
Osteoporotic vertebral fractures are highly prevalent among postmenopausal women and are independently associated with advanced age, prolonged duration since menopause, low BMI, reduced lumbar spine bone mineral density, vitamin D deficiency, and prior fragility fractures.
Dr. Nayan Silawat, Department of Orthopaedics, Sundarlal Patwa Government Medical College, Mandsaur, Madhya Pradesh, India. E-mail: drnayansilawat@gmail.com
Abstract
Introduction: Underdiagnosed osteoporotic vertebral fractures are a major cause of morbidity in postmenopausal women. For prompt intervention and prevention, early detection of clinical, metabolic, and densitometric risk factors is essential. The purpose of this study was to ascertain the frequency of vertebral fractures and the risk factors that are linked to them in a group of postmenopausal women.
Materials and Methods: 220 postmenopausal women participated in a cross-sectional study conducted in a hospital. We gathered information on body mass index (BMI), previous fragility fractures, lifestyle factors, demographics, reproductive history, and serum vitamin D levels. Dual-energy X-ray absorptiometry was used to measure the bone mineral density (BMD) at the femoral neck and lumbar spine. Lateral thoracolumbar radiographs were used to assess vertebral fractures, which were then graded using a standardized semiquantitative method. Women with and without vertebral fractures were compared, and independent predictors were found using multivariate logistic regression.
Results: The participants’ average age was 61.8 ± 8.4 years. 76 women (34.5%) had vertebral fractures, which were classified as mild in 15.5%, moderate in 11.8%, and severe in 7.3%. 44.5% had osteoporosis of the lumbar spine. Significantly older, longer postmenopausal duration, lower BMI, lower lumbar spine T-scores, higher rates of vitamin D deficiency, increased physical inactivity, and more frequent fragility fractures were all present in women with vertebral fractures (all P < 0.01). Age ≥65 years, time since menopause ≥15 years, BMI <20 kg/m2, lumbar spine osteoporosis, vitamin D deficiency, and previous fragility fractures were found to be independent predictors of vertebral fractures by multivariate analysis.
Conclusion: Osteoporotic vertebral fractures are common in postmenopausal women and are closely associated with advanced age, prolonged menopause, low BMI, decreased lumbar spine BMD, vitamin D deficiency, and prior fragility fractures. A thorough evaluation of risk factors beyond BMD is necessary for early detection and preventive measures.
Keywords: Postmenopausal women, osteoporosis, vertebral fractures, bone mineral density, vitamin D deficiency.
Reduced bone mass and disruption of bone microarchitecture are hallmarks of osteoporosis, a generalized skeletal disorder that increases susceptibility to fragility fractures. Because of the sudden drop in estrogen levels following menopause, this condition is particularly common in postmenopausal women [1]. Vertebral fractures are the most common type of osteoporotic fractures and are linked to significant clinical outcomes, such as chronic pain, diminished physical function, a lower quality of life, and an increased risk of death [2]. Notably, women whose bone mineral density (BMD) does not fall within the osteoporotic range may still experience vertebral fractures, highlighting the fact that factors other than BMD also affect fracture risk [3]. One well-known, unchangeable factor influencing the risk of vertebral fractures is getting older. The incidence of vertebral fractures rises sharply with age, according to epidemiological data, which is consistent with progressive age-related bone loss and deteriorating bone strength [4]. In addition, a longer time since menopause has been associated with an increased risk of vertebral fractures, probably as a result of the cumulative effects of long-term estrogen deficiency on skeletal integrity and bone remodeling [1,3]. Low BMD is still a major predictor of fracture risk, despite the fact that many other factors also play a role. Reduced BMD at the hip and spine is strongly linked to a higher risk of osteoporotic fractures, including vertebral fractures, according to population-based studies [1,4]. Furthermore, a number of clinical and lifestyle factors have been found to be significant contributors in postmenopausal women, such as low body mass index (BMI), little physical activity, and vitamin D deficiency. Inadequate vitamin D reduces calcium metabolism and may hasten bone loss, both of which raise the risk of fracture [5,6]. Low BMI is linked to less mechanical loading on bone. Because it indicates underlying skeletal fragility and cumulative fracture risk, a history of previous fragility fractures is also a strong predictor of future vertebral fractures [3]. Considering the multifactorial etiology of osteoporotic vertebral fractures, comprehensive evaluation of both modifiable and non-modifiable risk factors is essential for effective prevention and clinical management in postmenopausal women. Although several studies have explored osteoporosis-related risk factors, vertebral fractures often remain clinically silent and underdiagnosed, particularly when assessment relies solely on BMD. In addition, data on radiographically detected vertebral fractures and their association with clinical, metabolic, and lifestyle factors in Indian postmenopausal women are limited. Therefore, this study was conducted to estimate the prevalence of vertebral fractures and to evaluate the demographic, clinical, and lifestyle determinants associated with fracture risk in this population, with the aim of enhancing risk stratification beyond BMD alone.
