
Proximal rectus femoris avulsions can be treated successfully with surgery in high-level athletes and enable them to return to high-level play.
Dr. Christian E Athanasian, Department of Orthopedic Surgery, Columbia University, New York, United States. E-mail: athanasiance@gmail.com
Abstract
Introduction: Proximal rectus femoris avulsion injuries are uncommon injuries, and there is no consensus regarding the optimal management of these injuries among high-level athletes with a goal of returning to play at a high-level. This specifically has never been explored in athletes with demands specific to an American football offensive lineman.
Case Report: A 20-year-old male Division I collegiate offensive lineman sustained a right proximal rectus femoris avulsion in training camp before the season. The patient failed non-operative treatment with physical therapy and underwent proximal rectus femoris repair with suture anchors. One year later, the patient returned to full participation and completed the following season without injury.
Conclusion: Proximal rectus femoris avulsions can be treated successfully with surgery in high-level athletes and enable them to return to high-level play.
Keywords: Rectus femoris avulsion, collegiate athletics, suture anchor repair, football.
Proximal rectus femoris avulsions are uncommon, representing just 1.5% of hip lesions that occur during sports [1]. The rectus femoris is a biarticular muscle crossing both the hip and knee, predisposing it to injury. It is the most commonly injured muscle in the quadriceps muscle group. Proximal rectus femoris avulsion injuries tend to occur during hip hyperextension and knee flexion or rapid eccentric contraction, and they are more commonly reported in sports with high demand for sprinting and kicking. There is no consensus treatment for proximal rectus femoris tendon avulsions. Previous studies have demonstrated that non-operative treatment can be successful in high-level athletes [2,3,4,5]. However, in those cases in which athletes failed non-operative treatment, surgical intervention has also demonstrated excellent results, returning athletes back to a high-level of play [6,7,8,9,10,11,12,13,14]. There is no consensus of the optimal surgical technique, with direct suture repair [12], suture anchors [8,10,13,14], muscle-to-muscle suture repair [11], and tenodesis [9] all demonstrating successful return to sport. Only one study has compared outcomes between different surgical techniques, with Kayani et al. preferring primary tenodesis to surgical repair due to reduced time for return to pre-injury level and decreased risk of injury recurrence [9]. This case demonstrates successful surgical repair of a proximal rectus femoris avulsion in a Division I collegiate football player who had failed non-operative treatment. The patient was informed that data concerning the case would be submitted for publication, and he provided consent.
A 20-year-old male Division 1 college offensive lineman with no significant medical history or right hip problems presented with right hip pain after feeling a pop in his right hip while doing a squat. His exam was notable for tenderness over the right hip flexors. Plain radiographs of the hip and pelvis demonstrated femoroacetabular impingement syndrome (FAI) morphology with an alpha angle of 60° and a lateral center edge angle of 40° (Fig. 1).
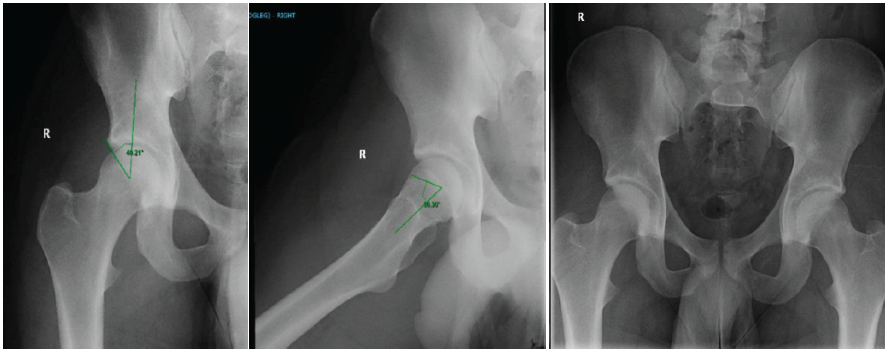
Figure 1: XR of right hip and pelvis demonstrating femoroacetabular impingement syndrome morphology.
