
Chronic patellar tendon rupture should be suspected in any patient with extensor lag and patella alta after knee trauma. Delayed presentation necessitates biological reconstruction rather than simple end-to-end repair. Semitendinosus–gracilis autografts provide strong, implant-free augmentation for extensor mechanism restoration. Modified Ecker’s single-tunnel, tension-band–like configuration can achieve stable fixation while reducing fracture risk.
Dr. S. Gokul, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospital, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: gokulsubramaniam96@gmail.com
Abstract
Introduction: Patellar tendon rupture is an uncommon injury that may progress to a chronic or neglected state when initial diagnosis and treatment are delayed.
Case Report: We report the case of a 17-year-old male who sustained a cut-laceration injury over the right knee that was sutured primarily elsewhere, following which he developed progressive instability and inability to actively extend the knee. Imaging revealed patella alta with a complete patellar tendon rupture. The patient underwent reconstruction using a modified Ecker’s technique with semitendinosus and gracilis autografts passed through single tibial and patellar tunnels in figure-of-eight and figure-of-seven configurations, respectively, to restore the extensor mechanism. Post-operative rehabilitation involved staged mobilization with a hinged knee brace and progressive range-of-motion exercises. At 1-year follow-up, the patient had regained functional knee flexion, returned to daily activities, and demonstrated only minimal residual extension lag.
Conclusion: This case highlights the effectiveness of hamstring autograft reconstruction using a biologic tension-band–like configuration for chronic neglected patellar tendon ruptures, allowing stable fixation, early rehabilitation, and satisfactory functional recovery
Keywords: Chronic patellar tendon rupture, neglected knee injury, hamstring autograft, semitendinosus–gracilis reconstruction, modified Ecker’s technique, extensor mechanism restoration.
Patellar tendon tears become chronic or overlooked if not properly diagnosed, and these tears are rare [1]. The incidence is 0.68/100000 [2]. These tears are seen in people under 40 years of age. The main goal of treating these tears is to restore the extensor mechanism that facilitates active knee extension. This can be achieved by end-to-end suturing or re-stitching. This is usually combined with further reconstruction to protect the affected tendon [3]. We report a 17-year-old boy with a neglected chronic patellar tendon tear after a cut-injury. The patient presented with limping and an inability to do a full extension of the knee following a cut injury 9 months ago.
A 17-year-old male patient came with a history of a cut laceration injury to the right knee that happened 9 months back, and the wound was sutured in a private hospital. Following the wound healing, he had instability while walking and an inability to extend the knee. Physical examination revealed extensor lag with a high-riding patella without limb length discrepancy and post-traumatic scar healed with secondary indention over the knee joint (Fig. 1).

Figure 1: Extensor lag, high-riding patella.
Investigations
A roentgenogram of the right knee showed a patella alta with an avulsion fragment on the lower pole of the patella (Fig. 2).

Figure 2: X-ray showing patella alta.
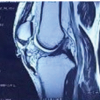
Magnetic resonance imaging of the right knee showed a complete tear of the patellar tendon with inflammatory changes in the Hoffman pad of fat and minimal fluid in the infrapatellar region. The patella was displaced superiorly, suggesting Grade-1 medial collateral injury (Fig. 3).
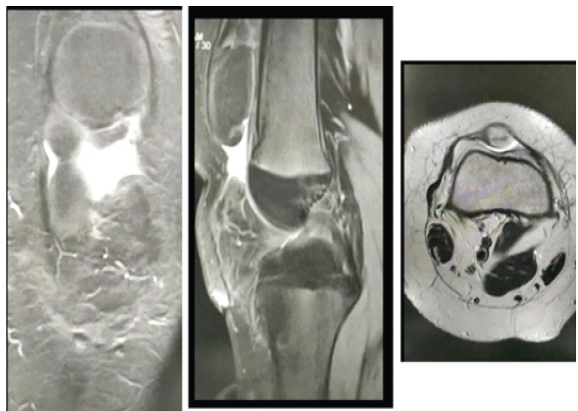
Figure 3: Magnetic resonance images, coronal, sagittal, and axial views.
Surgical intervention
The patient underwent surgical reconstruction of a neglected patellar tendon using semitendinosus (ST) and gracilis graft. By the modification of Ecker’s technique, graft was harvested and prepared using a single horizontal tunnel in the tibia and patella, and the ST graft as a single longitudinal bundle in figure of eight pattern whereas gracilis is inserted in the figure of seven pattern through a single tunnel in the tibia as well as patella (Fig. 4).
