
Early osteonecrosis monitoring should be performed in patients with atraumatic joint pain up to 2.5 years after compromised systemic circulation and systemic inflammation.
Dr. Ricki Sheldon, Department of Osteopathic Manipulative Medicine, A.T. Still University, Kirksville, Missouri. E-mail: rikkisheldon@gmail.com
Abstract
Introduction: Multifocal osteonecrosis (MFON) (avascular necrosis [AVN] in more than three joints) is rare. It occurs when blood flow to multiple osseous sites is disrupted, and it is usually associated with systemic disease, coagulopathies, or high cumulative doses of steroids. The current report describes a case of bilateral femoral and humeral head AVN misdiagnosed as fibromyalgia several years after a severe COVID-19 infection with complications of asystole and multi-organ failure.
Case Report: A 37-year-old woman presented with joint pain that started 2 years and 4 months after a COVID-19 infection that was complicated by respiratory failure and cardiac arrest. She denied drinking alcohol or smoking and had no past medical history of osteoporosis, autoimmune diseases, coagulopathies, or chronic steroid use. In the hospital, respiratory distress was managed with a cumulative dose of 1640 mg of steroids over 27 days. Her disease course was complicated by asystole and an exacerbated systemic inflammatory process, as evidenced by multi-organ failure, including acute kidney disease, shock liver, and encephalopathy.
Conclusion: Patients should be monitored for bone and joint pain indicative of possible osteonecrosis complications for several years after recovery from systemic diseases like COVID-19, regardless of whether they received high-risk cumulative steroid doses. Further, MFON should be considered with prolonged proinflammatory states, especially with concomitant cardiac events that compromise systemic sanguinous perfusion. Misdiagnosis and late magnetic resonance imaging can defer definitive treatment during the early, treatable stages of this disease.
Keywords: Osteonecrosis, avascular necrosis, multifocal osteonecrosis, COVID-19, risk factor, steroid.
Non-traumatic avascular necrosis (AVN) occurs when the blood supply to osseous tissue is disrupted. It is associated with systemic oral or intravenous corticosteroid therapy and with coagulopathies and highly inflammatory systemic illnesses, such as liver disease, cancer treatments, connective tissue disorders, and inflammatory bowel disease [1]. When occurring in more than three anatomic sites, it is called multifocal osteonecrosis (MFON). The most common risk factor for MFON is chronic high-dose systemic corticosteroid use, but it can also occur with illnesses affecting systemic perfusion like coagulopathies, leukemia, or sickle cell disease [2]. Although bilateral femoral head AVN is relatively common because of its tenuous arterial supply, MFON is rare [3,4]. Powell et al. [5] first reported the relationship between corticosteroids and AVN in organ transplant patients taking chronic steroid therapy. Corticosteroids can increase fat production, impair collagen synthesis, cause endothelial dysfunction, and alter osteoblast function [1]. Sanguinous supply may be compromised if increased lipids block flow in the rigid interosseous vascular pathways or if vascular integrity is affected in delicate extramedullary arteries [1]. Because of steroid-induced reductions in osteoblast functionality, bone remodeling may suboptimally compensate for the original injury [1]. Symptoms may take months to 1 year to appear in individuals aged 30–60 years [5]. Cumulative doses of steroids may be more detrimental than daily doses, and underlying comorbidities may increase AVN risk [6]. Association Research Circulation Osseous classification criteria for osteonecrosis of the femoral head [6] indicate increased AVN risk with cumulative doses >2 g over 3 months. Mont et al. [7] found increased AVN risk in patients with systemic lupus erythematosus with daily doses >20 mg/d; that every additional 10 mg/d increased incidence by 3.6%, and that cumulative doses of 2 g increased risk by 6.7%. COVID-19 infections create hypoxia, increase inflammatory markers, induce hypercoagulability, dysregulate vascular tone, and reduce osteoblast function [8,9,10,11]. Patients are often treated with steroids because doses as low as 6 mg/d have been shown to improve hypoxia and reduce acute hypoxic respiratory failure (AHRF) [10]. Although AVN is documented in COVID-19 patients without concurrent steroid use, there is some disagreement about whether steroid treatments further increase AVN risk [10,12,13]. Studies investigating severe acute respiratory syndrome, which is in the same virus family as COVID-19, reported an increased risk for AVN and MFON with cumulative corticosteroid doses as low as 480 mg over 2–6 months [14]. In patients aged 20–60 years, AVN symptoms after COVID-19 are insidious and may take 80 days to 2.5 years to appear [10,15]. Systemic infections and corticosteroid use may induce AVN at lower doses than previously considered safe. Variabilities in duration and doses of steroids, coupled with increased risk from underlying comorbidities, make it difficult to define safe steroid-dose thresholds. In the current report, we describe a case of bilateral femoral and humeral head AVN misdiagnosed as fibromyalgia several years after a severe COVID-19 infection with complications of asystole and multi-organ failure, treated with a cumulative corticosteroid dose <2 g.
