
Minimizing Metal, Maximizing Motion: Results of headless compression screw fixation of capitellum fractures through a lateral-based elbow approach provide stable, anatomy-preserving fixation with excellent functional range of motion and minimal hardware-related complications.
Dr. Udit Sourav Sahoo, Department of Orthopaedics, SCB Medical College, Cuttack - 753 007, Odisha, India. E-mail: uditsouravsahoo@gmail.com
Abstract
Introduction: Capitellum fractures are rare injuries contributing only 1% of all elbow fractures. Being such a rare injury, there is a lack of consensus with regard to the treatment recommendations. This study aims to evaluate the functional outcome of capitellum fractures treated by open reduction and internal fixation (ORIF) with headless screws through a lateral approach.
Materials and Methods: The study design was a prospective observational study conducted on 61 patients who were undergoing ORIF through a lateral approach to the elbow, between January 2023 and August 2025, at a tertiary care level 1 trauma center. The Oxford elbow score (OES) was recorded post-surgery, starting at 2 weeks and then at 2-monthly intervals.
Results: The mean OES at 6 months was 32.6 ± 7.3 (18–46). Mean pronation–supination arc was 86.9 ± 20.2 (range 40–110°). Mean flexion–extension arc was 131.1 ± 2.9° (range 110–150°, standard deviation 11.5), with a 95% confidence interval of 128.2–134.0°. Our results suggest that ORIF is a safe and effective treatment option for a stable, pain-free elbow with a good range of motion. There was no evidence of avascular necrosis or arthritic changes. The mean duration of follow-up was 15.8 ± 3.2 months (range: 12–27 months).
Conclusion: Headless compression screw fixation via a lateral elbow approach yielded stable fixation with excellent functional outcome for capitellum fractures in our study.
Keywords: Capitellum fracture, open reduction and internal fixation of capitellum fractures.
Fractures of the capitellum represent an uncommon subset of elbow injuries, comprising roughly 1% of reported elbow fractures. They most often result from axial forces transmitted through an extended elbow [1,2]. These fractures typically occur due to axial loading of a fully extended elbow [3,4] or as a result of direct impact to the lateral aspect of the elbow. Treatment options include conservative management with casting, fragment excision, and surgical fixation using Kirschner wires (K-wires), headless compression screws, or anatomical plates [5,6]. Given the rarity of this injury, consensus regarding optimal management remains lacking in the literature [6]. Headless compression screws are designed to achieve stable interfragmentary fixation while remaining recessed below the articular surface, thereby reducing the risk of cartilage injury and post-operative joint irritation. This stability allows early post-operative mobilization, and implant removal is generally unnecessary [7,8]. The present study aimed to evaluate the clinical outcomes of capitellum fractures treated with open reduction and internal fixation (ORIF) using headless compression screws through a lateral-based approach to the elbow.
A total of 61 consecutive patients with isolated capitellum fractures treated with ORIF between January 2023 and August 2025 at a tertiary care Level 1 trauma center were included. Institutional ethical committee approval was obtained (IEC 717, dated January 25, 2023). Written informed consent was obtained from participants. Inclusion criteria were age ≥18 years, isolated capitellum fractures or capitellum fractures with limited trochlear involvement, and treatment with ORIF. Patients with pathological fractures, associated ipsilateral upper limb fractures affecting elbow function, and open fractures with extensive soft-tissue injury were excluded. All patients underwent standard anteroposterior and lateral radiographs and computed tomography with three-dimensional reconstruction to accurately define fracture morphology and plan surgical fixation (Fig. 1a and b). Fractures were classified according to the Bryan and Morrey classification with McKee modification where applicable.
