
Proximal tibial stress fractures are a rare but significant complication following tibial tuberosity osteotomy. Prevention relies on precise surgical technique, gradual rehabilitation, and early identification of symptoms, while surgical fixation remains a reliable treatment when fractures arise.
Dr. Anton Maliarov, Bnai Zion Hospital, Haifa, Israel. E-mail: dr.antonmaliarov@gmail.com
Introduction: Tibial tubercle osteotomy (TTO) is an appropriate surgical procedure for patellar instability and chronic patellofemoral pain; however, complications such as proximal tibial fracture occur in 1–1.8% of cases.
Case Report: A 19-year-old non-professional dancer underwent TTO with medialization for patellofemoral pain. Postoperatively, rehabilitation followed a structured protocol. At 3 months, radiographs revealed an onset of stress fracture below the TTO site, progressing and involving two-thirds of the tibial diameter on the last follow-up. Surgical fixation with a lateral tibial locking plate was performed to prevent propagation. Ten months after plating, the fracture had fully consolidated, while a Knee Injury and Osteoarthritis Outcome score was 90.5, and the hardware was removed without complications.
Conclusion: Proximal tibial stress fractures post-TTO are rare but require early recognition and intervention. This case highlights the caution required in rehabilitation and the necessity of surgical intervention as a viable treatment to ensure proper fracture healing and successful recovery.
Keywords: Tibial tubercle osteotomy, patellofemoral pain syndrome, proximal tibial stress fracture, surgical complications of the knee.
Chronic patellar pain syndrome, lateral patellar instability, and localized patellofemoral osteoarthritis are widely recognized indications for tibial tubercle osteotomy (TTO) [1]. Several surgical options exist for addressing patellar instability and/or patellofemoral pain and osteoarthritis. These include soft-tissue procedures such as medial patellofemoral ligament reconstruction or repair, lateral patellar release, and various femoral and tibial osteotomies [2]. While these techniques are generally effective for most patients, complications may arise in 4–8% of cases [3].
Initially, the procedure outlined by Elmslie–Trillat involves medial displacement of the tibial tuberosity (TT) to realign the knee extensor mechanism [4]. However, other types of TT transfer, such as distalization, anteriorization (Maquet’s technique), and anteromedialization (Fulkerson’s technique), are also documented and can be applied [5].
Proximal tibial fractures are uncommon and usually arise intraoperatively or within 8–14 weeks postoperatively [6].
This article details a unique case of a stress proximal tibial fracture that was initiated 3 months after TTO for chronic patellofemoral pain syndrome. In addition, we analyze the factors contributing to this fracture to enhance our surgical technique and improve future post-operative rehabilitation protocols.
An athletic 19-year-old non-professional dancer experienced worsening pain primarily in her left knee during physical activities. She underwent surgery for an unstable and painful patella, involving a TTO along with medialization. Her pre-operative Knee Injury and Osteoarthritis Outcome Score (KOOS) was 72. The TT–trochlear groove (TG) distance was measured to 20 mm, and the Caton–Deschamps index was calculated as 1.24, and the patellar tilt measured 18°, with clinically excessive tightness, and the hip-knee angle was aligned at 177°. A combined open and arthroscopic approach was applied.
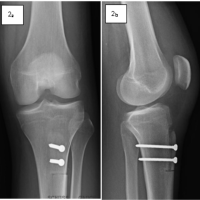
During the arthroscopic portion of the surgery in May 2023, a grade 1 chondral lesion on the lateral patellar facet was identified according to the Outerbridge classification, and lateral retinacular release was performed. During the second part, the tibial tuberosity (TT) was medialized by 1 cm and secured with two 4.5 mm lag screws, achieving a TT-TG distance up to 10 mm in the final measurement (Fig. 1).

Figure 1: (a) Anteroposterior and (b) lateral view of the left tibia immediately after tibial tuberosity osteotomy fixed with 4.5 screws.
Post-operative care was straightforward, with a weight-bearing restricted protocol for 6 weeks. A removable knee extension splint was adjusted by gradually increasing the range of motion by an additional 30° every 2 weeks.
