
Deformed patella shape can be seen in X-rays after primary open repair after an acute traumatic quadriceps rupture, if we take direct stitches in the patella during repair.
Dr. Soumya Paik, Department of Paediatric Orthopedics, KIDS Orthopedic Clinic, Property No. DGK 110, DLF Galleria, Premises- 02-0124, Plot No. BG/8, AA - 1B, Major Arterial Road, Action Area 1, Newtown, North 24 Parganas, Kolkata-700156, West Bengal, India. E-mail: drsoumyapaik@gmail.com
Abstract
Introduction: Adolescent quadriceps rupture is a rare entity, that’s why there is a paucity of literature regarding it. In this study, we showcased a case of adolescent traumatic quadriceps rupture treated with open repair with a long follow-up.
Case Report: Traumatic quadriceps rupture is very rare in adolescents. A 14-year-old male child suffered an acute trauma over left knee and was presented with imaging (magnetic resonance imaging) showing a traumatic quadriceps rupture. Primary open repair (bone to tendon) done with high tensile non-absorbable suture. Full range of motion returned, and the patient is living a normal life within a year. Age of the patient, type of rupture, and treatment modality in our case make it unique.
Conclusion: Primary open quadriceps repair can give good knee function if treated early and efficiently, even in adolescents.
Keywords: Quadriceps tear, primary open repair, extensor mechanism, adolescent quadriceps tear
Adolescent acute traumatic quadriceps rupture is of extremely rare occurrence. Quadriceps tendon ruptures (QTRs) are relatively uncommon injuries (1.37/100,000) that usually present in middle aged and elderly men with a history of chronic illness, such as diabetes, renal failure, gout, rheumatoid arthritis, or hyperparathyroidism [1]. QTRs in children and adolescents are exceedingly rare injuries, with sparse literature reporting findings within this patient population [1]. Most of the literature talks about adult quadriceps rupture and the treatment modality regarding this. It can be of two types: Partial and complete tear. Treatment options depend on the severity: Partial tears may be managed conservatively, while complete ruptures with extensor mechanism disruption typically require surgical repair [2]. Magnetic resonance imaging (MRI) is the preferred diagnostic tool, especially when there is uncertainty, as it helps distinguish between partial and complete tears [2]. This imaging modality is essential in confirming the diagnosis and guiding treatment decisions. The diagnosis of quadriceps rupture in adolescents can be challenging due to its rarity, and a timely diagnosis is essential for appropriate treatment and optimal clinical outcomes. In this article, we will be presenting a case of adolescent traumatic quadriceps rupture managed by primary open repair at our institution. The caregivers of the patient were informed that data concerning the case would be submitted for publication, and they provided consent.
A 14-year-old male patient with a body weight of 30 kg came to our department with left knee pain after an alleged history of trauma while playing football 2 days back. On clinical examination, pain over the left knee was encountered, there was a palpable gap over the left patella, and the patient could not do active straight leg raising. After doing a proper investigation, it was seen in the MRI that the quadriceps of the left side are completely ruptured and got erased from the patellar surface (Fig. 1).
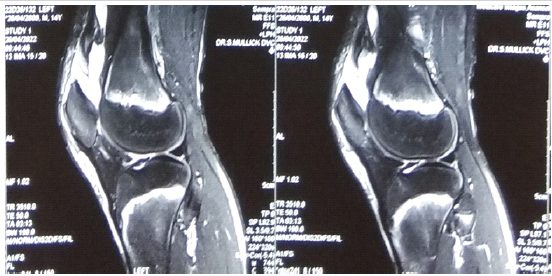
Figure 1: Pre-operative magnetic resonance imaging of the patient showing quadriceps tear.
After proper evaluation, the patient was planned for primary open repair of the quadriceps tendon by high-tensile non-absorbable suture (Ethibond No.5). A midline knee incision was made with tourniquet support, followed by meticulous soft-tissue dissection. It was seen intraoperatively that complete rupture of quadriceps from the upper pole of patella (Fig. 2A and B). The distal part of the tendon was resurfaced, and three Krakow stitches were taken over the tendon from proximal to distal direction (Fig. 3). Tendon was then pulled distally towards patella with the three ends of krackow stitches. There was no distal stump of the quadriceps left. Hence, we decided to stitch it directly to the upper pole of the patella with osseous stitches taken through the patella itself (Fig. 4). While stitching and tightening the sutures, we kept the knee in full extension. Intraoperative range of motion was checked, which was 0–100°. The wound was closed in layers.
