
Dorsal scapular osteochondromas with lateral and ventral extension are rare and should be considered in scapular swellings, with surgery reserved for clear indications and outcomes best assessed using Patient-Reported Outcome Measures to strengthen clinical research in benign bone tumors.
Dr. V S Sri Hari Ram, Lokmanya Tilak Municipal Medical College, Mumbai, Maharashtra, India. E-mail: 1997srihari@gmail.com
Introduction: Osteochondromas are the most common benign bone tumors, typically arising from the metaphyseal regions of long bones. However, their occurrence in flat bones, particularly the scapula, is rare. We report a case of a large solitary osteochondroma arising from the dorsal aspect of the scapula in a pediatric patient, which was successfully treated with surgical excision.
Case Report: A 12-year-old female presented with a progressively enlarging bony swelling over the right scapular region since the age of 7 years, recently associated with difficulty in lying over the affected side. Radiological evaluation, including X-ray and computed tomography scan confirmed a large osteochondroma arising from the inferior angle of the right scapula. This case is unique as the osteochondroma extends from dorsal to ventral aspect through the lateral aspect of scapula making it difficult for the child to lie on both supine and right lateral positions. The patient underwent en bloc excision, resulting in complete resolution of symptoms and had no recurrence at follow-up.
Conclusion: Though uncommon, osteochondroma should be considered in the differential diagnosis of bony swellings over flat bones, such as the scapula. Earlier surgical management may yield the best functional and cosmetic outcomes.
Keywords: Osteochondroma, scapula, bony swelling, pediatric bone tumor, surgical excision.
Osteochondroma or osteocartilaginous exostosis, accounts for approximately 35–50% of benign bone tumors. While commonly found in long bones, such as the femur, tibia, and humerus, involvement of flat bones – especially the scapula – is uncommon, accounting for only 3–4.6% of all osteochondroma cases. Among scapular tumors, osteochondromas account for 14.4%, with the ventral surface being the more common site of occurrence [1,2]. We present a rare case of a large, solitary osteochondroma arising from the dorsal surface of inferior angle of scapula, which was successfully treated with complete surgical excision.
A 12-year-old female presented to our orthopedic clinic with complaints of a large, hard swelling over the right scapular region and difficulty in lying on the affected side. The swelling was noted since the age of 7 years and gradually increased in size over the years, becoming symptomatic in the past year with difficulty in lying on the affected side.
On physical examination, a lobulated, bony‑hard, and non‑tender mass measuring approximately 15 × 6 × 6 cm was palpated over the inferior angle of the right scapula, extending from the posterior aspect forward toward the thoracic wall; the overlying skin was freely mobile and there were no signs of inflammation or neurovascular compromise (Figs. 1 and 2). An incidental finding of multiple swellings around bilateral knee joints was made.

Figure 1: Preoperative clinical photograph from the back showing a large lobulated swelling over the dorsal aspect of the right scapula, causing visible posterior asymmetry and pseudowinging.

Figure 2: Pre-operative clinical photograph from the right side revealing extension of mass from the posterior to the anterior aspect.
Plain radiographs and computed tomography (CT) of the right scapula revealed a large, pedunculated exostosis arising from the dorsal aspect of the scapula (Fig. 3). Multiple pedunculated bony lesions from the bilateral distal femur and proximal tibia were noted. Surgical excision of the scapular mass was elected, while the knee lesions were left under observation since there were no clinical complaints.
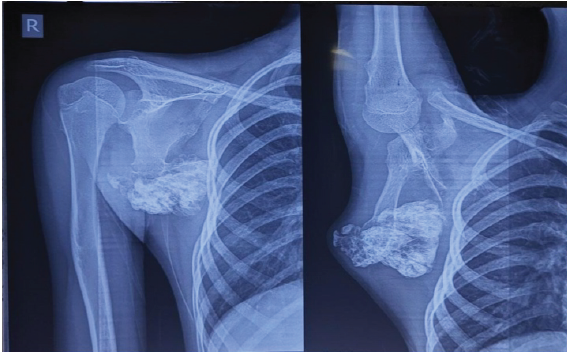
Figure 3: Preoperative shoulder radiograph (antero-posterior and scapular Y views) showing a large, well-circumscribed, pedunculated bony mass arising from the inferior angle of the right scapula.
