
Simultaneous ACL reconstruction with meniscal repair ensures better functional outcomes, pain relief, and long-term knee joint preservation.
Dr. Sandip Kumar Verma, Department of Orthopaedics, Pt. J.N.M. Medical College and Dr. B.R.A.M. Hospital, Raipur, Chhattisgarh, India. sandipkumarvermacims@gmail.com
Introduction: Combined anterior cruciate ligament (ACL) and meniscus injuries are common in active individuals. This study evaluates the outcomes of arthroscopic ACL reconstruction with simultaneous meniscus repair.
Materials and Methods: A prospective study of 14 patients undergoing ACL reconstruction with meniscus repair was conducted. Lysholm Knee Score and Visual Analog scale (VAS) were used for outcome assessment. Intraoperative and post-operative complications were recorded.
Results: All 14 patients had poor pre-operative Lysholm Scores (mean 25.2). At 6 months, 71.4% achieved excellent outcomes, with the mean score improving to 92 (P < 1.54 × 10⁻¹⁷). Mean VAS scores decreased from 4 pre-operatively to 0.8 at 6 months (P < 1.98 × 10⁻12), indicating significant functional recovery and pain relief.
Conclusion: Arthroscopic ACL reconstruction with meniscus repair provides excellent functional outcomes with minimal complications.
Keywords: Anterior cruciate ligament, meniscus repair, arthroscopy, lysholm score, Visual Analog Scale, clinical outcome.
Combined injuries to the anterior cruciate ligament (ACL) and menisci are frequently observed in acutely injured knees and represent significant trauma in young, active patients [1]. The meniscus has a crucial role in knee biomechanics, aiding in load distribution, shock absorption, and joint stability. Many studies have reported a strong link between ACL injuries and meniscal tears, with meniscal damage commonly present in patients undergoing ACL reconstruction [2,3]. Advancements in arthroscopic techniques have improved surgical management and clinical outcomes, with reported success rates reaching up to 92% during ACL reconstruction [4]. However, the timing of ACL reconstruction and the extent of meniscal injury remain key factors affecting success. Delayed ACL reconstruction is associated with increased prevalence and severity of meniscal tears, emphasizing the importance of timely surgical intervention. Therefore, we conducted a prospective study to assess the clinical outcomes of arthroscopic ACL reconstruction with simultaneous meniscus repair, evaluating success and failure rates along with subsequent patient functional outcomes [5].
This was a prospective, observational study conducted in the Department of Orthopedics, Pt. J.N.M. Medical College and Dr. B.R.A.M. Hospital, Raipur (C.G.), after obtaining approval from the Institutional Ethical Committee. The study period extended from March 2023 to March 2025. All patients fulfilling the selection criteria and admitted during this period were included. Patients who underwent arthroscopic ACL reconstruction with simultaneous meniscus repair formed the study group. Data were collected using a structured and pre-validated pro forma. Each patient underwent detailed history taking, thorough clinical and radiographic examination, followed by surgical intervention. Loss to follow-up was considered as a potential source of bias. Inclusion criteria consisted of patients above 18 years of age with a traumatic ACL tear associated with medial, lateral, or combined meniscal injury, where the injury was <1-year-old. Exclusion criteria included ACL tears associated with fracture, collateral ligament or complex multi-ligament injuries, ipsilateral bony injuries, significant osteoarthritis, pathological degenerative ACL tears (such as due to mucoid degeneration), meniscal injuries not amenable to repair, and patients unwilling to give consent. Informed written consent was obtained from all participants in Hindi or English, using a patient information sheet and consent form.
All patients fulfilling the inclusion criteria underwent surgery after informed consent and pre-operative fitness assessment. Standard pre-operative preparations included intravenous ceftriaxone 1 g administered 30 min before incision, shaving of the operative site, spinal anesthesia, and application of a pneumatic tourniquet. Patients were positioned supine with the operative leg flexed at 90° and hanging from the side of the table. Arthroscopy was performed via anterolateral and anteromedial portals; in bucket-handle tears, a central trans patellar portal was used. Diagnostic arthroscopy confirmed ACL and meniscal tears. Semitendinosus tendon autograft was harvested through a 4 cm medial tibial incision, quadrupled, and prepared on a graft board. Femoral and tibial tunnels were created arthroscopically, with femoral fixation achieved using an Endo Button and tibial fixation with an interference screw. Meniscus repair was performed using all-inside techniques for posterior horn tears and inside-out or all-inside techniques for body and anterior horn tears, with prior debridement and rasping to enhance healing. Post-operatively, patients were immobilized in a long knee brace, received intravenous antibiotics for 3 days, and had dressings changed at 72 h. Sutures were removed at 2 weeks, and rehabilitation included early mobilization and strengthening exercises under protocol-based physiotherapy (Fig. 1).
