
In radial club hands, due to the lack of a standard treatment protocol, based on the established principles of reconstructive surgery and the surgical techniques described by different authors, a tailored approach has to be adopted as per the severity of the case, to restore the form and function, even with a minimalistic wedge osteotomy alone.
Dr. Mainak Mallik, Department of Burns and Plastic Surgery, All India Institute of Medical Sciences, Kalyani, West Bengal, India. (Former Associate Professor, Department of Burns and Plastic Surgery, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India). 550/4, P.K. Guha Road, Radhanagar, P.O. Dumdum, Kolkata - 700028, West Bengal, India. E-mail: mognomainak@gmail.com
Introduction: Radial club hand is a rare congenital condition (1 in 100,000) involving varying deformities on the radial side of the forearm, ranging from thumb underdevelopment to absence of the radius and related structures. It can be isolated or part of syndromes, such as thrombocytopenia-absent radius, Holt-Oram, or vertebral, anal, cardiac, tracheo-esophageal, renal, limb, and is bilateral in 50–72% of cases.
Case Report: A 12-year-old right-handed girl presented with an isolated, non-syndromic right radial club hand and flexion deformity at the wrist and elbow, without functional impairment. Her pathology did not fit existing Bayne and Klug or Heikel classifications, as her proximal radius was absent but the distal epiphysis and wrist were developed. A corrective wedge osteotomy with bilobed skin flaps was performed to realign the forearm. No intervention was made at the wrist or musculotendinous units, resulting in an acceptable outcome.
Conclusion: Reasonable outcome could be obtained in a rare case of complex congenital anomaly like radial club hand following a minimalist approach of wedge osteotomy alone to correct the forearm deformity.
Keywords: Radial club hand, osteotomy, bilobed flap, case report.
Radial club hand is a rare congenital anomaly (1 in 100,000 births) involving varying degrees of radial-side forearm malformations, from thumb hypoplasia to complete absence of the radius and first ray, often accompanied by underdevelopment of adjacent muscles, tendons, ligaments, nerves, and vessels. It may occur in isolation or in association with syndromes, such as thrombocytopenia-absent radius, Holt-Oram, and vertebral, anal, cardiac, tracheo-esophageal, renal, limb. The condition is bilateral in 50–72% of cases and linked to disruptions in sonic hedgehog gene pathways that influence the apical ectodermal ridge, essential for limb development [1]. The earliest known report is credited to Jean-Louis Petit in 1733 [2]. Treatment strategies vary, ranging from conservative observation to surgical procedures aimed at centralizing the carpus over the ulna, often combined with corrective casting [3,4].
A 12-year-old girl (right hand dominant) presented with a congenital right upper limb isolated non-syndromic radial club hand (unclassified as per Heikel’s or Bayne and Klug classifications). Her main complaint was flexion deformity of the right upper limb at the wrist and elbow joint levels without any functional deficit of the hand. X-ray shows the presence of distal radial epiphysis with a radially deviated integral wrist joint (maintained radio-carpal, ulno-carpal and distal radio-ulnar joints), absence of diaphysis and proximal radius, and shortened ulna with a radial bent (Fig. 1).
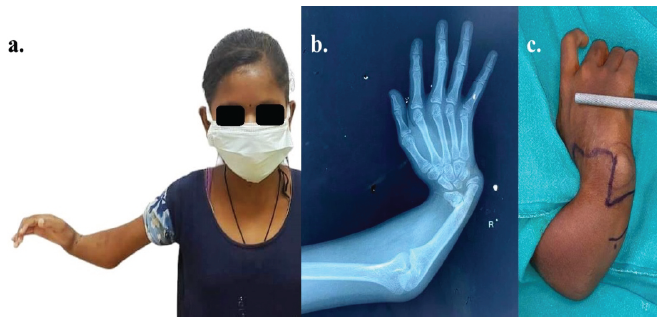
Figure 1: Pre-operative pictures (a) the affected right upper limb deformity; (b) skiagram showing the same; (c) pre-operative markings.