A 37-year-old woman with a body mass index (BMI) >40 presented to our orthopedic clinic in April 2024 for shoulder and hip pain. She was a non-smoker and denied drug and alcohol use. She reported first noticing joint pain in November 2023, approximately 2 years and 4 months after a severe COVID-19 infection in July 2021. Her COVID-19 disease process was complicated by asystole, acute kidney injury (AKI), shock liver, and acute encephalopathy. In the hospital, her AHRF was managed with intubation and a cumulative dose of 1640 mg of steroids. Before COVID-19, her past medical history included Class III obesity, prediabetes, polycystic ovarian syndrome, hypertriglyceridemia, hypertension, chronic bronchitis, anxiety, and depression. She was taking no chronic steroids; her bronchitis was managed with albuterol and montelukast. Initially, the patient’s COVID-19 infection was diagnosed at the pharmacy, but she later presented to the emergency department for respiratory distress, where 2 days of 20 mg of prednisone were prescribed. Due to worsening symptoms, the patient was then hospitalized for AHRF and received 40 mg of methylprednisolone twice per day. After succinylcholine administration for intubation, she went asystolic and needed cardiopulmonary resuscitation. After reanimation, transesophageal echocardiography showed a transient cardiomyopathy with reduced ejection fraction at 45–50%. Laboratory values showed elevated D-dimer levels, peaking at 17.73 mg/L (normal <0.5 mg/L), and elevated inflammatory markers, specifically an interleukin-6 of 56.54 pg/mL (normal <7.01 pg/mL), C-reactive protein of 279.30 mg/L (normal < 5 mg/L), and procalcitonin of 0.11 ng/mL (normal <0.1 ng/mL). During hospitalization, creatinine levels increased, indicating AKI; her alanine transaminase rose to 1318 U/L, indicating shock liver. She was also diagnosed with acute encephalopathy, evidenced by abrupt neurological changes, disorientation, reduced concentration, and slow speech. Overall, she spent 27 days in the hospital and received 1640 mg of steroids. After discharge, she received rehabilitative care at a nursing home. In November 2023, approximately 2 years and 4 months after being admitted for COVID-19, she was referred to rheumatology by her primary care physician for hip, knee, and shoulder joint pain of unknown etiology. With a history of metabolic encephalopathy overlying preexisting anxiety and depression, radiographic imaging without osseous findings, a positive antinuclear antibody, and no other rheumatological biomarkers, the rheumatologist diagnosed her with fibromyalgia. In March 2024, she was referred to a bariatric arthroplasty clinic for worsening hip pain and new-onset numbness and tingling. At the clinic visit, she had a positive Stinchfield