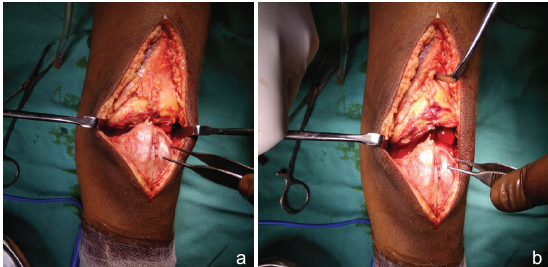
Figure 2: (a and b) Intraoperative picture showing the quadriceps separation from the upper pole of patella.
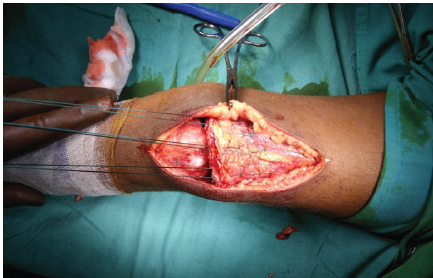
Figure 3: Krakow stitches taken over the quadriceps.
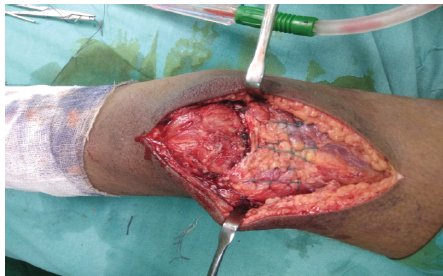
Figure 4: After the repair.
Post-surgery, the patient was placed in an above-knee cast in full extension for 6 weeks. Rehabilitation began with range-of-motion exercises as tolerated after 6 weeks. By the 3rd month, the patient showed gradual improvement in the active range of motion. At the 6-month follow-up, the patient reported significant improvement in knee function. He was able to stand fully weight-bearing and walk unaided. He resumed most of his daily activities with satisfactory outcomes within a year (Table1).
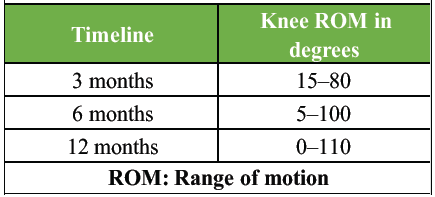
Table 1: Timeline of ROM improvement in follow-ups
Now we got a 3-year follow-up with a full range of motion, can do squatting on his own, and no pain at the operated site. However, as we saw the recent X-ray of the patient, we discovered a spike of bone developing at the upper pole of the patella where we took the stitches (Fig. 5).
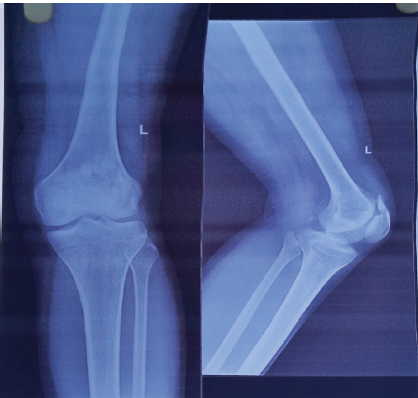
Figure 5: Recent X-ray showing the bony spike.
We did an MRI recently, to look for any abnormality, but the MRI showed that the quadriceps was intact, and no sign of AVN was noted over the upper pole of the patella (Fig. 6a and b).
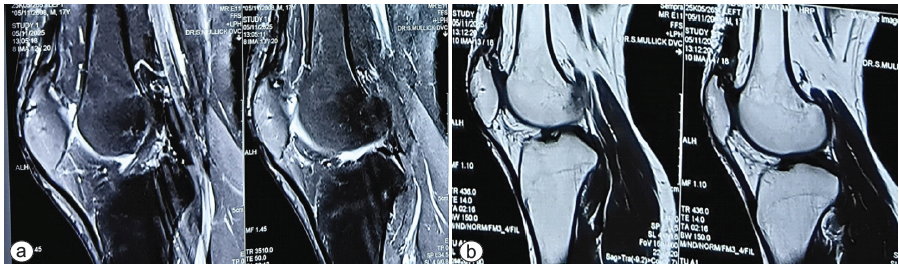
Figure 6: (a and b) Recent magnetic resonance imaging showing the intact quadriceps.
The knee extensor mechanism consists of the quadriceps muscle, quadriceps tendon, medial and lateral patellar retinacula, patella, patellar tendon, and tibial tubercle [3]. Insufficiency in any of these structures can compromise the extensor mechanism, limiting daily activities. Structurally, the quadriceps tendon is biomechanically capable of withstanding high loads without rupturing [4]. A relatively hypovascular zone exists about 1–2 cm superior to the patella, thus making it more susceptible to injury [5]. Complete quadriceps rupture is very rare in the adolescent age group, so there is very little literature for this topic. Most of the literature said the transosseous method is the gold standard for QTR, but all the literature was about adults. Hence, we decided to modify the technique a bit, as we did not drill transosseous holes through the patella from distal to proximal. We directly stitched the tendon to bone with non-absorbable stitches with osseous stitches taken at the proximal pole of the patella. However, the feasibility of transosseous repair depends on patellar thickness and resurfacing status [6]. We have followed a strict post-operative management with a structured rehabilitation program, including delayed weight bearing and gradual range-of-motion exercises, which ultimately led to favorable outcomes[7-10].