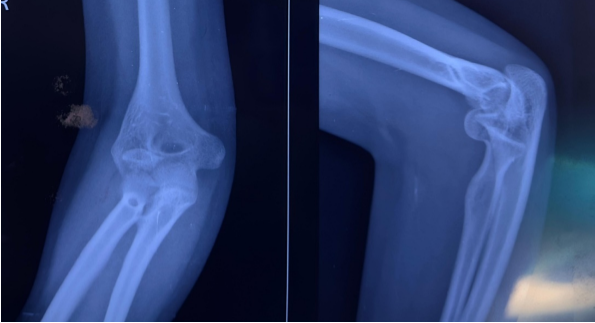

Figure 1: (a) Pre-operative X-ray radiograph. (b) Pre-operative computed tomography scan.
All surgeries were performed under regional anesthesia with the patient in the supine position. Exposure was achieved through a lateral elbow approach, most commonly through the Kocher or Kaplan interval, ensuring preservation of the lateral collateral ligament complex (Fig. 2).
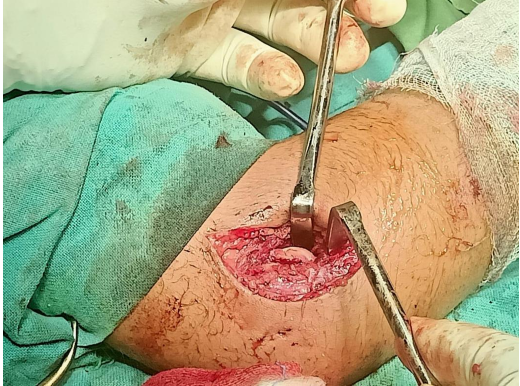
Figure 2: Kocher’s approach to the elbow joint for open reduction and internal fixation.
Fracture fragments were anatomically reduced under direct visualization and temporarily stabilized with K-wires and 1 or 2 number of 3.5 mm headless compression screws were inserted in either anterior-to-posterior or posterior-to-anterior direction, depending on the fracture configuration (Fig. 3).

Figure 3: Intra-operative fluoroscopy for assessment of reduction and screw placement.
In some cases, to avoid the articular surface, screws were angled slightly. In cases where the capitellar fragment was large, screws were directed in a posterior to anterior direction. Anterior-to-posterior direction was generally preferred for most of the cases due to convenience. Screws were countersunk beneath the articular surface to avoid cartilage damage. Fluoroscopy was used to confirm reduction, screw position, and joint congruity. Postoperatively, the elbow was immobilized in a posterior slab for 2 weeks. Graduated elbow mobilization was commenced once pain permitted, with the aim of reducing post-operative stiffness. Indomethacin was given for prophylaxis against heterotopic ossification. The primary outcome was the Oxford elbow score (OES) at the final follow-up. Secondary outcomes included demographics, radiographic fracture union, post-operative complications, and final elbow range of motion (ROM). Patient evaluation and data collection were done by orthopedic surgeons in the outpatient department, other than the treating surgeon, on a case-by-case basis. Continuous variables were reported as means with ranges, and categorical variables as frequencies and percentages. Statistical analysis was done using the Statistical Package for Social Sciences software. ROM and functional scores were normally distributed, as found out using the Shapiro–Wilk test, and parametric tests were used to generate the P-value.
A total of 61 patients were included in the study. The mean age was 50.1 ± 13.3 (26–76 years). The affected side was predominantly the right elbow in 38 patients (63%), whereas the left elbow was involved in 23 patients (37%). The mean time for radiological union was 9.2 weeks (range 6–15 weeks) (Fig. 4).

Figure 4: Follow-up X-ray radiograph at 3 months showing radiological union.
The mean pronation–supination arc was 86.9 ± 20.2° (range, 40–110°) (Fig. 5). Mean flexion extension arc was 131.1 ± 2.9° (range 110–150°, standard deviation 11.5), with a 95% confidence interval of 128.2–134.0° (Fig. 5).
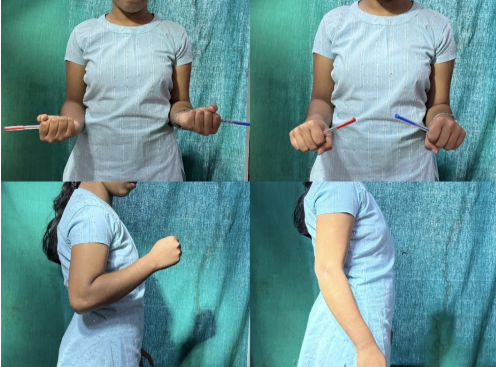
Figure 5: Clinical photograph at 3 months follow-up showing excellent elbow range of movement.