The distal shaft of the ulna was approached with a bilobed (transposition flap) incision and following exposure of distal ulna at the subperiosteal level, corrective osteotomy was done as per planning and marking of osteotomy after measuring from the skiagram with calculation of angular deviation to precisely plan the osteotomy triangle (Figs. 2 and 3).
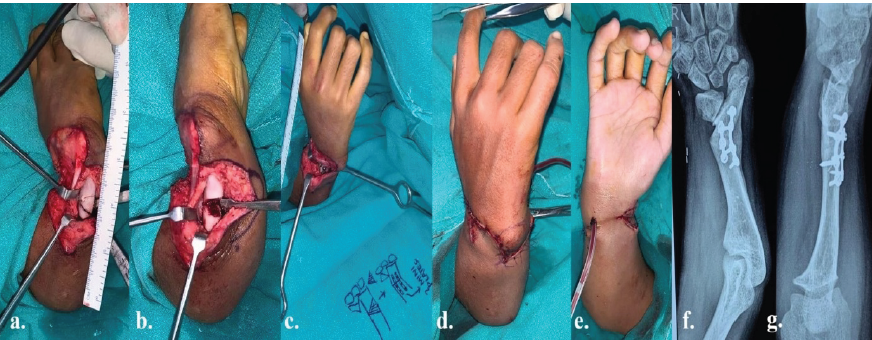
Figure 2: Intraoperative pictures- (a) marking of osteotomy after exposure of distal forearm bone; (b) wedge osteotomy done; (c) fixation with 2 miniplates- 4-holed with gap and 3-holed with gap; (d and e) skin closure with bilobed flaps- dorsal and volar views; (f and g) skiagram to check the position after correction.
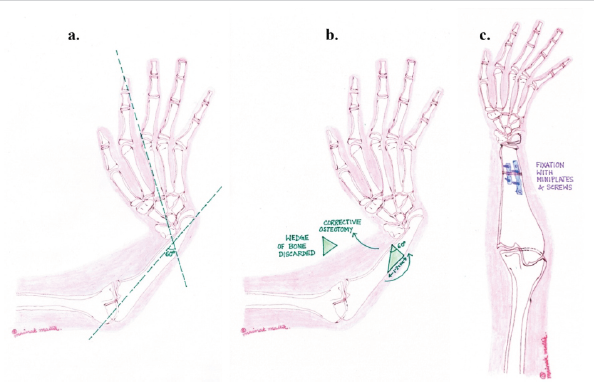
Figure 3: Planning of the osteotomies with measurement from skiagrams- (a and b) calculation of angular deviation and planning the osteotomy triangle; (c) diagrams after fixation with miniplates and screws.
Following osteotomy, the segments of ulna were approximated to the desired corrected position to achieve the straightening and fixed with two mini plates in a parallel manner (one 4 holed with gap and another 3 holed with gap). Fixation was done only on the dorsal aspect, and the volar aspect was not disturbed to avoid deterioration of flexor function. Heavy implants were avoided looking at the inadequate bone volume and also to get rid of any deleterious effect of them in future skeletal development. Intraoperatively, it was challenging to achieve the goals of the surgical procedure (to achieve adequate straightening, good stability of osteotomized bone segments, and preservation of soft tissue elements), aiming for an optimum functional hand. The skin was closed by radial transposition of the bilobed fasciocutaneous flaps. Plaster of Paris cast was applied with the limb in functional position of 30° wrist extension, 90° metacarpophalangeal joints extension and inter-phalangeal joints extension for 3 weeks post-operatively (Fig. 2 and Video 1).
On follow-up visits subsequently, the sutures were removed after 2 weeks and the forearm deformity was corrected with preservation of all hand functions and wrist movements as she had pre-operatively (Fig. 4 and Video 2). The patient was followed up for 3 months after surgery. The functional outcome was not assessed using any objective scoring system. However, she was observed to retain all the hand functions as she had before surgery (Video 2).