Ethical considerations
The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. All clinical, radiological, and laboratory investigations performed for the purpose of the study were provided free of cost to the participants, and no additional expenses were borne by them.
Study design and setting
This research was a cross-sectional observational study conducted at a tertiary care teaching hospital in India.
Study population
Postmenopausal women visiting the outpatient and inpatient orthopedic departments during the study period were evaluated for their eligibility. Postmenopause was characterized by the lack of menstrual periods for at least 12 continuous months, which is not due to any pathological or physiological factors apart from menopause.
Sample size estimation
The sample size was calculated based on previously documented prevalence rates of osteoporotic vertebral fractures in postmenopausal women from Indian and other Asian demographics, which vary from 20% to 30%. With an anticipated prevalence of 25% [7], a 95% confidence level, and an absolute precision of 6%, the required minimum sample size came out to be 200 participants. To account for potential non-response or incomplete data, a total of 220 postmenopausal women were recruited using a consecutive sampling method.
Inclusion criteria
- Women who’re past menopause and are 45 years or older
- Provision of informed written consent
- Willingness to undergo clinical, radiological, and laboratory evaluation.
Exclusion criteria
- History of high-energy spinal trauma
- Presence of secondary causes of osteoporosis, including chronic kidney disease, hyperthyroidism, Cushing’s syndrome, or malignancy
- Long-term use of medications known to influence bone metabolism, such as systemic corticosteroids, anticonvulsants, bisphosphonates, or hormone replacement therapy within the preceding year
- History of spinal surgery or congenital spinal abnormalities.
Data collection
Demographic, clinical, and lifestyle-related data were systematically gathered utilizing a pre-established structured pro forma. The variables documented encompassed age, duration post-menopause, BMI, parity, age at which menopause occurred, prior fragility fractures, familial predisposition to osteoporosis, tobacco use, alcohol consumption, levels of physical activity, and dietary calcium intake. Anthropometric evaluations were conducted in accordance with standardized protocols. The BMI was computed as weight (kg) divided by the square of height (m2) and classified in alignment with the guidelines provided by the World Health Organization.
Assessment of BMD
BMD was assessed using dual-energy X-ray absorptiometry (DEXA) at the lumbar spine (L1-L4) and femoral neck. Results were expressed as T-scores and categorized as normal, osteopenia, or osteoporosis based on established diagnostic criteria.
Radiological assessment of vertebral fractures
It was carried out through lateral radiographs of the thoracic and lumbar spine for all participants. Vertebral fractures were detected and categorized utilizing a standardized semiquantitative approach predicated on the reductions observed in vertebral height. The fractures were classified as mild, moderate, or severe, contingent upon the degree of loss in anterior, middle, or posterior height. All radiographic evaluations were executed independently by a seasoned radiologist who remained blinded to both clinical and BMD findings.
Laboratory investigations
Baseline biochemical evaluations included serum calcium, phosphate, alkaline phosphatase, and 25-hydroxyvitamin D levels to assess bone metabolic status and to rule out secondary causes of bone loss.
Outcome measures
The primary outcome was the existence of osteoporotic vertebral fractures. Among the key explanatory variables included age, duration since menopause, BMI, BMD, Vitamin D status, lifestyle factors, and reproductive characteristics.
Statistical analysis
The data were entered and analyzed using standard statistical software. Continuous variables were summed as the mean and standard deviation, while categorical variables were expressed as frequencies and percentages. Comparison of participants with and without vertebral fractures was analyzed using the independent t-test for continuous variables and the Chi-square test for categorical variables. After adjustment for potential confounding factors multivariate logistic regression analysis was performed to identify independent predictors of osteoporotic vertebral fractures. A statistically significant P-value was considered 0.05.