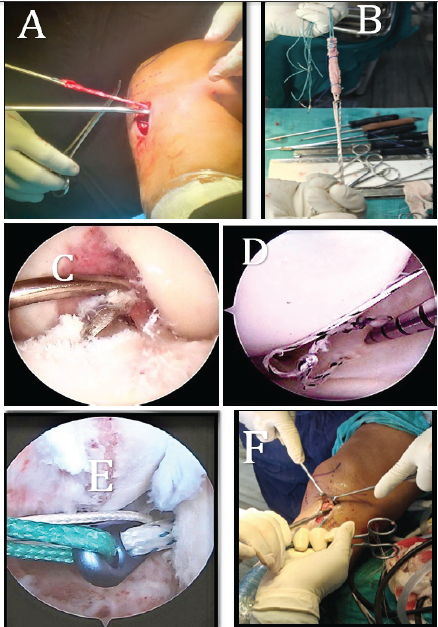
Figure 1: (a) Semitendinosus graft harvesting. (b) Quadrupling of semitendinosus graft. (c) Tibial tunneling. (d) All inside repair of meniscus. (e) Shuttling of graft with the Endo button. (f) Tibial fixation of anterior cruciate ligament reconstruction with interference screw.
Follow-up and assessment criteria
All patients were followed up at 6 weeks, 3 months, and 6 months post-operatively. Functional outcomes were assessed using the Lysholm Knee Scoring Scale, which comprehensively evaluates stability, pain, swelling, stair climbing, and overall mobility. Pain was specifically evaluated using the Visual Analog Scale (VAS), providing a reliable measure of symptom improvement over time.
Age incidence
In our study, the age of patients was in the range from a minimum of 22 years to a maximum of 37 years, with a mean age of 25.9 years (Table 1).
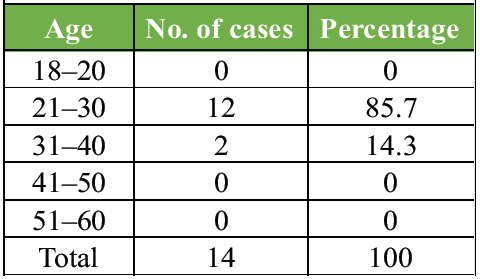
Table 1: Age incidence
Sex incidence
Males were significantly more likely to experience this type of injury, accounting for 78.6% of patients compared to 21.4% in females.
Mode of injury
Among the 14 cases, sports injuries were the most common mode of injury, occurring in 7 cases (50%). Road traffic accidents (RTA) were responsible for 4 cases (28.6%), while other causes accounted for 3 cases (21.4%) (Table 2).

Table 2: Mode of injury
Type of sports
Among the total cases, 7 patients sustained sports-related injuries. The majority were injured while playing football (3 patients, 42.8%), followed by high jump (2 patients, 28.6%), long jump (1 patient, 14.3%), and kho-kho (1 patient, 14.3%).
Side of injured knee
In our study of 14 injured patients, 5 had injuries on the left side, while 9 had injuries on the right side.
Type of ACL tear
In our study, 10 out of 14 patients (71.4%) experienced a complete ACL tear, while the remaining 4 patients (28.6%) had a partial tear (Table 3).
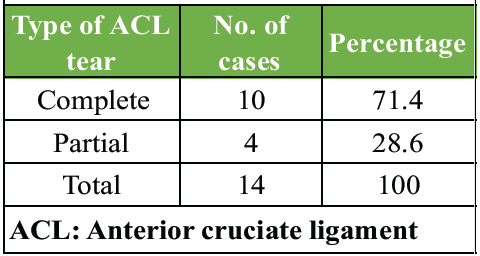
Table 3: Type of ACL tear
Side of meniscus injury
In our study, the medial meniscus was injured in 10 out of 14 patients (71.4%), whereas the lateral meniscus was injured in 4 patients (28.6%) (Table 4).