Under general anesthesia with the patient prone, a straight incision was made along the lateral border of the right scapula; the 15 × 6 × 6 cm, lobulated, bony mass was noted which was delivered en bloc (Fig. 4). The tumor was lobulated with a cartilage cap, and continuity between the medullary canal of the lesion and the native scapula confirmed the diagnosis of osteochondroma. Intraoperative clinical picture and fluoroscopy ensured complete resection. Post op X-ray confirmed the same.
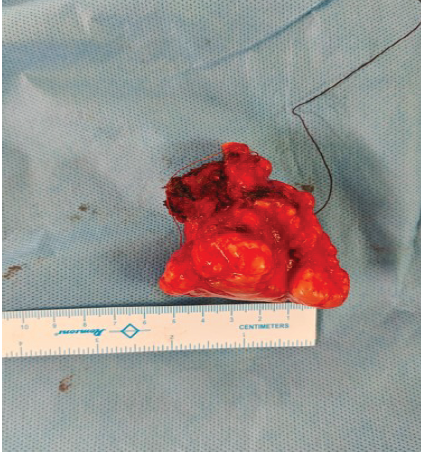
Figure 4: Gross image of the excised tumor with multilobulated surface and cartilaginous cap, placed next to a scale for reference (approx. 6 cm).
Histopathological examination confirmed benign osteochondroma. Post-operatively, the patient had significant improvement in shoulder mobility, with complete wound healing and no recurrence on follow-up examination and imaging(Figs. 5 and 6).

Figure 5: 1-year clinical follow-up image from behind showing no signs of clinical recurrence with healed scar.

Figure 6: 1-year follow-up antero-posterior X-ray showing no recurrence of the lesion.
Osteochondromas are benign osteocartilaginous exostoses that originate when epiphyseal (growth‑plate) cartilage herniates through the periosteal sleeve and ossifies – separating from the parent bone cortex and medulla – yet remain usually asymptomatic and are detected incidentally on radiographs or CT scans [3,4]. Flat bone involvement is uncommon, and dorsal scapular osteochondromas are even rarer compared to the ventral side. Scapular osteochondroma on superomedial angles are also reported and are excised by superior approach to scapula [5]. Classification is based on the morphology of the base, defined as either pedunculated (with a stalk, growing away from the epiphysis) or sessile (broad based) [6]. Osteochondroma on the dorsal aspect are usually reported Sessile [7]. In rare sites, such as the scapula, however, they may produce symptoms, such as pain, cosmetic prominence, or mechanical issues, such as snapping or restricted scapulothoracic motion [8].
Signs most concerning for malignant transformation include new onset pain, rapid growth especially after skeletal maturity, anatomical site-scapula or pelvis, and a cartilage cap thickness >2 cm. In skeletally immature bone, during spurts of growth, the cartilage cap may become quite large, and necessarily does not indicate a malignant transformation [7]. They may mimic other pathologies, such as lipomas, soft tissue tumors, or bony deformities [9,10]. In our case, the size and location of the tumor resulted in functional limitation, warranting surgical intervention.
Delayed diagnosis can lead to complications, such as pseudo-winging, snapping scapula, bursa formation, or nerve compression [11,12,13,14]. Surgical excision provides excellent results, as seen in our patient [15].Physiotherapy rehabilitation should be given to improve quality of life [16].
Massive solitary osteochondroma of the dorsal scapula is a rare clinical entity, but should be considered in the differential diagnosis of longstanding scapular swellings. Early imaging, prompt diagnosis, and surgical excision can prevent complications and restore function, especially in pediatric patients.
Osteochondroma, although typically seen in long bones, can present atypically in flat bones, such as the scapula. Large lesions can cause functional impairment and should be surgically addressed for symptomatic relief and prevention of complications.