In this report, we present a case of a rare traumatic QTR in the adolescent age group, which was managed by primary open repair. Excellent functional outcomes with no extensor lag and excellent restoration of the flexion arch of motion are reported, except the bony spike that we saw recently in the X-ray. The etiology of this particular X-ray pattern may be due to the stitches we took at the proximal pole of the patella directly. Orthopaedic surgeons performing these reconstructions should know that these X-ray findings can occur.
We reported a case of adolescent traumatic quadriceps repair, treated with primary open repair. Follow-up showed no disability from patient’s point of view. Our study has post-operative MRI, which shows intact quadriceps and no other abnormalities. The etiology of this particular X-ray pattern may be due to the stitches we took at the proximal pole of the patella directly.
References
- 1. Zuke WA, Go B, Weber AE, Forsythe B. Quadriceps tendon rupture in an adolescent athlete. Case Rep Orthop 2017;2017:2718013. [Google Scholar] [PubMed]
- 2. Mishra B, Raj M, Behera S, Bhadani JS, Kumar R, Kumar P. Bilateral traumatic rupture of the quadriceps tendon – a case report. J Orthop Case Rep 2024;14:36-40. [Google Scholar] [PubMed]
- 3. LaPrade MD, Kallenbach SL, Aman ZS, Moatshe G, Storaci HW, Turnbull TL, et al. Biomechanical evaluation of the medial stabilizers of the patella. Am J Sports Med 2018;46:1575-82. [Google Scholar] [PubMed]
- 4. Barge-Caballero G, López-Bargiela P, Pombo-Otero J, Pardo-Martínez P. Quadriceps tendon rupture in wild-type transthyretin amyloidosis (ATTRwt). Eur Heart J 2019;40:1307. [Google Scholar] [PubMed]
- 5. Nori S. Quadriceps tendon rupture. J Family Med Prim Care 2018;7:257-60. [Google Scholar] [PubMed]
- 6. Braun S, Flevas DA, Marcos CR, Boettner F, Sculco PK, Sculco TP. Reconstruction of chronic quadriceps tendon rupture: The quadriceps advancement and imbrication technique. J Arthroplasty 2024;39:S237-43. [Google Scholar] [PubMed]
- 7. Cannamela PC, Maak TG, Adeyemi TF, Aoki SK. Traumatic pediatric quadriceps rupture after medial patellofemoral ligament reconstruction: A case report. JBJS Case Connect 2019;9:e0134. [Google Scholar] [PubMed]
- 8. Albuquerque RP, Neto JF, Giordano V, Albuquerque MI, Amaral NP, Barretto JM. Total rupture of the quadriceps muscle in an adolescent. Rev Bras Ortop 2013;48:111-3. [Google Scholar] [PubMed]
- 9. Seguritan RE, Wolfe AR, Mena P, Bibawy J, Bianchi C, Solomon N, et al. Bipartite patella separation and partial quadriceps tendon rupture in the setting of trauma. Radiol Case Rep 2019;14:526-9. [Google Scholar] [PubMed]
- 10. Alkhatatba M, Anaqreh Y, Essa SB, Alma’aiteh A, Ziad Audat H, Obeidat N, et al. Bilateral spontaneous quadriceps tendon rupture: A case report and literature review. SICOT J 2023;9:31. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2024 Bilateral Traumatic Rupture of the Quadriceps Tendon – A Case Report
December 1, 2024 Bilateral Traumatic Rupture of the Quadriceps Tendon – A Case Report March 1, 2025 Atraumatic Bilateral Patellar Tendon Rupture: A Case Report
March 1, 2025 Atraumatic Bilateral Patellar Tendon Rupture: A Case Report January 10, 2018 Impalement Injury to Thigh: A Case Report with Review of Literature
January 10, 2018 Impalement Injury to Thigh: A Case Report with Review of Literature July 10, 2016 A rare case of Glomus Tumor of the Thenar Eminence of the Hand Misdiagnosed as Carpal Tunnel Syndrome.
July 10, 2016 A rare case of Glomus Tumor of the Thenar Eminence of the Hand Misdiagnosed as Carpal Tunnel Syndrome.