Type of meniscus tear
In our study, the longitudinal type of meniscus tear was the most common, occurring in 8 patients (57.2%). The bucket handle tear was observed in 4 patients (28.4%), while both the horizontal tear and radial tear were identified in 1 patient each (7.1%). No patients with oblique tears were recorded.
Type of meniscus tear
In our study, the most common type of meniscal tear was the longitudinal tear, observed in 50% of medial meniscus cases and 75% of lateral meniscus cases. The second most common tear type was the bucket-handle tear, seen in 30% of medial and 25% of lateral meniscus cases. Other tear types, such as horizontal and radial tears, were found only in the medial meniscus, each accounting for 10%. No complex or oblique tears were identified in either meniscus.
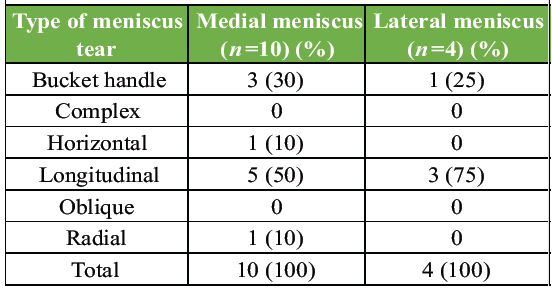
Table 4: Type of meniscus tear
Pre-operative manual knee laxity test
A manual knee laxity test was performed in all 14 cases of ACL injury. First, it was performed in the normal knee, which was taken as the standard of that patient, and then it was performed in the injured side. It was recorded as +, ++, +++ (if positive) and (if negative). Anterior drawer test, Lachman test, and pivot shift test were positive in 100% cases. Various grades of these tests are shown in Table.
Pre-operative McMurray test
In our study, the McMurray test was positive in 9 cases (64.3%) and negative in 5 cases (35.7%).
Trauma surgery interval
Among the 14 patients, the interval between trauma and surgery varied. Most patients (57.1%) underwent surgery within 2 to 6 months after the trauma, accounting for 8 patients. A smaller proportion, 14.3% (2 patients), had surgery between 7 and 10 months after the trauma. The remaining 28.6% (4 patients) had surgery within 11–12 months. The mean interval between trauma and surgery in our study was 7 months.
Surgical technique used for meniscus repair
In our study, the all-inside surgical technique was the most used method for meniscus repair, performed in 11 patients (78.6%). The inside-out technique was used in 3 patients (21.4%).
Lysholm Knee Score
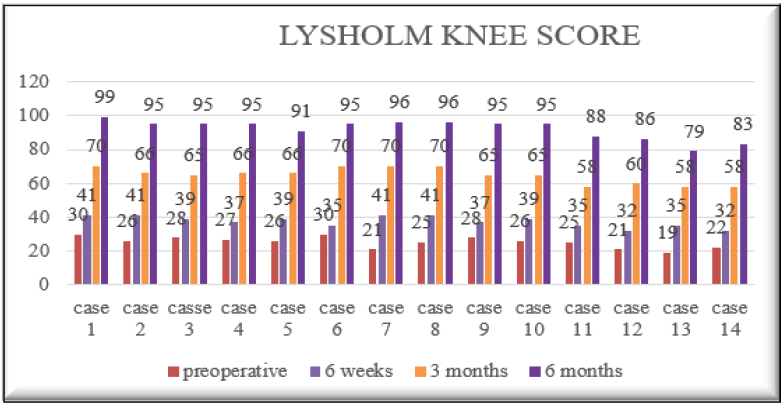
Pre-operatively, all 14 patients (100%) had poor Lysholm scores (mean 25.2). At 6 weeks, patients remained in the poor category (mean 37.4). By 3 months, 71.4% improved to fair and 28.6% remained poor (mean 64.7). At 6 months, no patient was poor; 71.4% achieved excellent, 14.3% good, and 14.3% fair outcomes, with a mean Lysholm Score of 92, indicating substantial functional recovery. A statistical comparison between pre-operative and 6-month follow-up Lysholm Scores using a paired t-test revealed a highly significant difference (t = 62.88, P < 0.0000000000000000154/P < 1.54 × 10⁻17), indicating that the observed improvement in knee function was statistically significant.(Table 5)
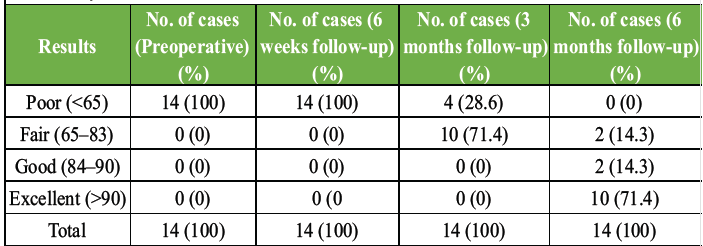
Table 5: Lysholm knee score
VAS score
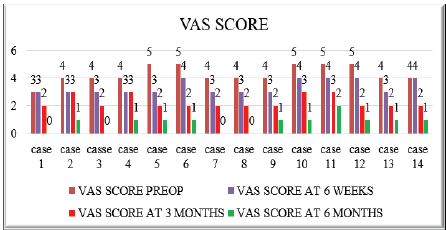
VAS scores showed progressive improvement post-operatively. The mean score decreased from 4 pre-operatively to 3.3 at 6 weeks, 2.2 at 3 months, and 0.8 at 6 months. By final follow-up, 92.9% of patients reported minimal or no pain (VAS 0–1), with no patient scoring ≥3 (image 2). A paired t-test comparing pre-operative and 6-month follow-up VAS scores demonstrated a statistically significant reduction in pain levels (t = 25.24, P = 0.00000000000198/P < 1.98 × 10⁻12), indicating that the improvement in VAS scores was highly significant. (Table 6)