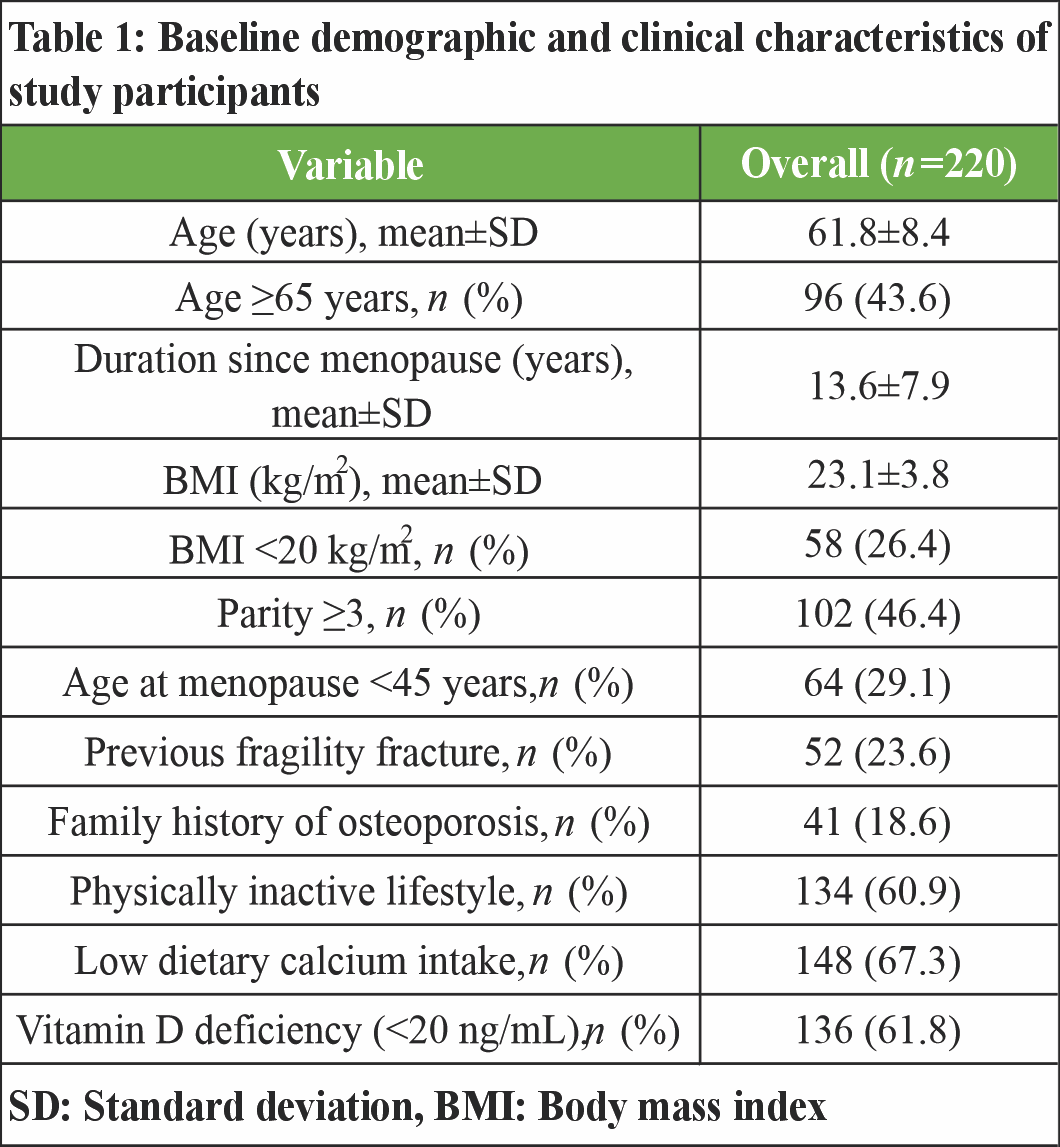
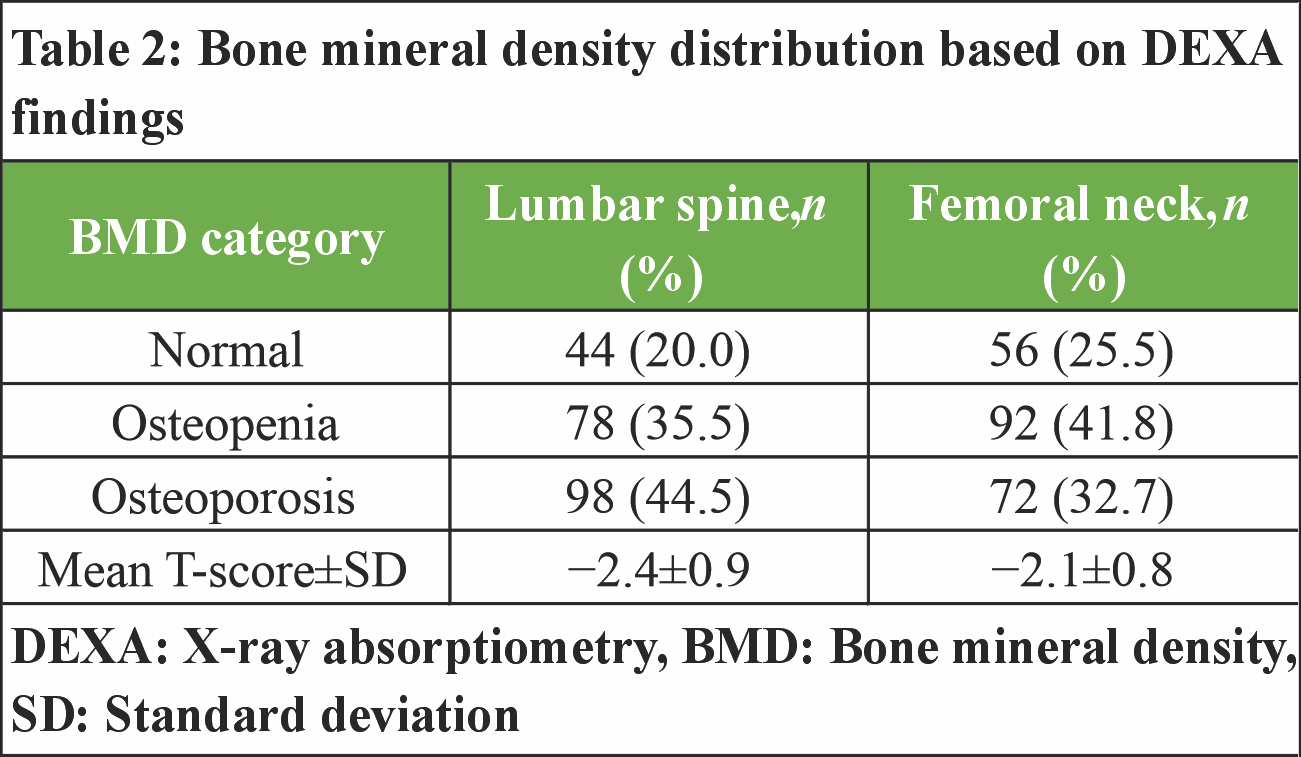
A total of 220 postmenopausal women were analyzed (Table 1). The mean age was 61.8 ± 8.4 years, and 43.6% were aged 65 years or older. The average time since menopause was 13.6 ± 7.9 years, while the mean BMI was 23.1 ± 3.8 kg/m2. Low BMI (<20 kg/m2) was observed in 26.4% of participants. A sedentary lifestyle was reported by 60.9% of women, and 67.3% had low dietary calcium intake. Vitamin D deficiency was identified in 61.8% of the study population. In addition, 23.6% reported a prior fragility fracture, and 18.6% had a family history of osteoporosis. Based on DEXA findings, osteoporosis at the lumbar spine was present in 44.5% of participants, while 35.5% had osteopenia and 20.0% had normal BMD. At the femoral neck, 32.7% were classified as osteoporotic, 41.8% as osteopenic, and 25.5% had normal bone density. The mean T-scores were −2.4 ± 0.9 at the lumbar spine and −2.1 ± 0.8 at the femoral neck (Table 2).
