
Delayed esophageal perforation can occur even more than a decade after cervical anterior decompression and fusion; long-term surveillance is mandatory.
Dr. Jun Hashimoto, Department of Orthopaedic Surgery, Kudanzaka Hospital, Chiyoda City, Tokyo, Japan. E-mail: hash.orth@tmd.ac.jp
Abstract
Introduction: We describe an exceptionally rare case of delayed esophageal perforation that developed 14 years after anterior decompression and fusion (ADF) of the cervical spine, ultimately necessitating complex revision surgery.
Case Report: A 62-year-old male had undergone C5–C7 ADF and experienced favorable neurological recovery, although post-operative screw loosening was noted. Fourteen years later, he developed progressive numbness and muscle weakness. Endoscopic examination revealed an esophageal perforation adjacent to the anterior plate. Considering the coexistence of cervical myelopathy, the patient underwent C3–T2 posterior decompression and fusion, implant removal, anterior reconstruction with a fibular graft, esophageal fistula closure, pectoralis major myocutaneous flap coverage, and tracheostomy. Following rehabilitation, he was able to resume oral feeding and ambulate with a cane 8 months postoperatively.
Conclusion: Esophageal perforation occurring more than a decade after ADF is extremely uncommon. In this case, chronic implant loosening was likely responsible. Because such complications often require extensive reconstructive procedures, vigilant long-term follow-up is crucial even after satisfactory early recovery.
Keywords: Esophageal perforation, anterior surgery, cervical spine, implant migration.
Cervical anterior decompression and fusion (ADF) is commonly used to treat cervical spondylotic myelopathy, disc herniation, and ossification of the posterior longitudinal ligament. Compared with posterior laminoplasty, ADF is associated with lower rates of C5 palsy and axial neck pain but a higher incidence of systemic complications such as dysphagia and hoarseness [1]. Esophageal perforation is particularly serious because it can lead to mediastinitis and feeding difficulties, often requiring fasting and resulting in malnutrition and systemic decline. The mortality rate for esophageal perforation is approximately 3.29% [2]. However, most esophageal injuries related to ADF are detected intraoperatively or immediately after surgery, and delayed esophageal perforation is extremely uncommon. We present a rare case of delayed esophageal perforation that required extensive treatment, including anterior and posterior cervical spinal fusion and esophageal reconstruction.
A 62-year-old male presented with gait disturbance, numbness, and muscle weakness due to cervical spondylotic myelopathy. He underwent C5–C7 ADF with a plate and cage at another hospital. Six months postoperatively, radiographs showed screw loosening and migration (Fig. 1).
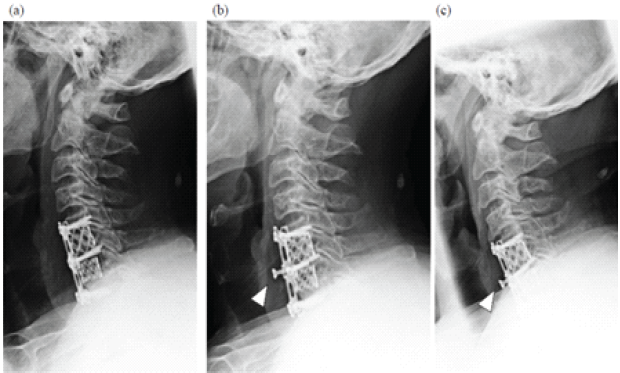
Figure 1: Plain radiographs after anterior cervical decompression and fusion. Radiographs obtained in 1 week (a), 6 months (b), and 3.5 years (c) post-operatively are shown. Migration of the C6 screw is evident at 6 months (arrowhead), although no further progression was observed.