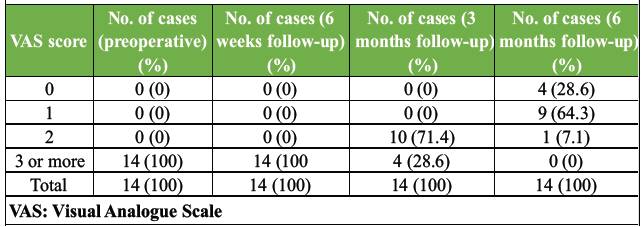
Table 6: VAS score
Complication
No major complication was seen in our study except numbness in 4 cases (28.6%), stiffness in 1 case (7.1%), and superficial infection in 1 case (7.1%) (Table 7).
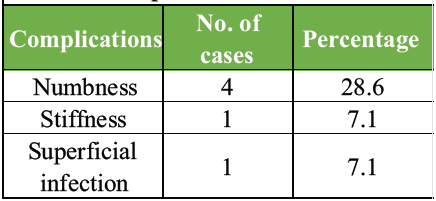
Table 7: Complication
In this study, the mean age of patients was 25.9 years, with the majority (85.7%) falling within the 21–30 years age group, reflecting the higher incidence of ACL–meniscus injuries in young, active populations. A predominance of male patients (78.6%) was observed, similar to previous findings by Soni et al. [6] and Keyhani et al. [3] Sports-related trauma accounted for half of the injuries, followed by RTAs (28.6%), aligning with the results reported by Majeed et al. [7]. Right knee involvement was more common (64.3%), comparable to the observations of Keyhani et al. [3]. Complete ACL tears were present in most patients (71.4%), consistent with the findings of Alsubaie et al. [8]. Medial meniscus injuries were more frequent (71.4%) than lateral ones (28.6%), as also described by Venkataraman et al. [2] and Rochcongar et al. [9]. Longitudinal meniscal tears were the predominant pattern (57.2%), followed by bucket-handle tears (28.6%), supporting prior reports by Westermann et al. [1] and Toman et al. [10]. Clinical tests demonstrated high diagnostic reliability: The anterior drawer, Lachman, and Pivot Shift tests were positive in all patients, in agreement with Benjaminse et al. [11]. The McMurray test identified 64.3% of meniscus tears but had some false negatives, consistent with Jain et al. [12]. Regarding meniscal repair, the all-inside technique was utilized in 78.6% of cases, primarily for posterior horn tears, whereas the inside-out technique was applied in 21.4% for anterior and mid-body tears. This approach aligns with trends reported by Westermann et al. [1], Dzidzishvili et al. [13], and Rodríguez Roiz et al. [14], offering advantages, such as reduced invasiveness, shorter surgery duration, and favorable healing outcomes. Functional recovery was excellent: Mean Lysholm Scores improved from 25.2 pre-operatively to 92 at 6 months, with 71.4% of patients achieving excellent outcomes, 14.3% good, and 14.3% fair. Pain, measured by VAS, decreased from 4 to 0.8, with 92.9% of patients reporting minimal or no pain. These results are comparable to those described by Arya et al. [15], Pathak et al. [16], and Sarraj et al. [17]. Minor complications included numbness (28.6%), stiffness (7.1%), and superficial infection (7.1%), most of which resolved within 6 months, consistent with findings by Inderhaug et al. and Horteur et al. Overall, simultaneous ACL reconstruction with meniscus repair, predominantly using the all-inside technique, provided excellent functional improvement, significant pain relief, and minimal complications. These findings reinforce the importance of early surgical intervention and meniscal preservation in managing ACL–meniscus injuries.