He was initially managed conservatively with physical therapy conducted by the athletic training staff. He attempted to return to football-related activities and drills when his right hip buckled again (4 weeks after initial injury). In addition to tenderness over the right hip flexor, his exam demonstrated weakness in hip flexion and knee extension. A magnetic resonance imaging demonstrated a complete avulsion of the proximal rectus femoris direct and indirect heads with approximately 3 cm of retraction in addition to FAI with associated anterior superior labral tear, osteitis pubis, and adductor aponeurosis tear (Fig. 2).
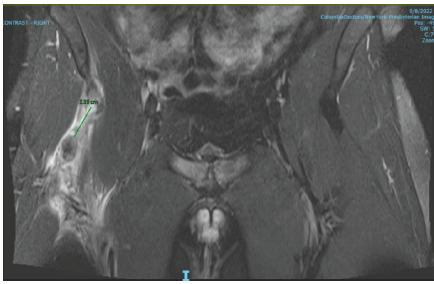
Figure 2: Coronal magnetic resonance imaging demonstrating complete avulsion of the proximal rectus femoris with approximately 3 cm of retraction.
To help distinguish between the rectus femoris avulsion and FAI as the source of his pain, a diagnostic intra-articular injection was performed with only 10–20% improvement in his pain suggesting FAI to be a minor contributor to his symptoms. Due to failure of conservative treatment and re-aggravation of his symptoms, surgical repair of the rectus femoris tendon was recommended.
The patient was positioned supine and underwent spinal and general anesthesia. Using the technique described by Dean et al., a 7 cm incision was made starting from 1 cm distal and 2 cm lateral to the anterior superior iliac spine toward the lateral border of the patella [16] (Fig. 3).
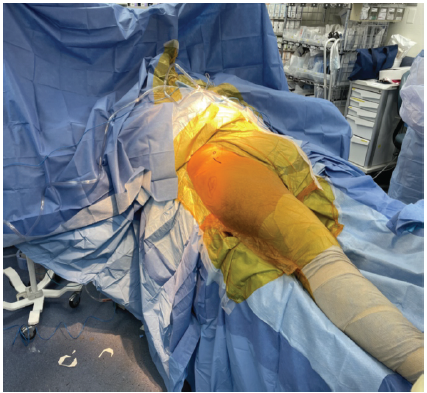
Figure 3: Patient positioned supine with the greater trochanter and anterior superior iliac spine marked.
Dissection was carried down through the superficial Smith-Peterson interval between sartorius and tensor fascia lata. The avulsed rectus femoris tendon was then visualized – it was retracted approximately 4cm with an associated seroma, and there were residual attachments of the indirect head to the superior acetabulum. The tendon was tagged with sutures and mobilized with blunt dissection (Fig. 4).
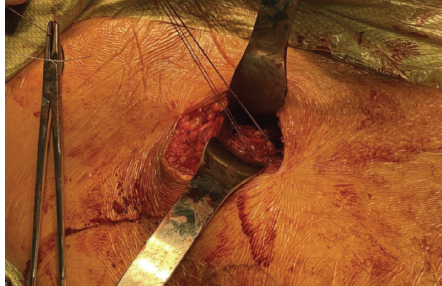
Figure 4: Avulsed rectus femoris tendon tagged with mobilizations sutures.
Next, fluoroscopy was used to identify the anterior inferior iliac spine (AIIS) and the AIIS footprint was prepared by removing residual fascial attachments and using a cobb elevator to create a bleeding bone surface. An obturator outlet view was utilized to confirm placement in the supracetabular bone and an iliac oblique view was used to direct anchors superior to the acetabulum. A 2.6 mm Fibertak (Arthrex) triple-loaded anchor was placed into the footprint with excellent fixation (Fig. 5), and a free needle was used to run 2 of the sutures through the tendon in a Krakow manner and the 3rd more distally as a rip-stop suture (Fig. 6).
