of the reliability of the modified Merle d’Aubigné and Postel Method. Acta Ortop Bras 2012;20:213-7. [Google Scholar] [PubMed]
- 8. Tile M. Fractures of the Pelvis and Acetabulum. 2nd ed. Baltimore: Williams and Wilkins; 1995. [Google Scholar] [PubMed]
- 9. Jouffroy P. Lesional diagnosis of acetabular fractures. In: SOFCOT Teaching Lectures. Vol. 78. 2001. p. 97–122. [Google Scholar] [PubMed]
- 10. De Peretti F, Schlatterer B, Cambas PM, Argenson C. The iliofemoral approach of Letournel in acetabular fractures involving both columns: A prospective study. Revue de Chirurgie Orthopédique et Traumatologique. 1994;80:476. [Google Scholar] [PubMed]
- 11. Griffin DB, Beaule PE, Matta JM. Safety and efficacy of the extended iliofemoral approach in the treatment of complex fractures of the acetabulum. J Bone Joint Surg Br 2005;87:1391-6. [Google Scholar] [PubMed]
- 12. Glas PY, Fessy MH, Carret JP, Bejui JH. Surgical treatment of acetabular fractures: Results of a continuous series of 60 cases. Revue de Chirurgie Orthopédique. 2001;87:529–38. [Google Scholar] [PubMed]
- 13. Berton C, Bachour F, Migaud H, Pinoit Y, Laffargue P: Nouvelle variété de fracture postéro-supérieure de l’acétabulum: Stratégie thérapeutique à propos d’un cas [A new type of acetabular fracture: “True” posterosuperior fracture, a case report]. Rev Chir Orthop Reparatrice Appar Mot 2007;93:93-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Navigation-Assisted Percutaneous Fixation of an Anterior Column and Posterior Hemitransverse Fracture in an Elderly Patient: A Case Report
March 1, 2026 Navigation-Assisted Percutaneous Fixation of an Anterior Column and Posterior Hemitransverse Fracture in an Elderly Patient: A Case Report March 1, 2026 A Case Report on Unclassified Anatomical Sciatic Nerve Variant in Acetabulum Fracture
March 1, 2026 A Case Report on Unclassified Anatomical Sciatic Nerve Variant in Acetabulum Fracture February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report
February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review
January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review