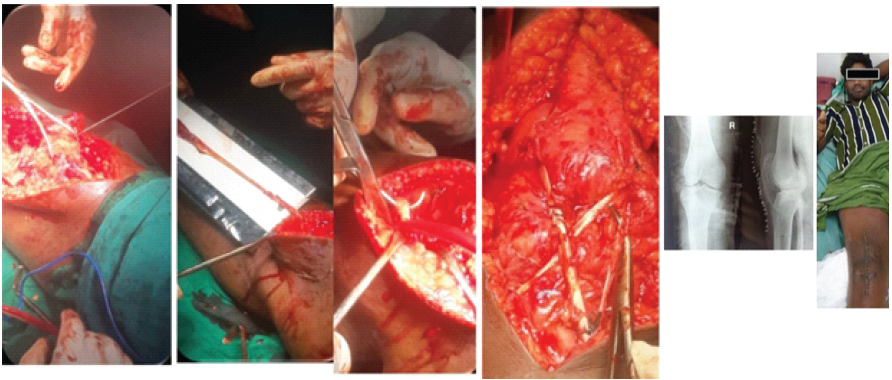
Figure 4: Intraoperative images and post-operative check X-ray.
This technique of graft insertion is different from the Eckers technique which provides a more tensile strength figure of eight biological grafts that act like a tension band wiring of the patellar tendon whereas the other strand gives additional stability in the longitudinal direction which helps the patient in early rehabilitation and return to daily activity earlier.
Outcome and follow-up
Postoperatively sutures were removed after 2 weeks. The patient was started on continuous passive motion for the next 3 days, up to 20°–30° for 3 days. After a hinged knee brace was applied, continued knee range of motion (ROM) exercises were performed twice daily for 4 weeks. After 6 weeks, the range of movements increased to 70°–90° of knee flexion. At the end of 5 months, flexion achieved up to 110°, and the patient returned to daily manual labor. Five degrees of extension lag persisted as a sequel of neglect (Fig. 5).

Figure 5: Post-operative follow-up at 3rd, 6th month, and 1 year.
Although the actual frequency of patellar tendon rupture is unknown, it ranks third among extensor mechanism injuries, following quadriceps tendon rupture and patella fracture [1]. A complete patellar tendon rupture occurs in 97% of cases documented in the literature, and is frequently near the pole of the patella [2]. Fresh patellar tendon ruptures, which typically occur at the inferior pole of the patella, necessitate urgent surgical restoration of the extensor mechanism for best recovery to pre-injury functional status. Conservative treatment plays no function, and surgical repair yields the best results if performed within 1 week of injury. Siwek and Rao observed 80% excellent and 16% good outcomes in patients treated with primary repair after 7 days of damage; however, results dropped in patients treated 2 weeks or more after injury, with only 33% excellent and 50% good results [3]. End-to-end repair is used with or without a strengthening cerclage suture made of wire or non-absorbable suture material; alternatively, tape and cast immobilization is indicated for 6–8 weeks after surgery. Immediate repairs of fresh patellar tendon ruptures have been shown to improve ROM, quadriceps muscle strength, and overall functional outcomes. Neglected rupture of the patellar tendon is a rare condition. Even if the proper physical examination is performed, patellar tendon rupture can be easily missed in patients with multi trauma, obesity, and knee hemarthrosis. When treatment is delayed for more than 6 weeks, simple re-approximation of the severed tendon ends becomes problematic. The longer the time between injury and repair, the higher the risk of quadriceps retraction and proximal patellar migration. Fibrous adhesions may form between the patella and the underlying femur. The torn tendon ends shrivel up and become covered with scar tissue. In two cases, some writers performed reconstruction and restoration of the neglected patellar tendon utilizing ST and gracilis tendons with preserved distal insertions [4]. Some other studies using a contralateral bone-patellar tendon-bone graft followed by double-wire loop reinforcement [4], bone-patellar tendon-bone allograft [5], Achilles tendon allograft [6], and synthetic materials [7] have also performed previously. Primary repair combined with autogenous graft augmentation using fascia lata or hamstring tendons has been most commonly used. The current approach consists of lowering the proximally migrated patella through intraoperative sectioning of the patellar retinaculum and release of the suprapatellar bursa by arthrolysis [8]. Ecker et al. [9] were the first to describe the use of hamstring tendon autograft in the reconstruction of chronic patellar tendon injuries. In their technique, they drilled 2 patellar and 2 tibial tunnels in a horizontal fashion, i.e., separate tunnels for the ST and gracilis. We believe this poses a high risk of intraoperative patellar or tibial fractures. There is also the risk of breaching the patellar articular cartilage. We performed reconstruction and restoration of ruptured patellar tendons using STG tendons. We suggest that this modified technique has several advantages. STG tendons are rich in tendon fibers and can be used to yield a strong graft; the ultimate tensile load of doubled ST tendon grafts has been reported to reach 2330 N [9,10], and they are often used in anterior cruciate ligament (ACL) reconstructions. We did not use wire cerclage, and this may have reduced the risk of infection and obviated the need for a second intervention to remove the implanted material. This method of graft insertion acts like biological tension band wiring, which helps in faster recovery and improved functional outcome of the patient.