Despite this, his neurological function improved, allowing him to resume independent activities, including recreational baseball. He subsequently stopped attending follow-up visits. At 76 years of age, he returned to the previous hospital with progressive sputum production, worsening limb numbness and weakness, and gait disturbance. Physiological and neurological evaluation revealed bilateral lower-extremity weakness (manual muscle testing: digit extensor 4/4, iliopsoas muscle 3/2, quadriceps muscle 4/4, tibia anterior muscle 5/3, and extensor hallucis longus muscle 4/2), heightened patellar and Achilles tendon reflexes, and dysphagia. His cervical Japanese Orthopaedic Association (JOA) score was 6.5. Radiographs and computed tomography demonstrated vertebral osteolysis around the implant, absence of the right C6 screw, and air between the anterior implant surface and the esophagus (Fig. 2). Magnetic resonance imaging revealed a high-signal lesion from C5 to C7 on short tau inversion recovery sequences with spinal cord compression (Fig. 3). Upper gastrointestinal endoscopy revealed a 2-cm esophageal mucosal perforation with direct exposure of the cervical implant (Fig. 4).
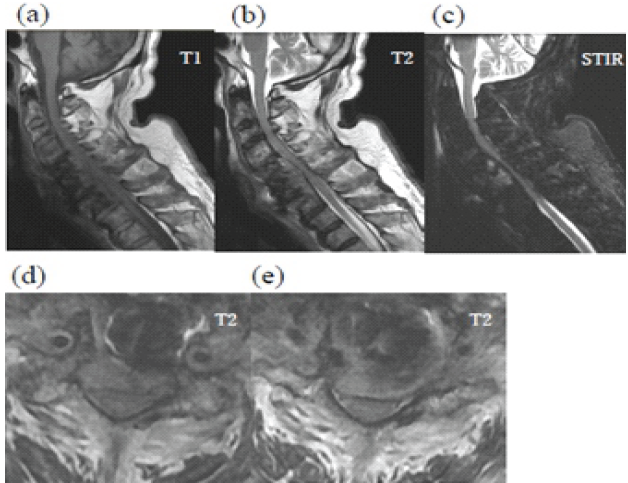
Figure 2: Magnetic resonance imaging of delayed esophageal perforation. Sagittal T1-weighted (a), T2-weighted (b), and short tau inversion recovery (c) images are shown in the upper row. Axial T2-weighted images at the C5/6 (d) and C6/7 levels (e) are shown in the lower row. Signal changes are observed in the C4-C6 vertebrae, and the spinal cord is compressed from the anterior aspect.
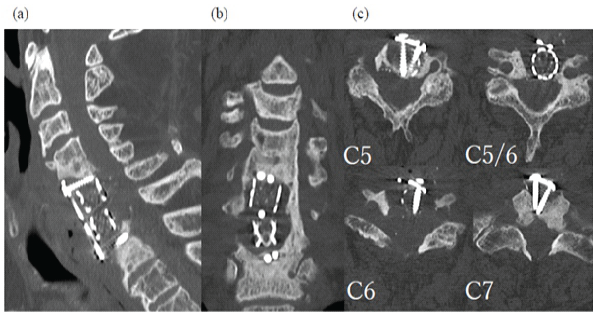
Figure 3: (a-c) Computed tomography (CT) images showing osteolysis and screw disappearance. CT demonstrates osteolysis around the implant and the absence of the right C6 screw.
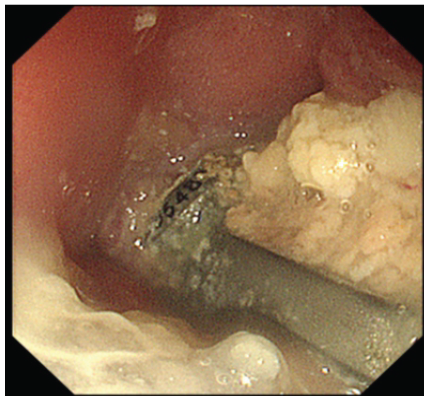
Figure 4: Upper gastrointestinal endoscopic findings. Endoscopy reveals exposure of the anterior cervical plate through a 2-cm defect in the posterior esophageal wall.