This study shows that arthroscopic ACL reconstruction combined with simultaneous meniscus repair provides excellent functional improvement, significant pain reduction, and a high likelihood of returning to activity in young, active individuals. The predominance of medial meniscus injuries and the favorable outcomes with both all-inside and inside-out repair techniques underscore the importance of preserving the meniscus in ACL-deficient knees. With minimal complications and marked improvements in Lysholm and VAS scores, this combined approach is a safe and effective treatment option. Early surgical management, coupled with structured rehabilitation, is essential for achieving optimal long-term outcomes and reducing the risk of degenerative joint changes.
Limitation
This study has certain limitations. The small sample size and single-center design may limit statistical power and generalizability. Follow-up was limited to 6 months, focusing on early post-operative recovery rather than long-term graft integrity, meniscal healing, or osteoarthritic changes. The absence of a control group and lack of randomization may introduce selection bias and limit the comparative interpretation of outcomes. Functional assessment was restricted to Lysholm and VAS scores, and objective evaluation of meniscal healing using post-operative magnetic resonance imaging or second-look arthroscopy was not performed. Inclusion of varied meniscal tear patterns and individualized selection of repair techniques based on tear configuration and surgeon discretion may have contributed to outcome variability. Pain assessment was limited to the short term, and objective return-to-sport outcomes were not formally assessed. Although a standardized rehabilitation protocol was advised, individual compliance could not be objectively quantified. Exclusion of complex and multiligament knee injuries limits applicability to such cases. Radiological or biomechanical evaluation of tunnel placement, graft incorporation, and knee kinematics was not performed. Finally, the predominance of young male patients reflects the typical demographic presenting with ACL injuries but limits extrapolation to other populations.
Simultaneous ACL reconstruction with meniscal repair provides excellent functional outcomes and pain relief. Meniscal preservation at the time of ACL surgery is crucial for knee stability and long-term joint health.
References
- 1. Westermann RW, Wright RW, Spindler KP, Huston LJ, MOON Knee Group, Wolf BR. Meniscal repair with concurrent anterior cruciate ligament reconstruction: Operative success and patient outcomes at 6-year follow-up. Am J Sports Med 2014;42:2184-92. [Google Scholar] [PubMed]
- 2. Venkataraman S, Ethiraj P, Shanthappa AH, Vellingiri K. Association of meniscus injuries in patients with anterior cruciate ligament injuries. Cureus 2022;14:e25878. [Google Scholar] [PubMed]
- 3. Keyhani S, Esmailiejah AA, Mirhoseini MS, Hosseininejad SM, Ghanbari N. The prevalence, zone, and type of the meniscus tear in patients with anterior cruciate ligament (ACL) injury; does delayed ACL reconstruction affects the meniscal injury? Arch Bone Jt Surg 2020;8:432-8. [Google Scholar] [PubMed]
- 4. Yang YP, Ma X, An H, Liu XP, An N, Ao YF. Meniscus repair with simultaneous anterior cruciate ligament reconstruction: Clinical outcomes, failure rates and subsequent processing. Chin J Traumatol 2022;25:37-44. [Google Scholar] [PubMed]
- 5. Vaquero-Picado A, Rodríguez-Merchán EC. Arthroscopic repair of the meniscus: Surgical management and clinical outcomes. EFORT Open Rev 2018;3:584-94. [Google Scholar] [PubMed]