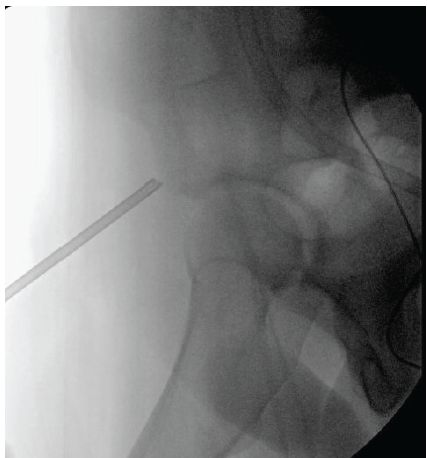
Figure 5: Intraoperative fluoroscopy showing insertion of 2.6 mm Fibertak directed into the anterior inferior iliac spine footprint.
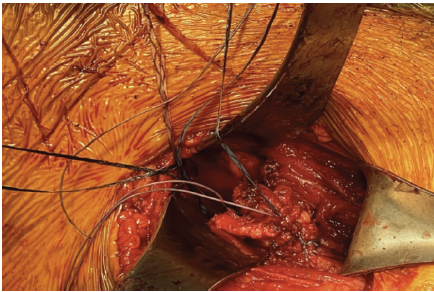
Figure 6: Avulsed rectus femoris tendon with 2 sutures from 2.6 mm Fibertak (placed in anterior inferior iliac spine footprint) run in Krakow manner.
These sutures were left untied, and fluoroscopy was again used to identify a more lateral site in the supra-acetabular bone for a 4.75 mm Swivelock (Arthrex), which was drilled and tapped. A bump was placed under the knee to aid in the reduction of the tendon to the footprint. The tendon was reduced to the footprint using the two Krakow sutures in a pulley fashion. These sutures were then tied, followed by the rip-stop suture. All of these sutures were then passed through the Swivelock anchor, which was then inserted into the previously prepared site (Fig. 7). Before closure, the bump was removed and the repair inspected – the leg was able to lay flat on the operating table without significant tension nor gapping.
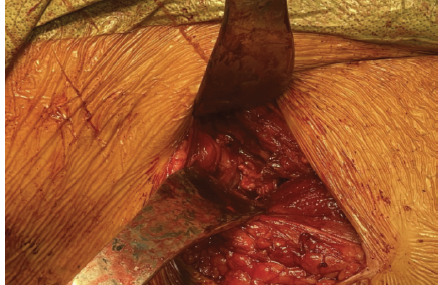
Figure 7: Final repair showing reattachment of the avulsed rectus femoris tendon to the anterior inferior iliac spine.
Post-operatively, the patient was placed in a hinged knee brace locked in extension and maintained flat foot weight-bearing for 6 weeks, followed by progressive weight bearing out of the brace. Beginning post-operative day 1, he used a continuous passive motion machine from 0 to 90° for 2 h/day to maintain his knee range of motion. At his initial post-operative visit 2 weeks after surgery, he reported decreased sensation in the lateral femoral cutaneous nerve distribution, which progressively improved. At 6-months post-operatively, the patient had returned to spring football practice, and at 1-year post-operatively, the patient had returned to full activity playing Division 1 college football as an offensive lineman without reinjury or recurrent symptoms.