Throughout the 6 weeks, the knee’s range of motion was progressively restored, with flexion not exceeding 90°. Isotonic knee-locking exercises were postponed for 6 weeks, while isometric contractions were encouraged. During a 3-month follow-up outpatient visit, X-rays confirmed the spontaneous onset of a stress fracture of the proximal tibia below the TTO site, showing signs of progression on the next follow-up (Fig. 2). The patient was advised to limit sports activities and postpone dancing. However, the 10-month follow-up evaluation revealed a significant progression of the fracture line, involving two-thirds of the entire tibial diameter, leaving just the posterior cortex intact (Fig. 3).

Figure 2: The lateral view demonstrates signs of a stress fracture along the lower margin of the osteotomy level, observed during the 3-month follow-up evaluation.
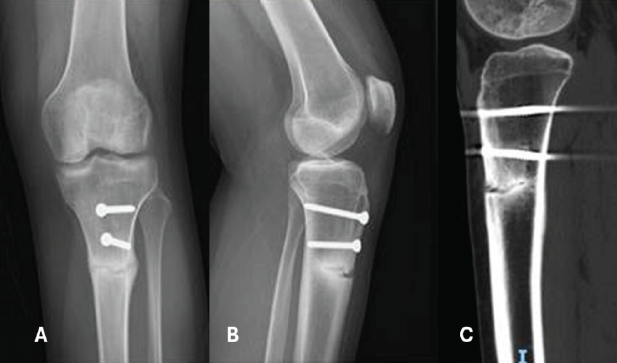
Figure 3: Anteroposterior view (a), lateral view (b), and sagittal computed tomography image (c) demonstrate the critical progression of the fracture line, involving two-thirds of the entire tibial diameter.
Fastly, a lateral tibial pre-modulated locking plate was applied to prevent further fracture propagation and avoid prolonged cast immobilization (Fig. 4). The same unlocked knee extension brace was recommended, along with a full weight-bearing protocol. Ten months after the plating procedure, the proximal tibial stress fracture had consolidated, with the KOOS score evaluated at 90.5 at that time (Fig. 5). Later, the patient underwent the removal of all hardware successfully (Fig. 6).
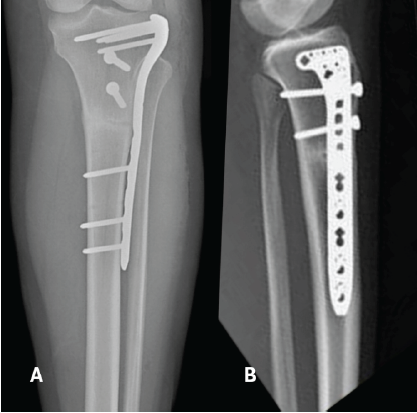
Figure 4: Anteroposterior view (a), lateral view (b) demonstrate the immediate post-surgical view of fracture fixation with lateral tibial pre-modulated locking plate.
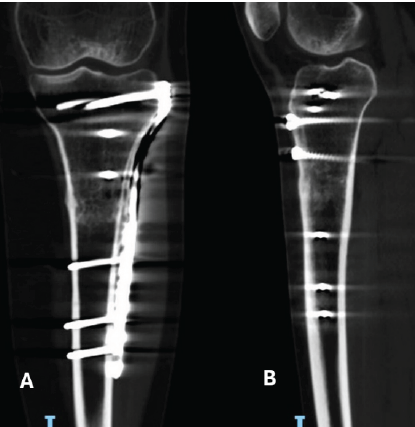
Figure 5: Coronal view (a) and sagittal view (b) computed tomography images demonstrate good consolidation of the fracture site.
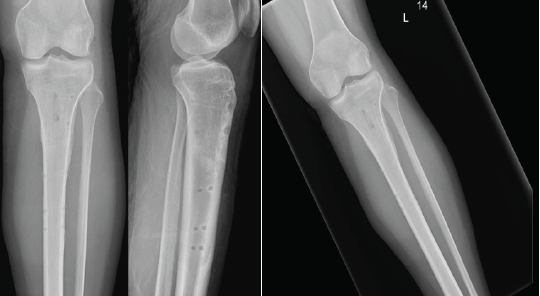
Figure 6: Anteroposterior view (a) and lateral view (b) demonstrate the post-removal tibia, showing a well-healed fracture site.