Chronic neglected patellar tendon ruptures present significant reconstructive challenges because of proximal patellar migration, tendon retraction, and surrounding fibrosis. Reconstruction using a modified Ecker’s technique with ST and gracilis autografts through single tibial and patellar tunnels provided stable biological fixation, restored the extensor mechanism, and permitted early, structured rehabilitation in this adolescent patient. The tension-band–like graft configuration avoided the need for metallic augmentation and a second surgery for implant removal while achieving satisfactory functional recovery. This technique appears to be a reliable option for managing chronic patellar tendon ruptures, particularly in young, active individuals, though larger series and longer follow-up are required to confirm reproducibility and long-term outcomes.
Modified Ecker’s hamstring autograft reconstruction is a reliable biological option for neglected patellar tendon ruptures, enabling stable fixation, early rehabilitation, and satisfactory functional outcomes in young active patients
References
- 1. Kannus P, Natri A. Etiology and pathophysiology of tendon ruptures in sports. Scand J Med Sci Sports 1997;7:107-12. [Google Scholar] [PubMed]
- 2. Greis PE, Holmstrom MC, Lahav A. Surgical treatment options for patella tendon rupture, Part I: Acute. Orthopedics 2005;28:672-9. [Google Scholar] [PubMed]
- 3. Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am 1981;63:932-7. [Google Scholar] [PubMed]
- 4. Chen B, Li R, Zhang S. Reconstruction and restoration of neglected ruptured patellar tendon using semitendinosus and gracilis tendons with preserved distal insertions: Two case reports. Knee 2012;19:508-12. [Google Scholar] [PubMed]
- 5. Casey MT Jr., Tietjens BR. Neglected ruptures of the patellar tendon. A case series of four patients. Am J Sports Med 2001;29:457-60. [Google Scholar] [PubMed]
- 6. Milankov MZ, Miljkovic N, Stankovic M. Reconstruction of chronic patellar tendon rupture with contralateral BTB autograft: A case report. Knee Surg Sports Traumatol Arthrosc 2007;15:1445-8. [Google Scholar] [PubMed]
- 7. Lewis PB, Rue JP, Bach BR Jr. Chronic patellar tendon rupture: surgical reconstruction technique using 2 Achilles tendon allografts. J Knee Surg 2008;21:130-5. [Google Scholar] [PubMed]
- 8. ElGuindy A, Lustig S, Servien E, Fary C, Weppe F, Demey G, et al. Treatment of chronic disruption of the patellar tendon in osteogenesis imperfecta with allograft reconstruction. Knee 2012;18:121-4. [Google Scholar] [PubMed]
- 9. Ecker ML, Lotke PA, Glazer RM. Late reconstruction of the patellar tendon. J Bone Joint Surg Am 1979;61:884-6. [Google Scholar] [PubMed]
- 10. Suydam SM, Cortes DH, Axe MJ, Snyder-Mackler L, Buchanan TS. Semitendinosus tendon for ACL reconstruction: Regrowth and mechanical property recovery. Orthop J Sports Med 2017;5:2325967117712944. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Patellar Tendon Reconstruction Using Ipsilateral Hamstring or Peroneal Autografts – A Case Series of Five Patients
May 1, 2026 Patellar Tendon Reconstruction Using Ipsilateral Hamstring or Peroneal Autografts – A Case Series of Five Patients June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study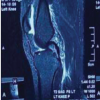 May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes
May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes May 11, 2018 Atypical Osteonecrosis of Humeral Head FollowingAnterior Shoulder Dislocation
May 11, 2018 Atypical Osteonecrosis of Humeral Head FollowingAnterior Shoulder Dislocation