test, and she reported a previous magnetic resonance imaging (MRI) of her left knee that had shown evidence for bone infarcts. Radiographic imaging of the hips was performed, showing bilateral AVN with collapse of the left femoral head. The patient was told that total joint arthroplasty was not an option at that time due to her elevated BMI and inflammatory markers. In April 2024, her primary care physician referred her to our orthopedic clinic for joint aspiration and intra-articular steroid injections. At that time, she was barely able to walk and also complained of increasing shoulder pain. Physical examination showed bilateral pain on palpation over the greater trochanters and the biceps tendons; she had a positive apprehension test and reduced shoulder range of motion. In April 2024, bilateral hip fluid aspiration with intra-articular steroid injections was performed. No marked effusions were found, and fluid cultures failed to show growth. Pain relief from the steroid injection lasted 2 weeks. Being a poor surgical candidate, in June 2024, bilateral femoral head core decompressive surgery was performed to try to delay total hip arthroplasty (THA) by improving interosseous blood flow. Due to continued pain, in August 2024, the shoulders and hips were imaged. Radiographs of the hips indicated no improvement of AVN despite decompressive surgery; there was Ficat-Arlet stage IV AVN bilaterally with crescentic sclerosis and bilateral femoral head collapse with greater collapse of the left femoral head (Fig. 1). Bilateral computed tomography angiography of the shoulders showed AVN affecting 75% of the surface areas in the humeral heads bilaterally, bilateral tendinosis of supraspinatus and infraspinatus muscles, and some degenerative changes in the long head of the right biceps (Fig. 2 and 3).
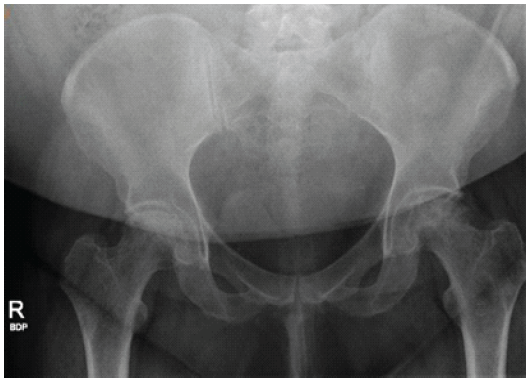
Figure 1: Radiograph of the pelvis of a 37-year-old woman with multifocal osteonecrosis. The image was obtained on August 21, 2024, approximately 2 weeks after core decompression and before total hip arthroplasty. The severity of avascular necrosis was diagnosed at Ficat and Arlet Stage IV bilaterally because of bilateral head collapse.
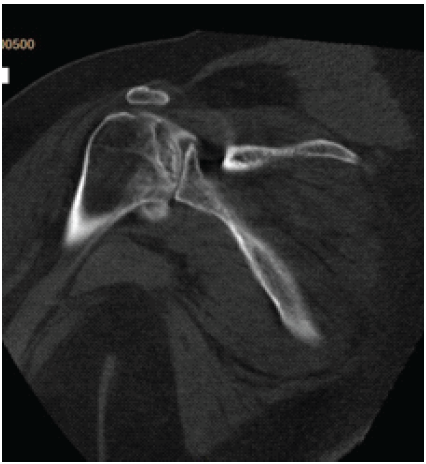
Figure 2: Computed tomography image of the left shoulder of a 37-year-old woman with multifocal osteonecrosis. The image was obtained on August 21, 2024. At present, no interventions have been performed on the avascular necrosis in the patient’s shoulders.
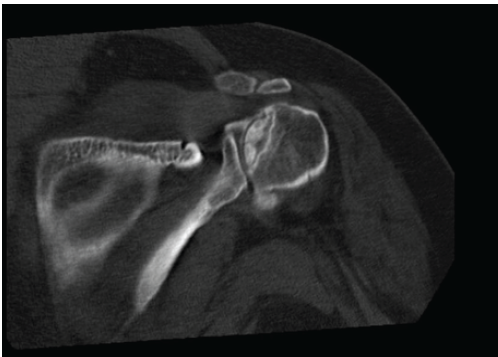
Figure 3: Computed tomography image of the right shoulder of a 37-year-old woman with multifocal osteonecrosis. The image was obtained on August 21, 2024. At present, no interventions have been performed on the avascular necrosis in the patient’s shoulders.