Dependence of fracture occurrence on the type of osteotomy
Proximal tibial fractures occurring after TTO are observed in approximately 1–1.8% of cases [3,7, ]. The risk of fracture appearance depends on the osteotomy direction, the necessity of distalization of the bone fragment [6], and the post-operative weight-bearing protocol [8].
A cadaveric study conducted by Cosgarea et al. revealed that mechanical stresses associated with a Fulkerson technique osteotomy tend to result in proximal tibial fractures more frequently, whereas those resulting from a flat osteotomy, such as the Elmslie–Trillat technique, are more likely to lead to fractures of the tuberosity [9].
In our case, the flat osteotomy, as described by Fulkerson, was performed. Interestingly, the signs of fracture progression began just after 3–4 months and progressed toward the medial and lateral cortex, with signs of obvious callus formation, matching stress fracture characteristics.
Healing of osteotomy
Healing at the osteotomy site can be affected by host factors (patient age, concomitant medical problems, and previous surgery) and surgical issues (osteotomy depth, fixation type, and post-operative rehabilitation). In a series of 153 cases, Johnson et al. reported that the rate of delayed union, defined as incomplete healing based on radiographic criteria at 90 days, was notably higher in cases involving TTO with distalization compared to those that involved medialization alone [6]. Payne et al. documented complication rates of 10.70% in patients with detachment of the distal ridge during osteotomy, in contrast to a notably lower rate of 3.30% observed in patients who maintained the distal attachment [3]. In addition, in one case report, the author described a spontaneous fracture of the proximal tibia originating from the TTO site, occurring 7 months after the initial procedure [8].
In our case, the flat osteotomy without distalization, but with the discontinuation of the distal ridge, was performed; however, the osteotomy was confirmed as healed based on serial follow-up radiographs after 3 months.
Rehabilitation
Salari et al. proposed a protocol involving 6–8 weeks of non-weight-bearing status, alongside the use of a removable knee extension splint. They advised that participation in high-impact activities, contact sports, or any sports that generate significant impact forces should be avoided for a period of 9–12 months [9].
Stetson et al. emphasized that patients should remain non-weightbearing initially, progress gradually to partial weightbearing, and not resume full weightbearing until radiographic confirmation of osteotomy healing, noting that all reported fractures occurred only after postoperative protocols were changed from partial weightbearing to immediate full weightbearing. [10].
In our case, the patient was managed with a partial weight-bearing protocol for 6 weeks with a protective splint and did not participate in any sports activities for 3 months.
Treatment
There are several options for the treatment of fractures associated with TTO, and the approach remains debatable, with a tendency toward surgical intervention. Gödde et al., in their two-patient study, reported success with conservative cast treatment [11]. Similarly, Eager et al., in their one-patient study, reported the same success with cast immobilization treatment [12]. In Johnson’s study, the same cast treatment was implemented with success [6]. Pierre-Emmanuel Goetz et al., in one patient, reported advances with plating of the fracture area [8].
In our case, we opted for a lateral tibial pre-modulated locking plate as the treatment option, primarily to prevent the progression of the fracture.
Proximal tibial stress fractures are a rare but significant complication following tibial tuberosity osteotomy. Prevention relies on precise surgical technique, gradual rehabilitation, and early identification of symptoms, while surgical fixation remains a reliable treatment when fractures arise.
After careful consideration of all factors, to prevent proximal tibial stress fractures after TT osteotomy, perform an oblique osteotomy, use partial weight-bearing with protection for 6 weeks, avoid sports for at least 3 months, and if a fracture occurs, stabilize early with a locking plate to prevent progression.