OES results demonstrated a mean pain score of 11.0 ± 2.9 (range, 6–16), function score of 10.9 ± 2.2 (6–15), and social interaction score of 10.7 ± 2.3 (6–15). The mean total OES was 32.6 ± 7.3 (range, 18–46), indicating good elbow function with minimal to no impairment (OES of >32–48). The mean duration of follow-up was 15.8 ± 3.2 months (range: 12–27 months). There were no cases of infection, non-union, implant impingement, or hardware prominence in the study. Results are summarized in Table 1.
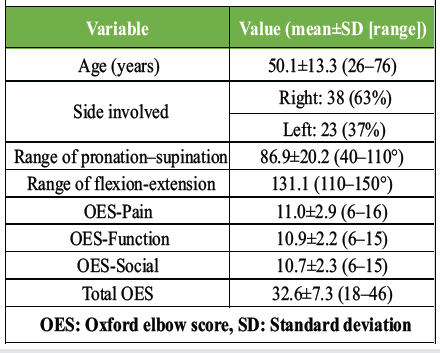
Table 1: Patient characteristics and outcomes
The results of our study indicate that the use of headless compression screws for ORIF of capitellum fractures through a lateral-based elbow approach is a successful method that achieves good pain control and improved elbow function. In our cohort of 61 patients, consistent post-operative improvement was observed using the OES across pain, function, and social domains, supporting the reliability of this fixation technique for managing capitellum fractures [8,9,10]. The management of capitellar fractures is technically demanding, largely because of their intra-articular involvement, limited fragment size, and the well-recognized tendency toward elbow stiffness after injury [11,12]. In this study, we report a mean post-operative pronation–supination arc of 86.9° and a mean flexion-extension arc of 131.1°, which represents a favorable outcome given the average patient age of 50 years and the known propensity for stiffness following elbow trauma, particularly in older individuals [13,14]. Although full restoration of motion was not achieved in all cases, the range obtained was sufficient for activities of daily living, as supported by functional outcome scores [15]. Functional assessment using the OES demonstrated excellent clinical benefit with this treatment method. The mean total OES of 32.6 reflects improved elbow-related quality of life, with parallel improvements in pain relief, functional performance, and social participation [15]. The low pain scores observed may be attributed to the use of headless compression screws, which provide stable fixation, allowing early mobilization while minimizing joint irritation due to reduced implant prominence [7,8,16]. Importantly, no complaints related to implant prominence or hardware-related discomfort were noted in our cohort, complications that are frequently reported with plate fixation [17]. The higher proportion of right-sided injuries observed in this study is consistent with previous reports and may be related to injury mechanisms involving falls onto the dominant limb [18]. Achieving satisfactory functional outcomes in these higher-demand extremities represents a notable success. Furthermore, no cases of non-union, radiocapitellar arthritis, or avascular necrosis were identified at final follow-up. Headless compression screws, being buried beneath the articular surface, reduce the risk of implant prominence and are particularly well suited for articular fractures such as those of the capitellum [7,16,19]. Direction of screw placement is a controversial issue in the context of capitellum fracture fixation. Dubberley et al. [4] placed the screw from the posterior to the anterior direction. Mighell and Frankle [19] argued that they preferred to place the screws from the anterior to the posterior, thus preserving the posterior flap and not disturbing the blood supply of the capitellum. We inserted the screws in either direction, depending on the fracture morphology. Anterior-to-posterior direction was more convenient, because it allows the screw to be inserted perpendicular to the fracture plane under direct vision. In some cases, to avoid the articular surface, screws were slightly angled. In cases where the capitellar fragment was large and the posterior humerus bone stock was