Given the continued severity of symptoms and core decompression failure backed by radiographic evidence, it was decided that bilateral THAs were needed. Because the patient had already paid her insurance deductible for 2024, she opted to undergo THA on both hips before the end of the year. Despite continued obesity, in September 2024, a left THA was performed; in December 2024, a right THA was performed.
Currently, the patient still has a BMI >40; does not have any underlying coagulopathies, leukemias, or autoimmune inflammatory conditions; and does not take chronic steroids. With reduced hip pain, she can now walk but continues to experience severe bilateral shoulder pain.
According to the Ficat and Arlet classification for osteonecrosis in the femoral head, early stages of AVN may be asymptomatic or produce mild pain without visible radiographic changes [16]. The patient in this current report was likely in early-stage osteonecrosis when diagnosed with fibromyalgia 2 years and 4 months after hospitalization for COVID-19. However, her care was not referred to orthopedics until her disease had progressed to advanced-stage osteonecrosis. Our patient’s COVID-19–associated increase in inflammatory markers, coupled with cardiac arrest, put her at risk for thrombotic microembolisms [8,9,10,11] and seemed to be associated with a system-wide sanguinous perfusion crisis affecting multiple organs (kidney, liver, and brain) during hospitalization. Her critical condition when receiving steroid treatments may have increased her risk for osteonecrosis despite receiving a cumulative dose below the recommended threshold of 2 g [6]. COVID-19, coagulopathies, and steroid use in immune-compromised and pro-inflammatory states have been shown to increase risk for unilateral and bilateral AVN [1,5,17]. However, MFON after COVID-19 has only been documented in one case report [18], where symptoms were reported 2 months after a COVID-19 infection not treated with steroids. Given that cytokines are known to damage endothelial cells, promote microembolisms, and increase bone resorption [18], our patient’s perfusion crisis during COVID-19 infection may have been exacerbated by continued post-COVID systemic inflammation, thereby prolonging poor osseous perfusion and promoting a systemic AVN-prone environment in multiple sites simultaneously. Since early stage asymptomatic and mild osteonecrosis can be visualized on MRI, even without radiographic evidence [16], MRI monitoring of arthralgia complaints for up to 2 years after COVID infection, as has previously been suggested [18,19], may have resulted in an earlier diagnosis and improved her outcome. Ultimately, this case highlights the importance of considering previous medical history for pro-inflammatory and perfusion-compromising events when diagnosing atraumatic bone and joint pain. A major limitation of the current case report was an inability to follow the patient throughout her yearslong disease process. The data presented here were based on available medical records from multiple hospitals and medical facilities where she received treatment over this period. Unfortunately, patient records from her nursing home stay were unreconcilable. Because she received care from multiple providers, and considering possible differences in each provider’s interpretation, gaps may exist in data and continuity of care. Furthermore, our care focused on the most symptomatic joints. There may have been possible necrosis in other, unimaged locations, or additional sites with small bone infarcts may have self-resolved with conservative care. For example, no follow-up imaging occurred for the left knee, which was reported as having a bone infarct on a previous MRI.
Early stage AVN is not visible on radiographs, and definitive care should not be delayed, as in the current case, when the condition is misdiagnosed as fibromyalgia. From a clinical perspective, this patient’s lack of follow-up is concerning. Because AVN progression is insidious and irreversible in advanced stages, early stages, more easily treatable with nonsurgical options, may be asymptomatic or mild for years after the original insult. By the time the patient presented to orthopedics, she had advanced-stage osteonecrosis in multiple joints and needed bilateral THA to manage symptoms. Given known AVN risks, early MRI imaging and joint pain monitoring should be indicated for over 2 years after known pro-inflammatory, microembolism-prone, and perfusion-compromising events, like COVID-19, treated with or without steroids. It should also be more broadly recognized that steroid use can have more damaging effects when systemic inflammation and perfusion-compromising pathology coexist.