References
- 1. Su P, Yao D, Zhang L, Li G. Results of medial patellofemoral ligament reconstruction with and without tibial tubercle osteotomy in patellar instability: A systematic review and single-arm meta-analysis. BMC Musculoskelet Disord 2024;25:642. [Google Scholar] [PubMed]
- 2. Rosso F, Rossi R, Cottino U, Bonasia DE. Tibial tubercle osteotomy for patellofemoral malalignment and chondral disease provided good outcomes: A systematic review. J ISAKOS 2022;7:78-86. [Google Scholar] [PubMed]
- 3. Payne J, Rimmke N, Schmitt LC, Flanigan DC, Magnussen RA. The incidence of complications of tibial tubercle osteotomy: A systematic review. Arthroscopy 2015;31:1819-25. [Google Scholar] [PubMed]
- 4. Trillat A, Dejour H, Couette A. Diagnosis and treatment of recurrent dislocations of the patella. Rev Chir Orthop Reparatrice Appar Mot 1964;50:813-24. [Google Scholar] [PubMed]
- 5. Fulkerson JP. Anteromedialization of the tibial tuberosity for patellofemoral malalignment. Clin Orthop Relat Res 1983;177:176-81. [Google Scholar] [PubMed]
- 6. Johnson AA, Cosgarea AJ, Wolfe EL. Complications of tibial tuberosity osteotomy. Sports Med Arthrosc Rev 2017;25:85-91. [Google Scholar] [PubMed]
- 7. Saltzman BM, Rao A, Erickson BJ, Cvetanovich GL, Levy D, Bach BR Jr., et al. A systematic review of 21 tibial tubercle osteotomy studies and more than 1000 knees: Indications, clinical outcomes, complications, and reoperations. Am J Orthop (Belle Mead, NJ) 2017;46:E396-407. [Google Scholar] [PubMed]
- 8. Goetz PE, Manon J, Quintart C. Delayed spontaneous fracture of the proximal tibia after tibial tubercle osteotomy for treatment of patella instability: A case report. J Orthop Case Rep 2023;13:80-5. [Google Scholar] [PubMed]
- 9. Salari N, Horsmon GA, Cosgarea AJ. Rehabilitation after anteromedialization of the tibial tuberosity. Clin Sports Med 2010;29:303-11, ix. [Google Scholar] [PubMed]
- 10. Stetson WB 1, Friedman MJ, Fulkerson JP, Cheng M, Buuck D Fracture of the proximal tibia with immediate weightbearing after a Fulkerson osteotomy. Am J Sports Med. 1997;25(4):570-574. [Google Scholar] [PubMed]
- 11. 11 Gödde S, Rupp S, Dienst M, Seil R, Kohn D. Fracture of the proximal tibia six months after Fulkerson osteotomy. A report of two cases. J Bone Joint Surg Br 2001;83:832-3. [Google Scholar] [PubMed]
- 12. 12 Eager MR, Bader DA, Kelly JD 4th, Moyer RA. Delayed fracture of the tibia following anteromedialization osteotomy of the tibial tubercle: A report of 5 cases. Am J Sports Med 2004;32:1041-8. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2023 Delayed Spontaneous Fracture of the Proximal Tibia after Tibial Tubercle Osteotomy for Treatment of Patella Instability: A Case Report
October 10, 2023 Delayed Spontaneous Fracture of the Proximal Tibia after Tibial Tubercle Osteotomy for Treatment of Patella Instability: A Case Report January 10, 2020 Pitfalls during Sacroiliac Joint Arthrodesis for Patients with Severe Sacroiliac Joint Pain: Report of Three Cases with Sacral Dysmorphism Induced by Lumbosacral Transitional Vertebrae
January 10, 2020 Pitfalls during Sacroiliac Joint Arthrodesis for Patients with Severe Sacroiliac Joint Pain: Report of Three Cases with Sacral Dysmorphism Induced by Lumbosacral Transitional Vertebrae October 10, 2015 Outcome Analysis following Operative Skeletal Stabilization in Established Non Unions of Malleolar Fractures – A Series of 11 Cases
October 10, 2015 Outcome Analysis following Operative Skeletal Stabilization in Established Non Unions of Malleolar Fractures – A Series of 11 Cases August 10, 2022 Complex Metacarpophalangeal Joint Dislocation of the Index Finger in Pediatric Age: A Case Report and Review of Literature
August 10, 2022 Complex Metacarpophalangeal Joint Dislocation of the Index Finger in Pediatric Age: A Case Report and Review of Literature