He was diagnosed with delayed esophageal perforation and pyogenic spondylitis with associated myelopathy and was referred to our department. On admission, blood tests showed mild inflammation (white blood cell count 5,900/µL; C-reactive protein 0.31 mg/dL) and hypoalbuminemia (3.5 g/dL). His myelopathy continued to worsen, likely due to instability from vertebral osteolysis. Posterior decompression and fusion (C3–T2 fusion with C3–T1 laminectomy) and gastrostomy were performed first, resulting in mild neurological improvement. Three weeks later, anterior surgery was performed in collaboration with head and neck, esophageal, and plastic surgeons. A right-sided incision – opposite the initial surgical approach – was used. A 20-mm defect in the posterior esophageal wall was identified where it contacted the cervical implant and was filled with infected tissue. After debridement, the left fibula was grafted into the C4–C6 vertebral space. The esophageal defect was sutured with endoscopic confirmation from within the lumen. A right pectoralis major myocutaneous flap was then placed to cover the repair and fill the space between the esophagus and reconstructed vertebra. A tracheostomy was added (Fig. 5).
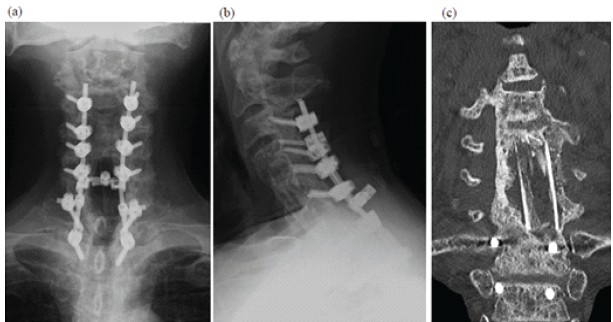
Figure 5: Post-operative plain radiographs and computed tomography image after staged reconstruction surgery. Frontal (a) and lateral (b) plain radiographs and coronal computed tomography images (c) at 1 year postoperatively are shown. Bony union has been achieved.
Total operative time was 561 min with an estimated blood loss of 710 mL. Postoperatively, the patient received cefepime (3 g/day), metronidazole (1500 mg/day), and micafungin (100 mg/day) for 6 weeks with no recurrence of infection. He underwent rehabilitation for dysphagia and received gastrostomy-based nutrition until oral intake began 4 months after surgery. The tracheostomy and gastrostomy were closed at 5 and 8 months, respectively. His myelopathy gradually improved, allowing him to walk with a cane, and his cervical JOA score increased to 10 at 9 months postoperatively.
The incidence of esophageal perforation after cervical ADF is reported to be 0.1–0.45% [3]. Perforations occurring within 30 days of surgery are considered acute, whereas those identified later are classified as delayed [4]. Acute esophageal perforations typically result from intraoperative traction or direct mechanical injury and are usually detected intraoperatively or shortly after oral intake resumes. By contrast, delayed perforations are generally caused by chronic esophageal irritation from implants, such as a loosened screw or plate. A systematic review found that 41% of perforations were associated with implant failure and 31% with chronic mechanical irritation between the implant and surrounding tissue [2,5]. The C6 level – where our patient’s perforation occurred – is particularly vulnerable due to the thin soft-tissue layer between the vertebral body and the esophagus. This region corresponds to the Killian triangle, bordered by the pharyngeal constrictor and cricopharyngeal muscles [6]. In this case, long-standing irritation from the loosened screw likely caused the delayed esophageal perforation and subsequent infection. Although implant failure was noted 6 months after surgery, symptoms related to perforation did not appear until more than a decade later. The mechanism behind this prolonged delay is unclear, but age-related tissue fragility and soft-tissue atrophy associated with weight loss may have increased esophageal vulnerability. Both conservative and surgical approaches have been described for delayed esophageal perforation. Conservative treatment – fasting and antibiotics – may be effective when the