When evaluating patient complaints of bone or joint pain, clinicians should consider past systemic illness with possible compromised sanguinous perfusion or chronic proinflammatory states with or without steroids as a risk factor for osteonecrosis. Present or past cumulative steroid use, even under recommended threshold guidelines, may exacerbate this risk. Because osteonecrosis occurs insidiously over several years, early MRI monitoring of joint pain to rule out osteonecrosis is important to avoid misdiagnosis and promote timely management of this limb-threatening condition. When a patient’s medical history includes a proinflammatory, perfusion-compromising event, scheduled follow-up assessments for over 2 years after discharge should be encouraged to monitor for possible AVN complications.
References
- 1. Richards RN. Short-term corticosteroids and avascular necrosis: Medical and legal realities. Cutis 2007;80:343-8. [Google Scholar] [PubMed]
- 2. Sun W, Shi Z, Gao F, Wang B, Li Z. The pathogenesis of multifocal osteonecrosis. Sci Rep 2016;6:29576. [Google Scholar] [PubMed]
- 3. Çavuş MC, Afacan MY, Zeytunlu A, Yapar A. Bilateral femur and humerus avascular necrosis associated with corticosteroids: A rare case presentation. Cureus 2023;15:e50834. [Google Scholar] [PubMed]
- 4. LaPorte DM, Mont MA, Mohan V, Jones LC, Hungerford DS. Multifocal osteonecrosis. J Rheumatol 1998;25:1968-74. [Google Scholar] [PubMed]
- 5. Powell C, Chang C, Naguwa SM, Cheema G, Gerschwin ME. Steroid induced osteonecrosis: An analysis of steroid dosing risk. Autoimmun Rev 2010;9:721-43. [Google Scholar] [PubMed]
- 6. Hines JT, Jo WL, Cui Q, Mont MA, Koo KH, Cheng EY, et al. Osteonecrosis of the femoral head: An updated review of ARCO on pathogenesis, staging and treatment. J Korean Med Sci 2021;36:e177. [Google Scholar] [PubMed]
- 7. Mont MA, Pivec R, Banerjee S, Issa K, Elmallah RK, Jones LC. High-dose corticosteroid use and risk of hip osteonecrosis: Meta-analysis and systematic literature review. J Arthroplasty 2015;30:1506-12.e5. [Google Scholar] [PubMed]
- 8. Sakellariou E, Argyropoulou E, Karampinas P, Galanis A, Varsamos I, Giannatos V, et al. A comprehensive review of COVID-19-infection-and steroid-treatment-associated bone avascular necrosis: A multi-study analysis. Diagnostics (Basel) 2024;14:247. [Google Scholar] [PubMed]
- 9. Hassan AA, Khalifa AA. Femoral head avascular necrosis in COVID-19 survivors: A systematic review. Rheumatol Int 2023;43:1583-95. [Google Scholar] [PubMed]
- 10. Sehrawat S, Ojha MM, Gamanagatti S, Nag HL, Kumar V. Is COVID-19 an independent risk factor for the development of avascular necrosis of the hip? A retrospective study to evaluate the factors associated with avascular necrosis of the hip in patients who had COVID-19 infection. Int Orthop 2024;48:745-52. [Google Scholar] [PubMed]
- 11. Fouda EA, Badr EA, Gawesh D, Mahmoud MA. The role of NOS3-rs1799983 and NOS3- rs2070744 SNP in occurrence of avascular necrosis as a post COVID-19 complication. BMC Med Genomics 2024;17:217. [Google Scholar] [PubMed]
- 12. Sulewski A, Sieroń D, Szyluk K, Dąbrowski M, Kubaszewski L, Lukoszek D, et al. Avascular necrosis bone complication after active COVID-19 infection: Preliminary results. Medicina (Kaunas) 2021;57:1311. [Google Scholar] [PubMed]