thinner, comminuted, or posterior trochlear involvement was present, screws were directed in a posterior-to-anterior manner. We did not encounter any screw-related complications in any patient after surgery. Poynton et al. [20] compared headless screws and Kirschner wire fixation in Type I capitellar fractures to conclude that Herbert screws resulted in earlier mobilization and better functional outcomes. Sultan et al. [21], in their retrospective study on Type I and IV fractures, reported excellent functional outcomes in 10 out of 15 patients treated with headless screws. The average time for union was 12 weeks, with no cases of non-union in their study. Nolte et al. [22] in their cadaveric study suggested that stability can be augmented with the use of a buttress plate in cases requiring additional structural support, such as osteoporotic and comminuted fractures involving the distal humerus posterior to the capitellum component. Overall, these findings suggest that Herbert screws consistently offer excellent functional and radiographic outcomes, which is also supported by the findings of our study. Despite these encouraging results, several limitations should be acknowledged. This was a single-center study, and the absence of a control group treated with alternative fixation methods or fragment excision limits direct comparison with other treatment strategies [6,23]. In addition, long-term radiographic outcomes such as post-traumatic osteoarthritis or avascular necrosis were not the primary focus of this investigation. With a short duration of follow-up at 15.8 ± 3.2 months (range: 12–27 months), definitive remarks on avascular necrosis or post-traumatic arthritis cannot be made. Consecutive patients were included without randomization; selection bias cannot be ruled out. Future prospective, randomized, multicenter studies with longer follow-up periods are needed to establish the optimal management strategy for capitellum fractures. Nevertheless, the prospective design and use of validated outcome measures strengthen the evidence supporting the effectiveness of headless compression screw fixation for these injuries in our study.
ORIF of capitellar fractures with headless compression screws resulted in good functional outcomes, satisfactory elbow motion, and effective pain control in this cohort of 61 patients. Based on our prospective observations, headless compression screw fixation appears to offer a dependable method for achieving stable fixation and satisfactory functional recovery in displaced capitellar fractures.
Headless compression screws provide low-profile, cartilage-sparing fixation and a stable mechanical construct that supports early mobilization and restoration of good elbow function in capitellum fractures.
References
- 1. Bryan RS, Morrey BF. Fractures of the distal humerus. In: Morrey BF, editor. The Elbow and its Disorders. 3rd ed. Philadelphia, PA: WB Saunders; 2000. p. 325-33. [Google Scholar] [PubMed]
- 2. Ring D, Jupiter JB. Fractures of the distal humerus. Orthop Clin North Am 2000;31:103-13. [Google Scholar] [PubMed]
- 3. McKee MD, Jupiter JB, Bamberger HB. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 1996;78:49-54. [Google Scholar] [PubMed]
- 4. Dubberley JH, Faber KJ, MacDermid JC, Patterson SD, King GJ. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 2006;88:46-54. [Google Scholar] [PubMed]
- 5. Ring D. Fractures of the capitellum and trochlea. J Hand Surg Am 2009;34:1589-92. [Google Scholar] [PubMed]
- 6. Duckworth AD, McQueen MM, Ring D. Fractures of the capitellum: A systematic review. J Hand Surg Am 2012;37:1739-44. [Google Scholar] [PubMed]
- 7. Herbert TJ, Fisher WE. Management of the fractured scaphoid using a new bone screw. J Bone Joint Surg Br 1984;66:114-23. [Google Scholar] [PubMed]