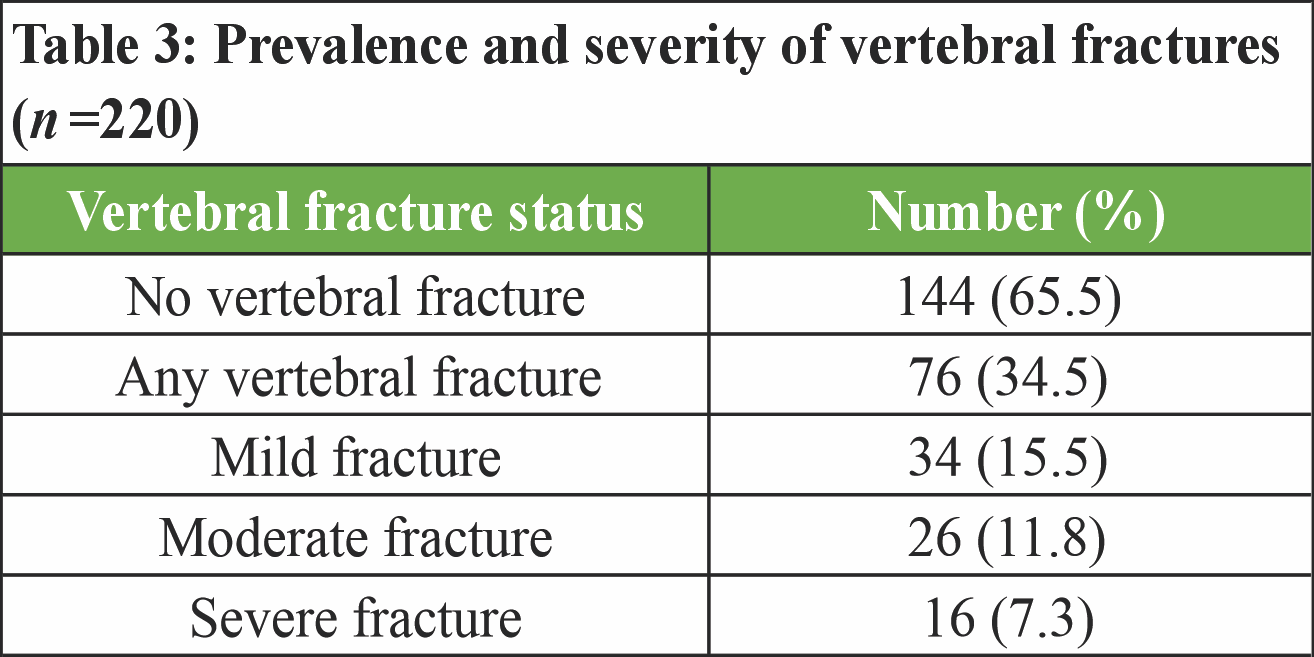
 Radiographic assessment demonstrated that 76 women (34.5%) had at least one vertebral fracture. Of these, 15.5% were classified as mild, 11.8% as moderate, and 7.3% as severe fractures. The remaining 65.5% of participants showed no radiological evidence of vertebral fracture (Table 3).
Radiographic assessment demonstrated that 76 women (34.5%) had at least one vertebral fracture. Of these, 15.5% were classified as mild, 11.8% as moderate, and 7.3% as severe fractures. The remaining 65.5% of participants showed no radiological evidence of vertebral fracture (Table 3).
Participants with vertebral fractures were significantly older than those without fractures (66.2 ± 7.5 vs. 59.4 ± 8.1 years; P < 0.001) and had a longer duration since menopause (17.8 ± 6.9 vs. 11.3 ± 7.4 years; P < 0.001). Mean BMI was significantly lower in the fracture group (21.4 ± 3.2 kg/m2) compared with the non-fracture group (24.0 ± 3.7 kg/m2; P < 0.001). Lumbar spine BMD was also substantially reduced among women with fractures, with a mean T-score of −3.0 ± 0.7 versus −2.0 ± 0.8 in those without fractures (P < 0.001) (Table 4).
