
Persistent ankle pain following minor trauma may indicate underlying talar vascular compromise, therefore, early advanced imaging is essential to diagnose occult fractures and prevent structural collapse.
Dr. Ehtesam Ahmed Chowdhury, Department of Trauma and Orthopaedic Surgery, Hereford County Hospital, Wye Valley NHS Trust, Hereford, England. E-mail: ehtesam.chowdhury2@nhs.net
Abstract
Introduction: Avascular necrosis (AVN) of the talus is an uncommon condition, although it can arise due to the bone’s limited blood supply and typically occurs following high-energy trauma or in patients with recognised medical risk factors. Fractures developing as a result of AVN, particularly vertical fractures through the talar body with early dome collapse, are relatively rare. This report describes a unique presentation in a patient without classical risk factors, highlighting delays in diagnosis and the complexities associated with management. This appears to be one of the few reported cases of a spontaneous vertical fracture of the talus secondary to AVN in a low-risk individual.
Case Report: A 47-year-old woman of no significant medical background presented with an 8-week history of progressive left ankle pain following minor trauma during a holiday. Initial assessment in the emergency setting suggested an ankle sprain, but persistent pain led to repeat clinic evaluation. Radiographs demonstrated a defect in the talar dome, and a subsequent urgent magnetic resonance scan revealed extensive involvement of the talar head and body with a vertical fracture extending into the dome, early medial collapse, and marked surrounding inflammation. The patient continued to experience deterioration despite immobilization, with increasing functional limitation, including difficulty managing stairs at home. A follow-up scan demonstrated non-union of the fracture and progressive collapse. While advanced reconstructive options such as total talus replacement were considered, ongoing systemic barriers, such as funding delayed access. Due to worsening symptoms, she underwent open reduction and internal fixation of the talar fracture as a temporizing measure whilst access to definitive management was sought.
Conclusion: This case highlights the aggressive course that talar AVN can take even in individuals with little to no risk factors. Early use of advanced imaging should be considered in patients with persistent ankle pain when initial radiographs are inconclusive, as delayed diagnosis may lead to structural collapse and reduced treatment options. This report adds to the understanding of atypical presentations of talar vascular insufficiency and underscores the importance of timely recognition, multidisciplinary decision-making, and addressing systemic barriers that may delay definitive care.
Keywords: Talar avascular necrosis, talar fracture, vertical talar body fracture, dome collapse; foot and ankle surgery.
Avascular necrosis (AVN) is a condition that occurs secondary to impaired perfusion of bone, which leads to ischemia and progressive tissue death. It can be divided into primary (idiopathic) or secondary (trauma, inflammatory conditions, alcohol misuse, medication, or genetic predisposition). The prevalence of AVN of the femoral head in the general United Kingdom population is two per 100,000 patients in the UK, with a mean age of 58.3, and more common in men aged between 25 and 44 and women between 55 and 75 years old [1]. AVN of the talus is relatively rare, accounting for a small percentage (2%) of all symptomatic cases of AVN [2]. The typical progression of AVN is described by the French radiologists Ficat and Arlet classification of osteonecrosis, from stage 0, or the “silent stage”, to stage 4, or the “terminal phase” [3]. Choi et al. further categorized AVN of the talus into “central talar dome”, where osteonecrotic lesions appear centrally without affecting the shoulder and being limited to the plafond, or “talar shoulder”, where one or both gutters is affected, extending into the talar dome (Fig. 1) [4].
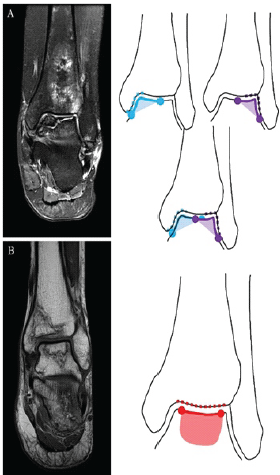
Figure 1: (a) Shoulder lesion of talar avascular necrosis (AVN) involves either the medial or lateral talar shoulder. (b) Non-shoulder lesion of talar AVN involves the central part of talar dome without shoulder area involvement.
We present a rare case of a young patient with AVN of the left talus leading to a vertical fracture through the talar body extending into the dome with superomedial collapse. The only potential risk factor identifiable was the use of vape.
A 47-year-old lady initially presented to the foot and ankle clinic in November of 2024 with an 8-week history of insidious onset of low-energy traumatic left ankle pain, which was noticed after returning from a holiday. This was initially diagnosed as an ankle sprain in the emergency department. Examination demonstrated anterolateral talar tenderness. X-rays repeated in the clinic demonstrated an osteochondral defect of the talar dome. She was sent home with walking boot for comfort, and an urgent magnetic resonance imaging (MRI) was requested. She was seen again in January of 2025 after her MRI, which reported extensive with segmental involvement of the head and posterior body, with a vertical fracture through the body extending into the talar dome and early superomedial dome collapse. Significant sinus tarsi edema and reactive synovitis were also evident (Fig. 2).