patient is clinically stable. Vrouenraets et al. reported that 20% of conservatively treated patients developed residual abscesses, recommending non-operative treatment only for asymptomatic patients with abscesses smaller than 1 cm [7]. Surgical treatment typically involves implant removal and stabilization when instability is present [8]. Adequate soft-tissue coverage is essential to protect the repaired esophagus. Small defects can be reconstructed using the sternocleidomastoid or sternohyoid muscles, whereas larger defects may require a pectoralis major flap or mesh graft [9]. Prior reports indicate that most delayed perforations after ADF were managed with implant removal and flap reconstruction alone [10]. In this case, significant cervical instability with osteolysis, progressive myelopathy, and a large esophageal defect necessitated a two-stage procedure: Posterior fixation followed by anterior reconstruction and coverage with a pectoralis major myocutaneous flap. The diagnosis was delayed partly because the patient did not recognize that his gradually worsening dysphagia was related to post-operative complications and had long discontinued follow-up. The missing right C6 screw was not found on whole-body computed tomography, raising the possibility of migration into the gastrointestinal or thoracic tract, as described in previous reports [11]. Risk factors for delayed infection after ADF include diabetes mellitus, trauma, human immunodeficiency virus, tuberculosis, metabolic disease, and prolonged operative time [12]. Preventive measures may include using low-profile locking plates and ensuring plate coverage with the longus colli muscles to reduce implant prominence and esophageal irritation. The patient experienced prolonged post-operative dysphagia. Known risk factors for dysphagia after ADF include long operative time, use of recombinant human bone morphogenetic protein, endotracheal tube cuff pressure, plate type and positioning (smaller, smoother plates or Zero-Profile implants are associated with less risk), increased C2–C7 kyphotic angle, psychiatric factors, smoking, anterior soft-tissue swelling, and injury to the superior or recurrent laryngeal nerves [13,14]. In this case, contributing factors likely included impaired esophageal function from prior injury, intraoperative nerve traction, tracheostomy, and post-operative scar formation due to flap reconstruction. Dysphagia following esophageal perforation repair has been reported in 28–57% of cases, although most cases improve within 2 years [15].
We encountered a rare case of delayed esophageal perforation and infection occurring 14 years after ADF. Management required extensive reconstructive surgery. Long-term surveillance is necessary after ADF, and reoperation – such as removal of loosened screws – should be considered even in asymptomatic patients, given the risk of esophageal injury.
Delayed esophageal perforation may develop more than 10 years after anterior cervical fusion due to chronic implant loosening, emphasizing the importance of lifelong follow-up after ADF.
References
- 1. Yoshii T, Egawa S, Chikuda H, Wakao N, Furuya T, Kanchiku T, et al. A systematic review and meta-analysis comparing anterior decompression with fusion and posterior laminoplasty for cervical spondylotic myelopathy. J Orthop Sci 2021;26:116-22. [Google Scholar] [PubMed]
- 2. Halani SH, Baum GR, Riley JP, Pradilla G, Refai D, Rodts GE Jr., et al. Esophageal perforation after anterior cervical spine surgery: A systematic review of the literature. J Neurosurg Spine 2016;25:285-91. [Google Scholar] [PubMed]
- 3. Fountas KN, Kapsalaki EZ, Nikolakakos LG, Smisson HF, Johnston KW, Grigorian AA, et al. Anterior cervical discectomy and fusion associated complication. Spine (Phila Pa 1976) 2007;32:2310-7. [Google Scholar] [PubMed]