- 8. Mighell MA, Harkins D, Klein D, Schneider S, Frankle M. Technique for internal fixation of capitellum and lateral trochlea fractures. J Orthop Trauma 2006;20:699-704. [Google Scholar] [PubMed]
- 9. Ruchelsman DE, Tejwani NC, Kwon YW, Egol KA. Open reduction and internal fixation of capitellar fractures with headless screws. Surgical technique. J Bone Joint Surg Am 2008;90:132-8. [Google Scholar] [PubMed]
- 10. Sen MK, Sama N, Helfet DL. Open reduction and internal fixation of capitellar fractures. J Orthop Trauma 2007;21:565-9. [Google Scholar] [PubMed]
- 11. Ring D, Jupiter JB, Gulotta L. Articular fractures of the distal humerus. Instr Course Lect 2003;52:373-81. [Google Scholar] [PubMed]
- 12. Doornberg JN, Ring D. Open reduction and internal fixation of coronal shear fractures of the distal humerus. J Orthop Trauma 2006;20:570-5. [Google Scholar] [PubMed]
- 13. Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-7. [Google Scholar] [PubMed]
- 14. Lindenhovius AL, Jupiter JB. The posttraumatic stiff elbow: A review of the literature. J Hand Surg Am 2007;32:1605-23. [Google Scholar] [PubMed]
- 15. Dawson J, Doll H, Boller I, Fitzpatrick R, Little C, Rees J, et al. The development and validation of a patient-reported questionnaire to assess outcomes of elbow surgery. J Bone Joint Surg Br 2008;90:466-73. [Google Scholar] [PubMed]
- 16. McKee MD, Schemitsch EH, Sala MJ. Fractures of the capitellum. Orthop Clin North Am 1999;30:99-109. [Google Scholar] [PubMed]
- 17. Athwal GS, Faber KJ, King GJ. Complications of plate fixation of elbow fractures. J Am Acad Orthop Surg 2011;19:554-62. [Google Scholar] [PubMed]
- 18. Robinson CM, Hill RM, Jacobs N, Dall G, Court-Brown CM. Adult distal humeral metaphyseal fractures: Epidemiology and results of treatment. J Orthop Trauma 2003;17:38-47. [Google Scholar] [PubMed]
- 19. Mighell MA, Frankle MA. Fractures of the capitellum and trochlea. J Am Acad Orthop Surg 2010;18:327-336. [Google Scholar] [PubMed]
- 20. Poynton AR, Kelly IP, O’Rourke SK. Fractures of the capitellum–a comparison of two fixation methods. Injury 1998;29:341-3. [Google Scholar] [PubMed]
- 21. Sultan A, Khursheed O, Bhat MR, Kotwal HA, Manzoor QW. Management of capitellar fractures with open reduction and internal fixation using herbert screws. Ulus Travma Acil Cerrahi Derg 2017;23:507-14. [Google Scholar] [PubMed]
- 22. Nolte PC, Midtgaard K, Miles JW, Tanghe KK, Provencher MT. The effect of buttress plating on biomechanical stability of coronal shear fractures of the capitellum: A cadaveric study. J Hand Surg Am 2023;48:621.e1-7. [Google Scholar] [PubMed]
- 23. Ring D, Jupiter JB. Surgical exposure of coronal shear fractures of the distal humerus. J Orthop Trauma 2002;16:638-43. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Acute Capitellum Fracture with Distal Radio-ulnar Joint Disruption: An Atypical Variant of an Essex Lopresti Injury – Case Report
June 1, 2026 Acute Capitellum Fracture with Distal Radio-ulnar Joint Disruption: An Atypical Variant of an Essex Lopresti Injury – Case Report May 1, 2026 Operative Management of a Late-Presenting McKee Type IV Capitellum Coronal Shear Fracture via an Anterolateral Approach: A Rare Case Report
May 1, 2026 Operative Management of a Late-Presenting McKee Type IV Capitellum Coronal Shear Fracture via an Anterolateral Approach: A Rare Case Report March 10, 2021 Spontaneous Early Intraprosthetic Dislocation of 22 mm Skirted Femoral Head in Dual Mobility Hip Prosthesis: A Case Report
March 10, 2021 Spontaneous Early Intraprosthetic Dislocation of 22 mm Skirted Femoral Head in Dual Mobility Hip Prosthesis: A Case Report July 30, 2019 Surgical Technique: Repair of Patella Tendon Rupture in a Previously Harvested Tendon for an Anterior Cruciate Ligament Reconstruction
July 30, 2019 Surgical Technique: Repair of Patella Tendon Rupture in a Previously Harvested Tendon for an Anterior Cruciate Ligament Reconstruction