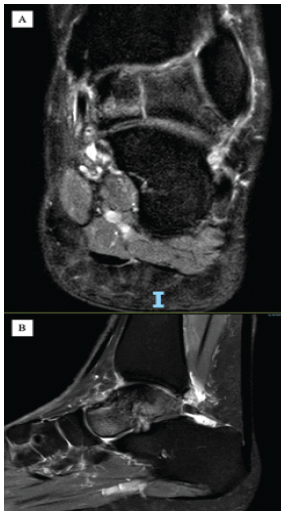
Figure 2: (a and b) T2-weighted magnetic resonance imaging of the ankle in the coronal plane sagittal plane, respectively. These demonstrate (1) extensive avascular necrosis of talus bone with involvement of head and posterior body, (2) vertical fracture through the talar body extending to talar dome, (3) significant sinus tarsi edema with associated reactive synovitis. Images were obtained locally from the picture archiving and communication system.
The patient reported persistent pain and swelling in the ankle joint despite the boot. She was given the options of attempting fixation, total talus replacement (TTR), conservative management with walking boot, analgesia and monitoring, or obtaining a second opinion for a tertiary center. After taking time to reflect, she elected to go down the surgical route. Therefore, a plan for bilateral ankle computed tomography (CT) with 3D reconstruction was formulated for custom implant design. She was seen in the clinic again in July 2025 with persisting symptoms. As there was an issue with obtaining funding for the operation from the National Health Service (NHS), her case was taken to the wider region multi-disciplinary team. The outcome of which as for one of three options: (1) conservative management with immobilization for 1–2 years, with the possibility that this was due to transient regional osteoporosis with self-limiting course, (2) fixation of the vertical split with internal pinning, (3) TTR with the acknowledgement that this is not a widely recommended surgery given the patients age. A re-application for an individual funding request was done and she remained on the waiting list. One month later, she was admitted through the acute route due to an acute increase in her ankle pain and swelling over several days. Functionally, she had deteriorated, with measures such as re-decorating her 2-story house to move everything downstairs due to inability to go up and down the stairs. On this admission, an acute infection such as septic or reactive arthritis was ruled out. A new MRI was performed, which demonstrated non-union of the fracture with arthritic changes and talar collapse, as well as the vertical fracture remaining unfused and unchanged from 2024. Given her deterioration, a plan was made to proceed with an open reduction and internal fixation of the talar fracture as a temporizing measure, while funding was still pending for a TTR (Fig. 3).
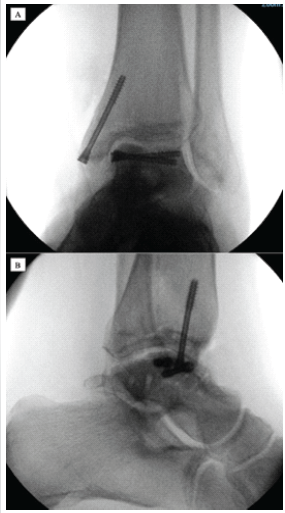
Figure 3: Intraoperative plain film imaging illustrating an open reduction and internal fixation of the previous unfused vertical fracture of the talar bone as a temporizing measure whilst awaiting definitive management. (a) Anteroposterior view. (b) Lateral view.
The case demonstrates the logistical difficulties in the diagnosis as well as the therapeutic challenges associated with AVN of the talus, a rare but potentially debilitation condition. Even though this patient had minimal to no risk factors, this case shows that a high index of suspicion is required in patients with persistent symptoms of ankle pain or post-traumatic pain in ankle where if plain radiographs are inconclusive, a CT scan may be required to diagnose or rule out fractures in the talus, despite absence of classical risk factors, such as high energy trauma or the more common causes like corticosteroid use, sickle cell disease or autoimmune diseases. AVN in the talus can be identified on radiography by an increase in the talar dome opacity and by articular collapse and fragmentation [5]. On MRI, AVN presents as a low signal on T1-weighted images and variable signal on T2-weighted images. The “double line” sign is considered pathognomonic but less common [6]. The consequences of AVN of the talus are disproportionately severe due to the talus’s tenuous blood supply and its central role in ankle and hindfoot biomechanics. In this patient’s case, the vertical fracture through the talar body extending into the dome, coupled with superomedial and later posteromedial collapse, reflects a progressive and structurally destabilizing pattern of necrosis. This aligns with Ficat classification’s later stages (III–IV), where subchondral collapse and joint space narrowing become evident. Choi et al.’s anatomical subclassification of talar AVN into “central” and “shoulder” lesions offers valuable prognostic insight. The involvement of the superomedial and posteromedial dome in this case supports a shoulder-type lesion, associated with a higher risk of progression and collapse. The persistence of the vertical fracture without healing supports the diagnosis of advanced AVN rather than transient regional osteoporosis. While conservative and joint-salvaging treatments are usually first-line management options, these are reserved for Stage I, II, and potentially early-stage III disease. Stage III-IV disease are indications for joint-sacrificing procedures, such as fusion, or partial or total talar replacements [7]. Studies, however, suggest TTR may offer superior outcomes in younger patients compared to fusion, especially in terms of mobility and long-term joint preservation [8,9]. This case also illustrates the systemic barriers to care within the NHS, where access to advanced surgical interventions may be limited by funding constraints. The patient’s functional decline, manifested by lifestyle adaptations such as relocating her living space, emphasizes the real-world impact of delayed intervention [10].