- 4. Ko SB, Park JB, Song KJ, Lee DH, Kim SW, Kim YY, et al. Esophageal perforation after anterior cervical spine surgery. Asian Spine J 2019;13:976-83. [Google Scholar] [PubMed]
- 5. Zakko P, Rontal M, Park D. Delayed esophageal perforation diagnosed 12 years after anterior cervical diskectomy and fusion: A case report and review of current literature. J Am Acad Orthop Surg Glob Res Rev 2022;6:e22.00080. [Google Scholar] [PubMed]
- 6. Tew JM Jr., Mayfield FH. Complications of surgery of the anterior cervical spine. Clin Neurosurg 1976;23:424-34. [Google Scholar] [PubMed]
- 7. Vrouenraets BC, Been HD, Brouwer-Mladin R, Bruno M, Van Lanschot JJ. Esophageal perforation associated with cervical spine surgery: Report of two cases and review of the literature. Dig Surg 2004;21:246-9. [Google Scholar] [PubMed]
- 8. Von Rahden BH, Stein HJ, Scherer MA. Late hypopharyngo-esophageal perforation after cervical spine surgery: Proposal of a therapeutic strategy. Eur Spine J 2005;14:880-6. [Google Scholar] [PubMed]
- 9. Hanwright PJ, Purnell CA, Dumanian GA. Flap reconstruction for esophageal perforation complicating anterior cervical spinal fusion: An 18-year experience. Plast Recostr Surg Glob Open 2015;3:e400. [Google Scholar] [PubMed]
- 10. Moletta L, Pierobon ES, Salvador R, Volpin F, Finocchiaro FM, Capovilla G, et al. Pharyngo-esophageal perforation following anterior cervical spine surgery: A single center experience and a systematic review of the literature. Global Spine J 2022;12:719-31. [Google Scholar] [PubMed]
- 11. Gazzeri R, Tamorri M, Faiola A, Gazzeri G. Delayed migration of a screw into the gastrointestinal tract after anterior cervical spine plating. Spine (Phila Pa 1976) 2008;33:E268-71. [Google Scholar] [PubMed]
- 12. Chen YC, Zhang L, Li EN, Ding LX, Zhang GA, Hou Y, et al. Late deep cervical infection after anterior cervical discectomy and fusion: A case report and literature review. BMC Musculoskelet Disord 2019;20:437. [Google Scholar] [PubMed]
- 13. Liu J, Hai Y, Kang N, Chen X, Zhang Y. Risk factors and preventative measures of early and persistent dysphagia after anterior cervical spine surgery: A systematic review. Eur Spine J 2018;27:1209-18. [Google Scholar] [PubMed]
- 14. Radcliff KE, Bennett J, Stewart RJ, Kepler CK, Sidhu GS, Hilibrand AS, et al. Change in angular alignment is associated with early dysphagia after anterior cervical discectomy and fusion. Clin Spine Surg 2016;29:248-54. [Google Scholar] [PubMed]
- 15. Frankel L, Ardeljan AD, Santizo G, Guerra M, Gharat G, Alnajar S, et al. Esophageal perforation in a 76-year-old man after C5-C7 anterior discectomy and anterior plate fusion. World J Oncol 2013;14:158-63. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 From Nail to Fail: Complications Encountered with Clavicle Nailing – A Series of 3 Cases
August 1, 2025 From Nail to Fail: Complications Encountered with Clavicle Nailing – A Series of 3 Cases November 10, 2022 Acute Paraparesis in a Patient after High Velocity Manipulation of Cervical Spine and its Management
November 10, 2022 Acute Paraparesis in a Patient after High Velocity Manipulation of Cervical Spine and its Management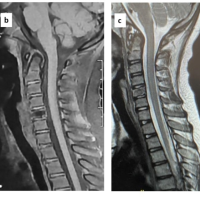 August 10, 2022 Eosinophilic Granuloma as a Solitary Lytic Lesion of the Cervical Spine in a Child
August 10, 2022 Eosinophilic Granuloma as a Solitary Lytic Lesion of the Cervical Spine in a Child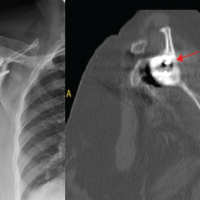 January 1, 2025 Diagnosing Mycobacterium Kansasii in Shoulder Periprosthetic Joint Infection: A Rare Case Report
January 1, 2025 Diagnosing Mycobacterium Kansasii in Shoulder Periprosthetic Joint Infection: A Rare Case Report