- 6. Soni S, Mankad SP, Sharma D, Patel K, Soni H, Shroff MR, et al. Impact of meniscus repair in conjunction with anterior cruciate ligament reconstruction on functional outcomes at six months. Cureus 2024;16:e54999. [Google Scholar] [PubMed]
- 7. Majeed H, Karuppiah S, Sigamoney KV, Geutjens G, Straw RG. All-inside meniscal repair surgery: Factors affecting the outcome. J Orthop Traumatol 2015;16:245-9. [Google Scholar] [PubMed]
- 8. Alsubaie SF, Abdelbasset WK, Alkathiry AA, Alshehri WM, Azyabi MM, Alanazi BB, et al. Anterior cruciate ligament injury patterns and their relationship to fatigue and physical fitness levels – a cross-sectional study. Medicine (Baltimore) 2021;100:e24171. [Google Scholar] [PubMed]
- 9. Rochcongar G, Cucurulo T, Ameline T, Potel JF, Dalmay F, Pujol N, et al. Meniscal survival rate after anterior cruciate ligament reconstruction. Orthop Traumatol Surg Res 2015;101 8 Suppl:S323-6. [Google Scholar] [PubMed]
- 10. Toman CV, Dunn WR, Spindler KP, Amendola A, Andrish JT, Bergfeld JA, et al. Success of meniscal repair at anterior cruciate ligament reconstruction. Am J Sports Med 2009;37:1111-5. [Google Scholar] [PubMed]
- 11. Benjaminse A, Gokeler A, Van Der Schans CP. Clinical diagnosis of an anterior cruciate ligament rupture: A meta-analysis. J Orthop Sports Phys Ther 2006;36:267-88. [Google Scholar] [PubMed]
- 12. Jain DK, Amaravati R, Sharma G. Evaluation of the clinical signs of anterior cruciate ligament and meniscal injuries. Indian J Orthop 2009;43:375-8. [Google Scholar] [PubMed]
- 13. Dzidzishvili L, Jackson GR, Allende F, Mameri ES, Allahabadi S, Chahla J. Meniscal radial tears repaired with all-inside and inside-out techniques result in improved clinical outcome scores, but inside-out repairs may be associated with higher failure rates clinically and on second-look arthroscopy: A systematic review. Arthroscopy 2024;41:1667-79. [Google Scholar] [PubMed]
- 14. Rodríguez-Roiz JM, Sastre-Solsona S, Popescu D, Montañana-Burillo J, Combalia-Aleu A. The relationship between ACL reconstruction and meniscal repair: Quality of life, sports return, and meniscal failure rate-2- to 12-year follow-up. J Orthop Surg Res 2020;15:361. [Google Scholar] [PubMed]
- 15. Arya A, Kumar SD, Rajkumar V, Sudhan SR. Comparison of anterior cruciate ligament reconstruction with and without concomitant meniscal repair: A prospective comparative study. J Med Sci Res 2023;11:315-22. [Google Scholar] [PubMed]
- 16. Pathak S, Bharadwaj A, Patil P, Raut S, Srikanth RV. Functional outcomes of arthroscopic combined anterior cruciate ligament reconstruction and meniscal repair: A retrospective analysis. Arthrosc Sports Med Rehabil 2020;2:e71-6. [Google Scholar] [PubMed]
- 17. Sarraj M, Coughlin RP, Solow M, Ekhtiari S, Simunovic N, Krych AJ, et al. Anterior cruciate ligament reconstruction with concomitant meniscal surgery: A systematic review and meta-analysis of outcomes. Knee Surg Sports Traumatol Arthrosc 2019;27:3441-52. Erratum in: Knee Surg Sports Traumatol Arthrosc 2019;27:3453. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient
March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient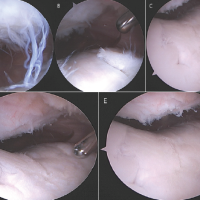 December 1, 2024 Patellofemoral Arthritis after Conservative Management for Post-operative Arthrofibrosis: A Case Report
December 1, 2024 Patellofemoral Arthritis after Conservative Management for Post-operative Arthrofibrosis: A Case Report March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study
March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study March 1, 2026 Functional Recovery after Arthroscopic Management of Meniscal Tears
March 1, 2026 Functional Recovery after Arthroscopic Management of Meniscal Tears