Complete rupture of the proximal rectus femoris is uncommon. It occurs more frequently in sports with high-level demands of sprinting and kicking [15]. In this case, we utilized the surgical technique demonstrated by Dean et al. to repair the direct head of the rectus femoris to the AIIS [16]. Dean et al. suggested that surgical repair is indicated in high-level athletes with significant demands on explosive hip flexion, and athletes who had failed non-operative treatment for at least 3 months with continued pain or weakness. Our patient had failed non-operative treatment for 6 weeks and was left unable to participate in Division I football. After surgical repair, he was able to return to full-participation without reinjury or recurrent symptoms. A 2023 systematic review by Knapik et al., including 132 competitive athletes with full-thickness proximal rectus femoris injuries, found that these injuries occurred most frequently in soccer (70.5%) and rugby (15.2%). The most common mechanisms of injury for these athletes were kicking (47.6%) and excessive knee flexion with forced hip extension (42.9%). Non-operative treatment was utilized in 19.7% of these athletes, with a return to play rate of 93.3% and a mean return to play time of 11.7 weeks. Operative treatment was utilized in 80.3% of these athletes, with a return to play rate of 100%, with a mean return to play time of 22.1 weeks [15]. The largest case-series of non-operative cases to date in high-level athletes by Gamradt et al. followed 11 NFL players, all of which demonstrated successful return to play within 6–12 weeks, with one player even making it to the Pro-Bowl [3]. The largest case-series involving operative treatment in high-level athletes was conducted by Lempainen et al. comprising 18 professional soccer players, one of which had bilateral tears. All players returned to the same-level of play, with some players returning to play in as little as 3 months. However, they did note that two players had a loss of sensation due to injury to the lateral femoral cutaneous nerve branches, which did not interfere with their function [10]. Based on the literature regarding proximal rectus femoris avulsions in high-level athletes and our specific patient’s case, we opted to treat our patient with surgical repair after initially failing an attempt at conservative management. Moreover, we believed this would allow our patient a better chance at not only returning to the same level of play, but also at a similar level to his pre-injury performance. Straw et al. found that a semiprofessional soccer player with a proximal rectus femoris rupture who had failed non-operative treatment for 12 months demonstrated only 66% of concentric quadriceps strength compared to the uninjured leg. Upon completion of rehabilitation for surgical repair, the patient’s concentric quadriceps strength returned to nearly normal, and was able to return to play 6 months post-operatively [12]. Across surgical repair, we believe we provided our patient the best opportunity to regain maximal strength and function, which was necessary to return to his sport as an offensive lineman. At 1-year follow-up, he was able to return to Division I football. Therefore, we believe that surgical repair of proximal rectus femoris avulsions is an excellent option for high-level athletes who have failed non-operative treatment. Limitations of our case include a lack of pre-operative and post-operative quantifiable measures of patient function and athletic performance. Therefore, while we are able to comment on this surgical technique’s ability to return athletes to the same level of competition, we are unable to comment on it’s ability to return athletes to the same level of on the field performance and function.
Proximal rectus femoris avulsions can be treated successfully with surgery in high-level athletes and enable them to return to high-level play. Specifically, power-based athletes, such as American football offensive lineman can succeed with this specific surgical intervention.
Proximal rectus femoris avulsions can be treated successfully with surgery in high-level athletes and enable them to return to high-level play.