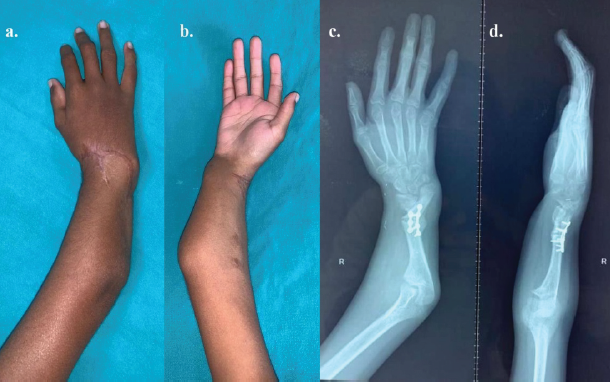
Figure 4: (a and b) 3-month post-operative views of the right upper limb dorsal and volar aspects; (c and d) skiagrams (anteroposterior and lateral views) on follow-up.
The management of radial club hand has evolved from purely corrective procedures to staged, multidisciplinary approaches aimed at maximizing both function and cosmesis. Gradual soft tissue distraction using external fixators, followed by centralization of the carpus over the distal ulna, remains a widely accepted strategy for severe deformities [5]. This method reduces tension on neurovascular structures and improves alignment before definitive reconstruction. Centralization and osteotomy are key surgical options for managing radial club hand, each suited to different deformity severities. According to Saini et al., gradual distraction followed by centralization effectively corrects severe radial deviation and soft-tissue contracture, improving wrist alignment and stability. Khan et al. emphasize an algorithmic approach, reserving centralization for advanced deformities and osteotomy for milder structural realignment. Olson and Hosseinzadeh note that osteotomy preserves growth and function with fewer complications. Takagi et al. conclude that while centralization achieves greater correction, osteotomy provides safer and more stable long-term results in mild cases [5,6,7,8].
Surgical timing is crucial, with early intervention (typically before 2 years of age) offering better outcomes in terms of alignment and growth modulation [6]. For acquired cases or late presentations, individualized algorithms based on residual bone, joint stability, and function guide decision-making [6]. In congenital cases, the choice between centralization, radialization, or ulnarization is based on severity, presence of functional musculature, and long-term growth potential [7,8,9,10]. Despite advances, recurrence of radial deviation remains a challenge, highlighting the need for long-term follow-up and, in some cases, secondary procedures [8].
As per literature, most radial club defects encompass the defects starting at the distal ends of radius (as proximodistal limb development occurs), which mandate reconstruction of the distal wrist joint in the form of centralization of the carpus on the distal end of ulna with a varying amount of rudimentary radius present from the proximal end at the proximal radio-ulnar joint. The two main classifications used to describe radial club hand are Heikel (1959) and Bayne and Klug (1987). Based on the degree of radial aplasia or hypoplasia, Heikel’s classification divided the deformity into four grades: Grade I exhibits slight radius shortening, Grade II has distal radius hypoplasia, Grade III shows partial aplasia, and Grade IV denotes complete absence of the radius. Building on this idea, Bayne and Klug offered a four-type classification based on radiography, with Type I representing a short distal radius, Type II representing a hypoplastic radius, Type III representing partial absence, and Type IV being the most severe form – complete absence of the radius [3,4].