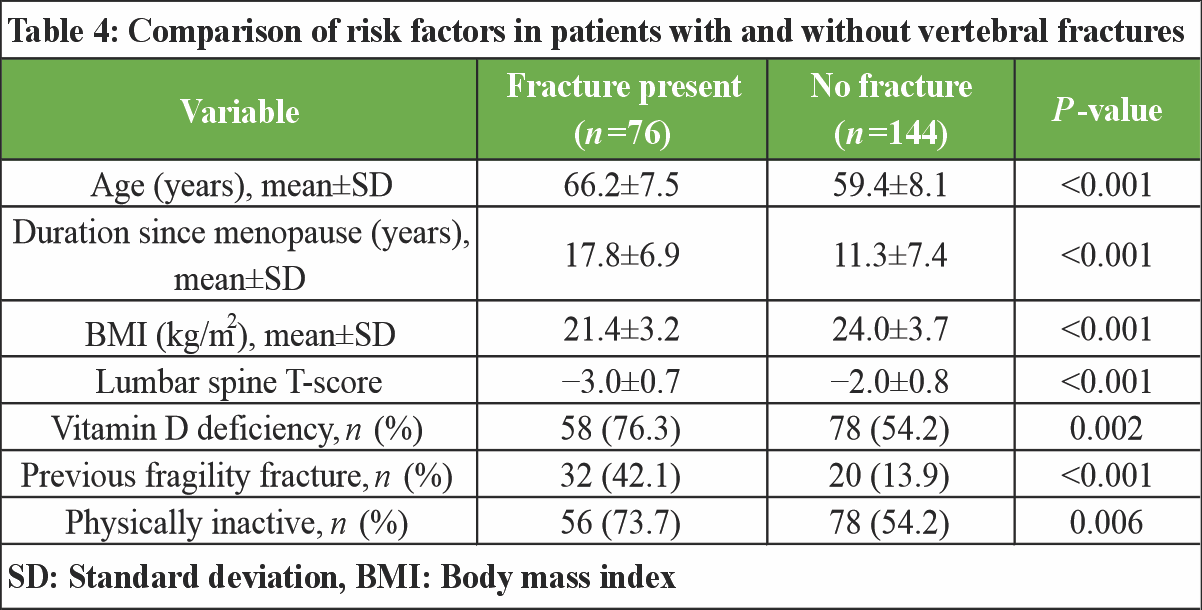
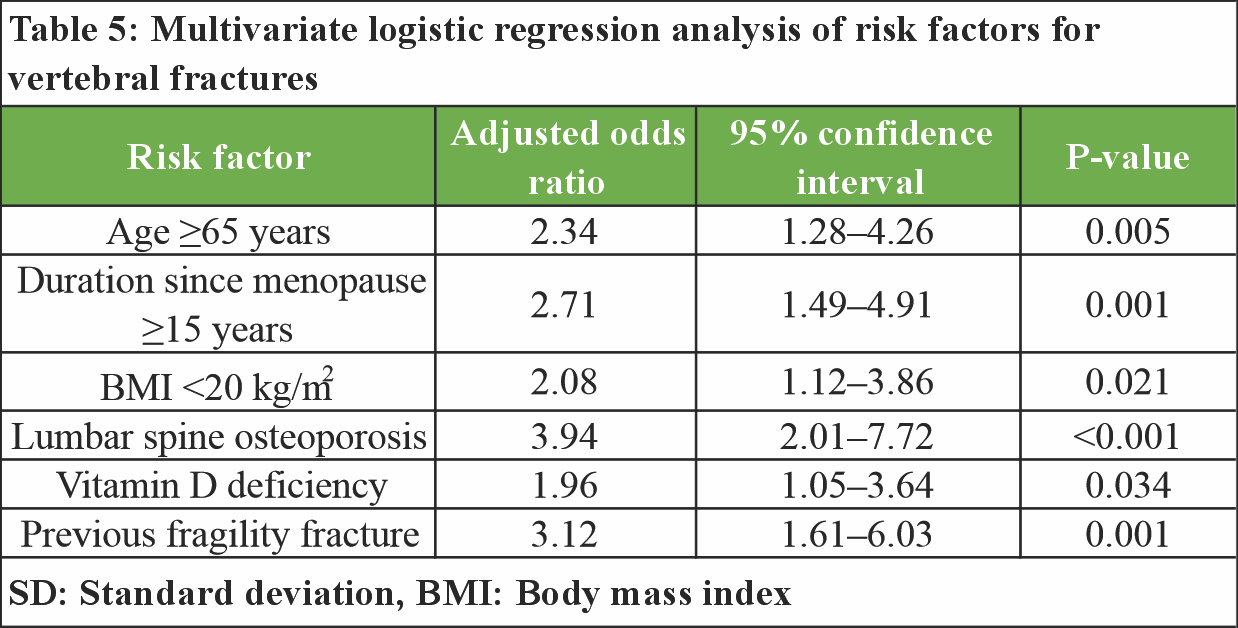
Vitamin D deficiency was more prevalent among women with vertebral fractures than among those without fractures (76.3% vs. 54.2%; P = 0.002). A history of prior fragility fracture was strongly associated with present vertebral fractures (42.1% vs. 13.9%; P < 0.001). Physical inactivity was also more common in the fracture group (73.7%) compared to the non-fracture group (54.2%; P = 0.006) (Table 4). Multivariate logistic regression analysis identified several independent predictors of vertebral fractures, including age ≥65 years (adjusted odds ratio [AOR] 2.34; 95% confidence interval [CI]: 1.28–4.26), duration since menopause ≥15 years (AOR 2.71; 95% CI: 1.49–4.91), BMI <20 kg/m2 (AOR 2.08; 95% CI: 1.12–3.86), and lumbar spine osteoporosis (AOR 3.94; 95% CI: 2.01–7.72). Vitamin D deficiency (AOR 1.96; 95% CI: 1.05–3.64) and a previous fragility fracture (AOR 3.12; 95% CI: 1.61–6.03) remained significantly associated with vertebral fractures after adjustment for potential confounders (Table 5).
Vertebral fractures were also identified to be considerably linked to advanced age, decreased BMI, extended postmenopausal years, reduced bone mineral level, vitamin D lack, and old history of fragility fractures in the present cross-sectional study of postmenopausal women. The latter findings are consistent with currently available epidemiological data that show that the risk of fracture increases with age due to the cumulative effect of bone loss and worsening bone microarchitecture. Age has always been an effective predictor of vertebral fractures in postmenopausal women, and meta-analyses have demonstrated that age is independently contributing to the risk of fractures in postmenopausal women [8]. The correlation between the BMI and vertebral fractures seems to be multifactorial. Past research indicates that both underweight and overweight bone mass index can have a different effect on the risk of fracture based on skeletal location and demographic. Although there are a few meta-analyses that have reported that obese postmenopausal women are at increased risk of skeletal fragility due to higher adiposity, other cross-sectional studies have also indicated that low BMI and lean and fat mass depletion are both related to the increased risk of vertebral fractures [9,10]. The findings indicate that, poor mechanical loading, body composition changes, as well as bone quality changes may all contribute to higher levels of fracture risk. Vitamin D deficiency has now