References
- 1. References [Google Scholar] [PubMed]
- 2. Kannus P, Natri A. Etiology and pathophysiology of tendon ruptures in sports. Scand J Med Sci Sports 1997;7:107-12. [Google Scholar] [PubMed]
- 3. Esser S, Jantz D, Hurdle MF, Taylor W. Proximal rectus femoris avulsion: Ultrasonic diagnosis and nonoperative management. J Athl Train 2015;50:778-80. [Google Scholar] [PubMed]
- 4. Gamradt SC, Brophy RH, Barnes R, Warren RF, Byrd JW, Kelly BT. Nonoperative treatment for proximal avulsion of the rectus femoris in professional American football. Am J Sports Med 2009;37:1370-4. [Google Scholar] [PubMed]
- 5. Hsu JC, Fischer DA, Wright RW. Proximal rectus femoris avulsions in national football league kickers: A report of 2 cases. Am J Sports Med 2005;33:1085-7. [Google Scholar] [PubMed]
- 6. Olmo J, Aramberri M, Almaraz C, Nayler J, Requena B. Successful conservative treatment for a subtotal proximal avulsion of the rectus femoris in an elite soccer player. Phys Ther Sport 2018;33:62-9. [Google Scholar] [PubMed]
- 7. García VV, Duhrkop DC, Seijas R, Ares O, Cugat R. Surgical treatment of proximal ruptures of the rectus femoris in professional soccer players. Arch Orthop Trauma Surg 2012;132:329-33. [Google Scholar] [PubMed]
- 8. Huri G, Dubin JM, Ozgonen K, Kaya D, Doral MN. A unique rectus femoris injury in an adolescent professional soccer player: A case report. JBJS Case Connect 2014;4:e115. [Google Scholar] [PubMed]
- 9. Irmola T, Heikkilä JT, Orava S, Sarimo J. Total proximal tendon avulsion of the rectus femoris muscle. Scand J Med Sci Sports 2007;17:378-82. [Google Scholar] [PubMed]
- 10. Kayani B, Singh S, Chang JS, Magan AA, Plastow R, Haddad FS. Outcomes of surgical repair versus primary tenodesis for proximal rectus femoris avulsion injuries in professional athletes. Am J Sports Med 2021;49:121-9. [Google Scholar] [PubMed]
- 11. Lempainen L, Kosola J, Pruna R, Puigdellivol J, Ranne J, Orava S. Operative treatment of proximal rectus femoris injuries in professional soccer players: A series of 19 cases. Orthop J Sports Med 2018;6:2325967118798827. [Google Scholar] [PubMed]
- 12. Sonnery-Cottet B, Barbosa NC, Tuteja S, Gardon R, Daggett M, Monnot D, et al. Surgical management of rectus femoris avulsion among professional soccer players. Orthop J Sports Med 2017;5:2325967116683940. [Google Scholar] [PubMed]
- 13. Straw R, Colclough K, Geutjens G. Surgical repair of a chronic rupture of the rectus femoris muscle at the proximal musculotendinous junction in a soccer player. Br J Sports Med 2003;37:182-4. [Google Scholar] [PubMed]
- 14. Ueblacker P, Müller-Wohlfahrt HW, Hinterwimmer S, Imhoff AB, Feucht MJ. Suture anchor repair of proximal rectus femoris avulsions in elite football players. Knee Surg Sports Traumatol Arthrosc 2015;23:2590-4. [Google Scholar] [PubMed]
- 15. Noble-Taylor K, Price M, McInnis K. Proximal rectus femoris tendon tear in a professional football placekicker: A case report. Curr Sports Med Rep 2023;22:187-90. [Google Scholar] [PubMed]
- 16. Knapik DM, Alter TD, Ganapathy A, Smith MV, Brophy RH, Matava MJ. Isolated, full-thickness proximal rectus femoris injury in competitive athletes: A systematic review of injury characteristics and return to play. Orthop J Sports Med 2023;11:23259671221144984. [Google Scholar] [PubMed]
- 17. Dean CS, Arbeloa-Gutierrez L, Chahla J, Pascual-Garrido C. Proximal rectus femoris avulsion repair. Arthrosc Tech 2016;5:e545-9. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Profile of Sports Injuries: Retrospective Analysis from a Single Centre
July 1, 2026 Profile of Sports Injuries: Retrospective Analysis from a Single Centre December 10, 2022 Osteomyelitis of the Pubis Treated by Masquelet Technique in a Football Player: A Case Report
December 10, 2022 Osteomyelitis of the Pubis Treated by Masquelet Technique in a Football Player: A Case Report April 1, 2025 Intra-Ligamentous Pigmented Villonodular Synovitis of the Anterior Cruciate Ligament, a Case Report
April 1, 2025 Intra-Ligamentous Pigmented Villonodular Synovitis of the Anterior Cruciate Ligament, a Case Report March 2, 2019 Para-articular Osteochondroma of Patella with Coexisting Osteoarthritis
March 2, 2019 Para-articular Osteochondroma of Patella with Coexisting Osteoarthritis