However, in this case, the procedure is not a generalized one as the anatomy did not fit to any described varieties of radial club hand deformity. The distal radial epiphysis, radio-carpal, and distal radio-ulnar joints were present, with absent radial diaphysis and proximal part in the entirety. As the carrying angle of the elbow joint was satisfactory, no intervention was planned at the elbow joint level in such restricted flexion deformity of the elbow. Only the radial deviation of the wrist joint and abnormal radial bending of the ulna (60° radial to the central axis) was corrected with a corrective osteotomy, leaving the functional wrist joint intact. Early and late post-operative results showed uncomplicated wound outcomes and the forearm axis to be centrally oriented with healed osteotomy sites as per the skiagram of the wrist joint. Hence, we conclude that surgical management of radial club hands is curtailed to the specific pathology due to developmental anomaly. A minimal surgical intervention to address the main issue, produces the optimum outcome and benefit.
As it is a report of a single case, ethical approval was not obtained, although informed consent obtained from the parents of the child for the use of the case details, with the photographs and videos for publication and educational purposes.
The radial club hand deformity in this particular patient was an exceptional variation and does not fit to the classifications used in contemporary clinical practice. Surgical technique was tailored and curtailed to address to the need for correction of pathological anatomy. Although this is an observation of a solitary case, it may be concluded that a satisfactory outcome can be expected with minimal surgical intervention, provided the basic reconstructive principles are followed meticulously. However, the technique needs to be applied for the surgical correction of similar deformities in more cases and by different hand surgeons in multiple centres to increase the feasibility and acceptability.
Even if no standard technique is described in literature for a specific clinical condition, surgical treatment can be tailored, based on basic standard reconstructive principles, to restore form and function.
References
- 1. Towers M, Tickle C. Sonic hedgehog regulates digit number by controlling the balance of Gli3 repressor and activator. Dev Cell 2004;6:349-57. [Google Scholar] [PubMed]
- 2. Flatt AE. The Care of Congenital Hand Anomalies. United States: Quality Medical Publishing; 1994. [Google Scholar] [PubMed]
- 3. Bayne LG, Klug MS. Long-term review of the surgical treatment of radial deficiencies. J Hand Surg Am 1987;12:169-79. [Google Scholar] [PubMed]
- 4. Heikel HV. Aplasia and hypoplasa of the radius: Studies on 64 cases and on epiphyseal transplantation in rabbits with the imitated defect. Acta Orthop Scand Suppl 1959;39:1-155. [Google Scholar] [PubMed]
- 5. Saini N, Patni P, Gupta S, Chaudhary L, Sharma V. Management of radial clubhand with gradual distraction followed by centralization. Indian J Orthop 2009;43:292-300. [Google Scholar] [PubMed]
- 6. Khan H, Ul Ain N, Afridi K, Bhatti Z, Chishti U, Malik TS, et al. Acquired radial club hand: An algorithm to manage radial deficiency. Cureus 2023;15:e43154. [Google Scholar] [PubMed]
- 7. Olson N, Hosseinzadeh S. Radial dysplasia. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar] [PubMed]
- 8. Takagi T, Seki A, Takayama S, Watanabe M. Current concepts in radial club hand. Open Orthop J 2017;11:369-77. [Google Scholar] [PubMed]
- 9. Avdeychik NV, Golyana SI, Safonov AV, Grankin DY, Zakharyan EA. Lengthening of radius in patients with congenital radial club hand, type II. Pediatr Traumatol Orthop Reconstr Surg 2019;7:15-24. [Google Scholar] [PubMed]
- 10. Matsuno T, Ishida O, Sunagawa T, Suzuki O, Ikuta Y, Ochi M. Radius lengthening for the treatment of Bayne and Klug type II and type III radial longitudinal deficiency. J Hand Surg Am 2006;31:822-9. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review
February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report February 1, 2026 A Novel Technique of Rerouting Semitendinosus Graft for Medial Collateral Ligament and Medial Patellofemoral Ligament Reconstruction – In a Polytrauma Patient with Multiligament Injury: Kakran et al. Technique
February 1, 2026 A Novel Technique of Rerouting Semitendinosus Graft for Medial Collateral Ligament and Medial Patellofemoral Ligament Reconstruction – In a Polytrauma Patient with Multiligament Injury: Kakran et al. Technique January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report
January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report