become a significant and possibly alterable risk factor of vertebral fractures. Reduced serum levels of 25-hydroxyvitamin D have been negatively related with the likelihood and the morbidity of vertebral fractures despite controlling by BMD and other confounders [11,12]. Since vitamin D plays a vital role in the body, especially when it comes to taking in calcium and bone mineralization, as well as bone remodeling, deficiency can further decrease skeletal fragility and weaken the vertebrae in postmenopausal women. Estrogen deficiency causes also contribute to the risk of fractures as well as the length of estrogen deficiency after menopause. The longer postmenopausal period is linked with continuous high bone turnover and rapid loss of trabecular bone, which preferentially impacts on vertebral integrity. This observation is in line with experimental and clinical studies that have revealed the negative impact of chronic estrogen deficiency on bone remodeling and fracture vulnerability [13,14]. Furthermore, a history of fragility fracture in the past is a good indicator of vertebral fracture in the future, as it is a reflection of systemic skeletal weakness and a combination of numerous risk factors [13]. Although the BMD is still a major predictor of fracture, the present results emphasize the need to take a wider scope of clinical and lifestyle risk factors into consideration. Combining age, body composition, Vitamin D status and fracture history with BMD measurement would facilitate a better risk stratification and thereby facilitate more effective prevention and management measures of vertebral fracture in postmenopausal women.
This cross-sectional review shows that osteoporotic vertebral fractures are a clinically important and common issue in postmenopausal women. The analysis revealed that increasing age, prolonged post menopause duration, low BMI, and low lumbar spine BMD were the most relevant independent risk factors of vertebral fractures. Further, the lack of vitamin D and the previous fragility fracture were linked to the high risk of fracture, which is the joint effect of the metabolic and clinical factors on skeletal fragility. The findings highlight the importance of early identification of women at high risk by conducting proper clinical examination, bone density testing, and addressing the modifiable factors, such as low BMI, sedentary living, and vitamin D deficiency. Routine screening and specific preventive measures could be used to reduce occurrence and morbidity of vertebral fractures in this vulnerable population.