This case depicts the aggressive nature of talar AVN, the use of classification systems in guiding prognosis, and the need for timely, individualized management strategies. It also calls attention to the importance of multidisciplinary decision-making and advocacy for patients navigating complex care pathways.
Early use of cross-sectional imaging in patients with persistent ankle pain can prevent missed diagnoses of talar osteonecrosis, a condition that may rapidly progress to collapse. Recognition of systemic barriers, such as delayed access to advanced interventions are essential for optimizing outcomes and retaining patient function.
References
- 1. Edwards CJ. Avascular necrosis of bone. BMJ 2019;365:l2178. [Google Scholar] [PubMed]
- 2. Yu GV, Judge MS, Hudson JR, Seidelmann FE. Talar osteonecrosis: Diagnosis and management. Foot Ankle Clin 2018;23:593-616. [Google Scholar] [PubMed]
- 3. Ficat RP. Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment. J Bone Joint Surg Br 1985;67:3-9. [Google Scholar] [PubMed]
- 4. Choi YS, Lee JW, Lee GY, Kim S, Choi JA, Kim BS. Avascular necrosis of the talus: Classification and imaging findings. BMC Musculoskelet Disord 2023;24:7136. [Google Scholar] [PubMed]
- 5. Pearce DH, Mongiardi CN, Fornasier VL, Daniels TR. Avascular necrosis of the talus: A pictorial essay. Radiographics 2005;25:399-410. [Google Scholar] [PubMed]
- 6. Zhang H, Fletcher AN, Scott DJ, Nunley J. Avascular osteonecrosis of the talus: Current treatment strategies. Foot Ankle Int 2022;43:291-302. [Google Scholar] [PubMed]
- 7. Tian L, Liu G, Zheng S, Hu K, Zhang W. Total talus replacement for talar avascular necrosis: A review of current concepts. Medicina 2024;60:1692. [Google Scholar] [PubMed]
- 8. Foot Innovate Exchange. Talar Avascular Necrosis: Replace, Don’t Fuse. Available from: https://www.footinnovatexchange.com/post/talar-avascular-necrosis-replace-don-t-fuse [Last accessed on 20th November 2025]. [Google Scholar] [PubMed]
- 9. Lareau CR, Richey J. Total talus replacement: indications, technique, and outcomes. J Foot Ankle Surg 2021;60:S29-36. [Last accessed on 20th November 2025]. [Google Scholar] [PubMed]
- 10. The King’s Fund. Tight Budgets, Tough Choices: The Pressures Facing England’s National Health Service; 2023. Available from: https://www.kingsfund.org.uk/insight-and-analysis/long-reads/tight-budgets-tough-choices [Last accessed on 20th November 2025]. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Reconstruction of Recurrent First Metatarsal Giant Cell Tumor with Vascularized Metatarsal Transfer: Long-Term Functional Outcomes
January 1, 2026 Reconstruction of Recurrent First Metatarsal Giant Cell Tumor with Vascularized Metatarsal Transfer: Long-Term Functional Outcomes November 1, 2025 Restoring Sagittal Alignment: Anterior Open-Wedge Flexion Valgus Osteotomy for Post-Traumatic Genu Recurvatum with Reversed Posterior Tibial Slope – A Rare Case Report
November 1, 2025 Restoring Sagittal Alignment: Anterior Open-Wedge Flexion Valgus Osteotomy for Post-Traumatic Genu Recurvatum with Reversed Posterior Tibial Slope – A Rare Case Report May 10, 2024 Spontaneous First Metatarsal Rotational Correction by the Syndesmosis Procedure for Hallux Valgus Deformity: A Case Report
May 10, 2024 Spontaneous First Metatarsal Rotational Correction by the Syndesmosis Procedure for Hallux Valgus Deformity: A Case Report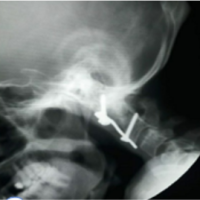 June 22, 2021 Basilar Invagination: Surgical Treatment by Novel Anterior Implant
June 22, 2021 Basilar Invagination: Surgical Treatment by Novel Anterior Implant