References
- 1. Kwon OS, Kelly JI. Delayed presentation of osteochondroma on the ventral surface of the scapula. Int J Shoulder Surg 2012;6:61-3. [Google Scholar] [PubMed]
- 2. Oliveira MA, Alfaro Y, Kotzias Neto A, Korman MC. Subscapular osteochondroma as a differential diagnosis of winged scapula. Rev Bras Ortop (Sao Paulo) 2019;54:241-6. [Google Scholar] [PubMed]
- 3. Ngongang FO, Fodjeu G, Fon AC, Fonkoue L, Guifo ML, Bitang A Mafok LJ, et al. Surgical treatment of rare case of scapula osteochondroma in a resource limited setting: A case report. Int J Surg Case Rep 2019;61:130-4. [Google Scholar] [PubMed]
- 4. Chun DI, Cho JH, Choi IH, Yi Y, Kim JY, Kim JH, et al. Osteochondroma of ventral scapula associated with chest pain due to rib cage compression: A case report. Medicine (Baltimore) 2018;97:e0510. [Google Scholar] [PubMed]
- 5. Shafer DH, Robles EL, Linsley CM, Lamb AN. Osteochondroma of the superomedial scapula managed with a novel muscle sparing approach: Case report and review of literature. J Surg Case Rep 2024;2024:rjae154 [Google Scholar] [PubMed]
- 6. Shreyas BL, Joshi S, Burhani AA, Jadon SP, Athul M, Yadav BR. Osteochondroma of the scapula: A rare case report. Int J Orthop Sci 2024;10:420-6. [Google Scholar] [PubMed]
- 7. Das R, Arya S, Krishna A, Ghosh S, Mukartihal R, Keezhadath S. Osteochondroma of dorsal scapula: A case report and review of literature. J Orthop Case Rep 2023;13:104-9. [Google Scholar] [PubMed]
- 8. Mozaffarian K, Farahani MJ, Vosoughi AR. Bilateral sandwiched scapulae: A rare presentation of hereditary multiple exostoses. J Clin Orthop Trauma 2016;7:5-7. [Google Scholar] [PubMed]
- 9. Nekkanti S, Moogali A, Meka A, Nair M. An unusual presentation of osteochondroma on the dorsal surface of the scapula: A review of two patients. J Orthop Case Rep 2018;8:38-41. [Google Scholar] [PubMed]
- 10. Bektas YE, Ozmanevra R. An unusual location of osteochondroma: Dorsal scapula. Cureus 2019;11:e6464. [Google Scholar] [PubMed]
- 11. Jadhav PU, Banshelkikar SN, Seth BA, Goregaonkar AB. Osteochondromas at unusual sites – case series with review of literature. J Orthop Case Rep 2016;6:52-4. [Google Scholar] [PubMed]
- 12. Ratra R, Peshin C. Rare presentation of benign osteochondroma: A case report. J Orthop Case Rep 2020;9:82-5. [Google Scholar] [PubMed]
- 13. Beauchamp-Chalifour P, Pelet S. Osteochondroma of the scapula with accessory nerve (XI) compression. Case Rep Orthop 2018;2018:7018109. [Google Scholar] [PubMed]
- 14. Chillemi C, Franceschini V, Ippolito G, Pasquali R, Diotallevi R, Petrozza V, et al. Osteochondroma as a cause of scapular winging in an adolescent: A case report and review of the literature. J Med Case Rep 2013;7:220. [Google Scholar] [PubMed]
- 15. Altwaijri NA, Fakeeha J, Alshugair I. Osteochondroma of the scapula: A case report and literature review. Cureus 2022;14:e30558. [Google Scholar] [PubMed]
- 16. Thakare V, Phansopkar P, Chitale N. Physiotherapy rehabilitation in subject with scapular osteochondroma: A case report. J Pharm Res Int 2021;33:160-4. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review
August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review October 10, 2023 Unveiling Scapular Pseudo-winging: A Case Report on Ventral Osteochondroma of the Scapula in a 21-year-old
October 10, 2023 Unveiling Scapular Pseudo-winging: A Case Report on Ventral Osteochondroma of the Scapula in a 21-year-old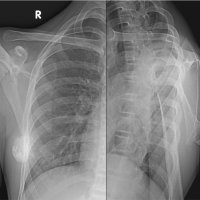 July 10, 2023 Osteochondroma of Dorsal Scapula: A Case Report and Review of Literature
July 10, 2023 Osteochondroma of Dorsal Scapula: A Case Report and Review of Literature