- 13. Hogea B, Suba MI, Abu-Awwad SA, Cuntan P, Popa MV, Braescu RD, et al. Exploring the association between COVID-19 and femoral head necrosis: A comprehensive review. Life (Basel) 2024;14:671. [Google Scholar] [PubMed]
- 14. Godoy-Monzón D, Cid-Casteulani A, Svarzchtein S, Sasaki S, Pascual-Espinosa JM. Avascular necrosis of the femoral head after COVID-19: Clinical presentation and management. Clinical-functional outcomes of decompression and supplementation with bone marrow cell aspirate. Necrosis avascular de la cabeza femoral tras COVID-19: Presentación clínica y manejo. Resultados clínico-funcionales de descompresión y suplementación con aspirado de células de médula ósea. Acta Ortop Mex 2024;38:208-13. [Google Scholar] [PubMed]
- 15. Migliorini F, Maffulli N, Shukla T, D’Ambrosi R, Singla M, Vaish A, et al. The pandemic is gone but its consequences are here to stay: Avascular necrosis following corticosteroids administration for severe COVID-19. J Orthop Surg Res 2024;19:135. [Google Scholar] [PubMed]
- 16. Kearns C. Ficat and Arlet Classification of Osteonecrosis of the Femoral Head. Radiopaedia; 2024. Available from: https://radiopaedia.org/articles/ficat-and-arlet-classification-of-osteonecrosis-of-the-femoral-head?lang=us [Last accessed on 2025 Jun 16]. [Google Scholar] [PubMed]
- 17. Seong J, Babakulov A, Asilova S, Shakhnoza B, Nodira M, Mirzayev A. Osteonecrosis of the femoral head in post-COVID-19 patients: A retrospective comparative study. J Orthop Surg Res 2025;20:362. [Google Scholar] [PubMed]
- 18. Klimenko AA, Demidova NA, Andryashkina DY, Babadayeva NM, Kondrashov AA, Saakyan YM. Multifocal osteonecrosis as a consequence of a new coronavirus infection. Nauchno Prakticheskaya Revmatol 2023;61:34-41. [Google Scholar] [PubMed]
- 19. Bone Circulation and Osteonecrosis Professional Committee Shockwave Medical Specialty Committee of Chinese Research Hospital Association. Expert consensus on prevention and treatment strategies for osteonecrosis of femoral head during the prevention and control of novel coronavirus pneumonia. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2020;34:1031-5. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2025 Complex Revisions in Total Hip Arthroplasty Amidst COVID-19 Delays: A Case Report
February 1, 2025 Complex Revisions in Total Hip Arthroplasty Amidst COVID-19 Delays: A Case Report January 1, 2025 Is there an Increase in Total Hip Arthroplasty Due to Osteonecrosis of Femoral Head After Covid-19 Pandemic?: A Retrospective Study Among Patients in Central Karnataka, India
January 1, 2025 Is there an Increase in Total Hip Arthroplasty Due to Osteonecrosis of Femoral Head After Covid-19 Pandemic?: A Retrospective Study Among Patients in Central Karnataka, India October 10, 2023 Joint-preserving Surgery for Idiopathic Bilateral Osteonecrosis of the Distal Tibia: A Case Report
October 10, 2023 Joint-preserving Surgery for Idiopathic Bilateral Osteonecrosis of the Distal Tibia: A Case Report June 10, 2022 Avascular Necrosis of the Hip Triggered by COVID-19 Infection in a Patient with Sickle Cell Disease: A Case Report
June 10, 2022 Avascular Necrosis of the Hip Triggered by COVID-19 Infection in a Patient with Sickle Cell Disease: A Case Report