A substantial proportion of postmenopausal women harbor vertebral fractures that may remain clinically unrecognized. Reliance on BMD alone is insufficient, as multiple clinical and metabolic factors significantly influence fracture risk. Comprehensive risk assessment incorporating age, menopausal duration, BMI, vitamin D status, and history of fragility fractures is essential for early identification of high-risk individuals. Timely screening and correction of modifiable risk factors can play a pivotal role in reducing fracture burden and related morbidity in this population.
References
- 1. Dimai HP, Fahrleitner-Pammer A. Osteoporosis and fragility fractures: Currently available pharmacological options and future directions. Best Pract Res Clin Rheumatol 2022;36:101780. [Google Scholar] [PubMed]
- 2. Khan AA, Slart RH, Ali DS, Bock O, Carey JJ, Camacho P, et al. Osteoporotic fractures: Diagnosis, evaluation, and significance from the international working group on DXA best practices. Mayo Clin Proc 2024;99:1127-41. [Google Scholar] [PubMed]
- 3. Smit AE, Meijer OC, Winter EM. The multi-faceted nature of age-associated osteoporosis. Bone Rep 2024;20:101750. [Google Scholar] [PubMed]
- 4. Hsu SH, Chen LR, Chen KH. Primary osteoporosis induced by androgen and estrogen deficiency: The molecular and cellular perspective on pathophysiological mechanisms and treatments. Int J Mol Sci 2024;25:12139. [Google Scholar] [PubMed]
- 5. Liu H, Li B, Liu L, Ying W, Rosen CJ. Weight loss induced bone loss: Mechanism of action and clinical implications. Bone Res 2025;13:99. [Google Scholar] [PubMed]
- 6. Rinonapoli G, Pace V, Ruggiero C, Ceccarini P, Bisaccia M, Meccariello L, et al. Obesity and bone: A complex relationship. Int J Mol Sci 2021;22:13662. [Google Scholar] [PubMed]
- 7. Sunder A, Chhabra HS, Aryal A. Geriatric spine fractures – demography, changing trends, challenges and special considerations: A narrative review. J Clin Orthop Trauma 2023;43:102190. [Google Scholar] [PubMed]
- 8. Shieh A, Ruppert KM, Greendale GA, Lian Y, Cauley JA, Burnett-Bowie SA, et al. Associations of age at menopause with postmenopausal bone mineral density and fracture risk in women. J Clin Endocrinol Metab 2022;107:e561-9. [Google Scholar] [PubMed]
- 9. Liu HF, Meng DF, Yu P, De JC, Li HY. Obesity and risk of fracture in postmenopausal women: A meta-analysis of cohort studies. Ann Med 2023;55:2203515. [Google Scholar] [PubMed]
- 10. Palermo A, Tuccinardi D, Defeudis G, Watanabe M, D’Onofrio L, Lauria Pantano A, et al. BMI and BMD: The potential interplay between obesity and bone fragility. Int J Environ Res Public Health 2016;13:544. [Google Scholar] [PubMed]
- 11. Fitzpatrick D, Laird E, Ward M, Hoey L, Hughes CF, Strain JJ, et al. Secondary hyperparathyroidism: Predictors and relationship with vitamin D status, bone turnover markers and bone mineral density. Bone 2024;184:117108. [Google Scholar] [PubMed]
- 12. Wang N, Chen Y, Ji J, Chang J, Yu S, Yu B. The relationship between serum vitamin D and fracture risk in the elderly: A meta-analysis. J Orthop Surg Res 2020;15:81. [Google Scholar] [PubMed]
- 13. Wang C, Fu R, Yang H. Toward a clear relationship between mechanical signals and bone adaptation. Mechanobiol Med 2025;3:100115. [Google Scholar] [PubMed]
- 14. Shi V, Morgan EF. Estrogen and estrogen receptors mediate the mechanobiology of bone disease and repair. Bone 2024;188:117220. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study
July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density
June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery
July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone
July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone