
This study highlights that physiotherapeutic modality i.e. transcutaneous electrical nerve stimulation (TENS) and neural mobilization both are helpful in treating cervical radiculopathy.
Miss. Sadhana Tiwari, Research Scholar, Department of Physiotherapy, Nims University, Jaipur, Rajasthan, India. E-mail: sadhanatphysio@yahoo.com
Abstract
Introduction: As we know that there are many complaints regarding cervical radiculopathy (CR) coming up nowadays. CR has many more causes, such as poor posture, screen time, prolong working duration on computer system, high pillow, sudden jerk, etc. Along with the above-mentioned causes physical activity also influences the CR cases. Lack of physical activity reduces the strength of the surrounding muscle which increases the chances for CR. A person with regular physical activity has less-chances of such conditions.
Objectives: To unlock the effects of neural mobilization (NM) versus transcutaneous electrical nerve stimulation (TENS) in CR.
Materials and Methods: Total 30 patients were selected and divided into two groups randomly. Patients were informed about the study and one group was treated with TENS and the other group was treated with NM. Two outcome measures were used to assess the pain and neck pain disability.
Results: The result of the study has shown the difference between pre- and post-treatment but the NM (Median Nerve Mobilization [ULTT 1]; Median Nerve Mobilization [ULTT 2A]; Radial Nerve Mobilization [ULTT 2B]; Ulnar Nerve Mobilization [ULTT 3]) and TENS (Conventional/Continuous Mode) are equally effective in CR patients (P <0.05).
Conclusion: The study concluded that NM and TENS are equally effective in CR.
Keywords: Transcutaneous electrical nerve stimulation, Numeric Pain Rating Scale, neural mobilization, cervical radiculopathy, upper limb tissue tension, neck disability index.
The human body spinal column is divided into several segments, such as Cervical, Thoracic, lumbar, Sacral and coccyx bone. Each segment distributes the spinal nerve bilaterally and an impingement of spinal nerve due to any reason gives the symptoms, such as radiation of pain in bilateral or unilateral upper limb is a very common pattern/nature of cervical radiculopathy (CR). This pain can radiate from the nape of neck to till tip off the fingers. With increasing sedentary lifestyles and computer-dependent occupations, the incidence of CR has been rising [1]. CR is a condition characterized by compression at cervical nerve roots and its branches, resulting in pain, numbness, tingling, or motor weakness radiating from the neck into the upper extremity. The condition significantly affects the “quality of life” and “functional capacity” of affected individuals in middle to older age groups [1,2,3]. Concurrently, inflammatory mediators such “tumor necrosis factor-alpha” and “interleukins” increase neuronal irritation and pain sensitivity [3]. Management strategies are both conservative and surgical, depending on the severity and duration of symptoms. Conservative treatment, such as physiotherapy, neural mobilization (NM), isometric neck exercises, and “Transcutaneous Electrical Nerve Stimulation” remains the first line of management in most cases [4,5]. Numerous studies have demonstrated that NM can reduce pain, enhance range of motion, improve nerve conduction, and restore functional activity. It has also been shown to complement other physiotherapeutic modalities, such as isometric strengthening, traction, and transcutaneous electrical nerve stimulation (TENS). The non-invasive and patient-specific nature of NM makes it a safe and effective intervention, particularly in conservative management of radiculopathies and peripheral nerve entrapment syndromes [6,7]. CR can greatly interfere with daily activities, occupational performance, and overall quality of life. Physiotherapy is essential in the conservative treatment of CR, and commonly used interventions include NM and electrotherapy techniques [8,9,10]. NM focuses on restoring normal nerve mobility and physiological function, which helps reduce neural mechanosensitivity and alleviate symptoms. In contrast, TENS is widely used to manage pain through neuromodulation. Although both approaches are frequently used in clinical settings, there is limited comparative research evaluating their effectiveness in reducing pain, improving functional ability, and supporting recovery in individuals with CR [11,12,13,14]. Therefore, this study aims to assess and compare the effects of NM and TENS, which may assist physiotherapists in determining the more effective treatment and improving therapeutic strategies for better patient outcomes.
Research design
Prospective comparative study.
Sample size
Total 30 patients with clinically and radiographically confirmed CR were recruited from physiotherapy outpatient department (OPD) at Nims Hospital using purposive sampling. A written consent form was obtained from all patients before enrolment. The study was approved from Institutional Ethical committee.
Study setting
A comparative study was conducted in OPD of the physiotherapy department at Nims Hospital.
Inclusion criteria
- Patients of all genders between 20 and 40 years of age
- Patient suffering from pain since a month
- Diagnosed case of CR by a Physiotherapist.
Exclusion criteria
- Patients undergone any surgical procedure near the neck
- Patients on painkillers, muscle relaxants
- Patients suffering from a neurological condition.
Outcome measure
- “Neck Disability Index” (NDI)
- “Numeric Pain Rating Scale” (NPRS)
Procedure
The patients were selected and divided into two groups. A detail explanation about the study and the procedure was explained to all the patients. Patients were explained about their valuable or genuine feedback. Patients were also explained about the 2 scale which they need to fill before starting treatment, i.e., day 1 and after 2 weeks, i.e., day 14 post-treatment. All the patients were given assistance for understanding both the scales whenever needed. Both the groups were as follows:
- Group A (n = 15): The most popular TENS mode is the conventional or continuous mode. It can be used both in the acute and chronic stages of pain. Large Aβ diameter fiber activity inhibits pain fibers, which modulates pain. Pain alleviation comes on quickly. The stimulation parameters include a low intensity (12–30 mA) that produces paresthesia and a pleasant tingling feeling without causing any muscular contraction. A high frequency, usually between 100 and 150 Hz. The typical pulse duration is between 50 and 80 µs. Treatment lasts 20–60 min.
- Group B (n = 15): The targeted NM was given to Median Nerve Mobilization (ULTT 1); Median Nerve Mobilization (ULTT 2A); Radial Nerve Mobilization (ULTT 2B); Ulnar Nerve Mobilization (ULTT 3). Each NM was given 10 time per session.
Data analysis
Data were analyzed by using “Statistical Package for the Social Sciences software version 25.0.”
The mean value of 30 patients was 36.50 and standard deviation (SD) is 2.837 in Group A while in Group B the mean value is 34.56 and SD is 4.43.
Group – A
The mean value of NDI pre is 48.93 and SD is 3.22 while NDI post-mean value is 6.33 and SD is 1.29. The mean value of NPRS pre is 6.66 and SD is 1.24 while NPRS post-mean value is .63 and SD is 0.718.
NDI
Paired “t”-test was conducted to compare with the pre and post-value of NDI in CR pts. A significant difference in the NDI Pre (M = 42.60, SD = 3.644), t = 64.02, P = 0.000 (<0.05). It shows positive effect. As mentioned in Table – 1, Graph 1
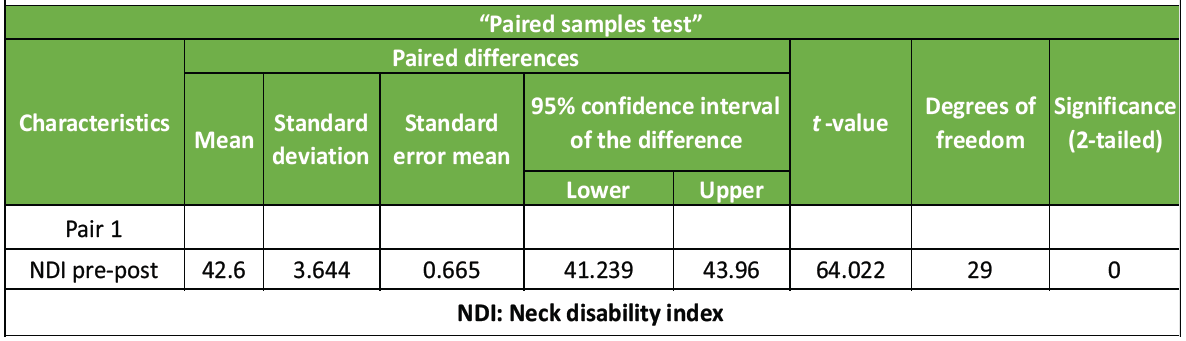
Table 1: Paired sample t-test for NDI (Pre-Post)
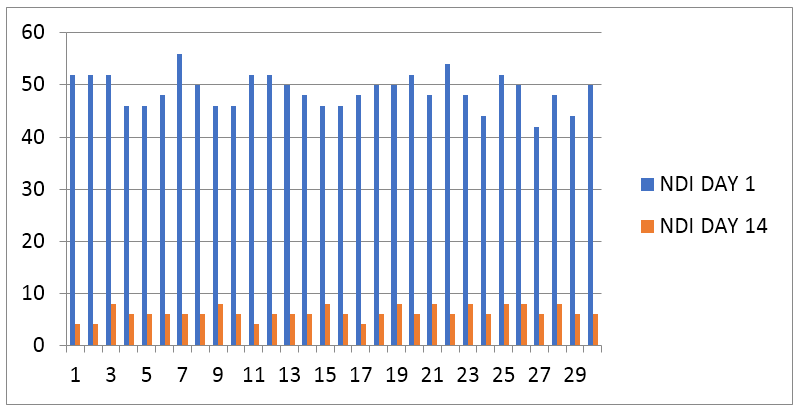
Graph 1: Graphical representation of neck disability index (NDI) pre and post (X = Number of pts, Y = NDI scale).
NPRS
Paired “t”-test was conducted to compare the pre– and post-value of NPRS in CR pts. A significant difference in the NPRS Pre Post(M = 6033, SD = 1.40), t = 23.57, P = 0.000 (<0.05). It shows positive effect. As mentioned in Table – 2, Graph 2
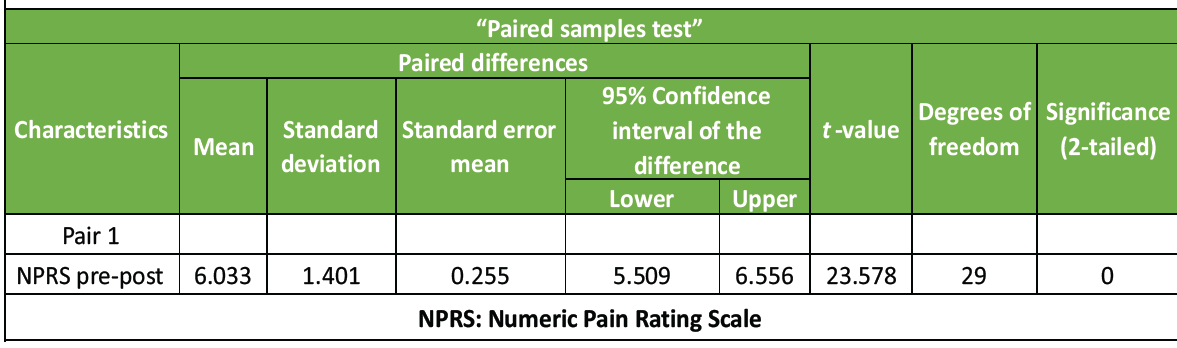
Table 2: Paired sample “t”-test for NPRS (Pre-Post)
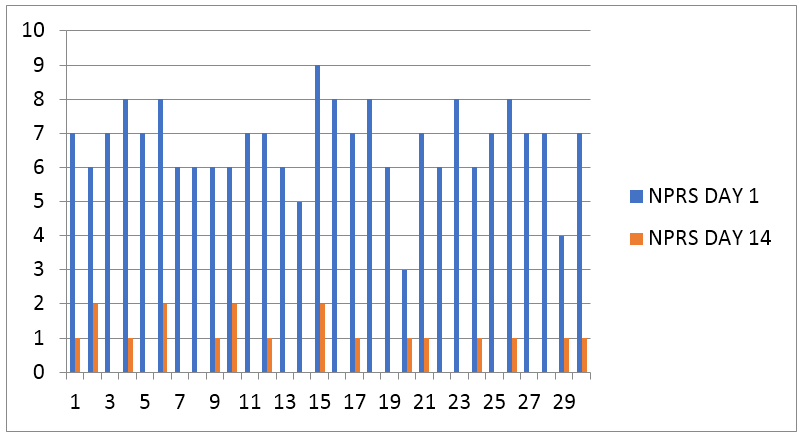
Graph 2: Graphical representation of numeric pain rating scale (NPRS) pre and post (X = Number of pts, Y = NPRS scale).
Group – B
The Mean value of NDI pre is 49.26 and SD is 3.50 while NDI post-Mean value is 5.66 and SD is 1.29. The Mean value of NPRS pre is 6.43 and SD is 1.30 while NPRS post-Mean value is .23 and SD is 0.43.
NDI
Paired t-test was conducted to compare the pre- and post-value of NDI in CR pts. A significant difference in the NDI Pre (M = 43.60, SD = 3.420), t = 69.82, P = 0.000 (<0.05). It shows positive effect. As mentioned in Table – 3, Graph 3
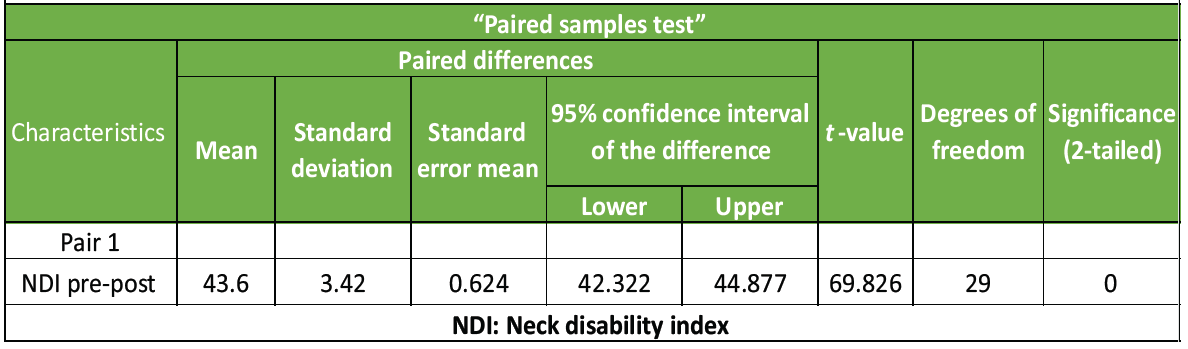
Table 3: Paired sample “t”-test for NDI (Pre-Post)
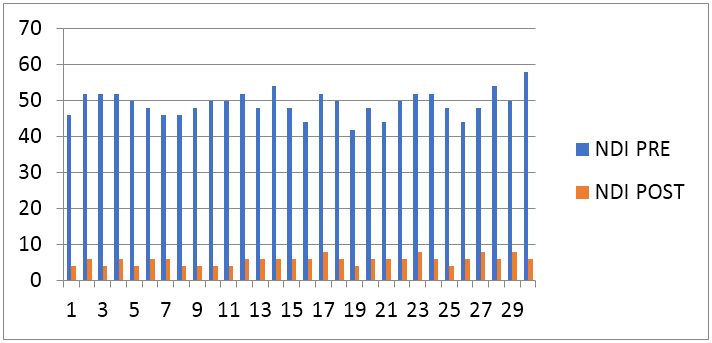
Graph 3: Graphical representation of neck disability index (NDI) pre and post (X = Number of pts, Y = NDI scale).
NPRS
A paired t-test was conducted to compare the pre- and post-value of NPRS in CR pts. There was a significant difference in the NPRS Pre (M = 6.20, SD = 1.29),. t = 26.17, P = 0.000 (<0.05). It shows positive effect. As mentioned in Table – 4, Graph 4
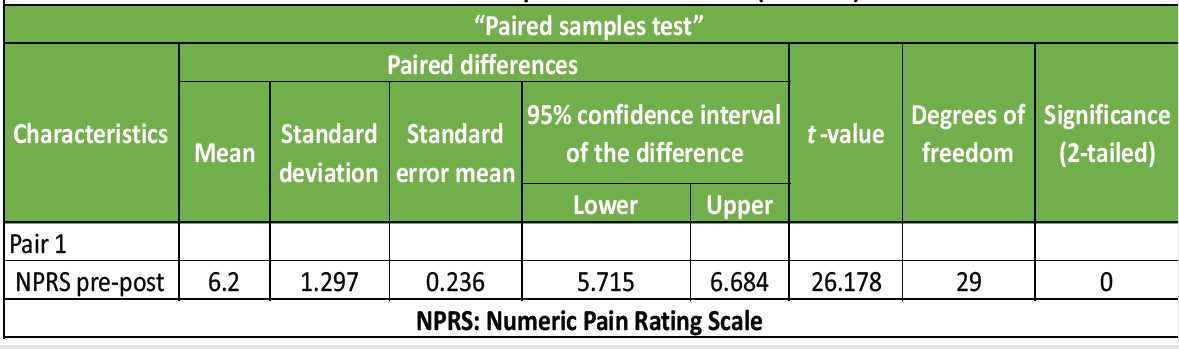
Table 4: Paired sample “t” test for NPRS (Pre-Post)
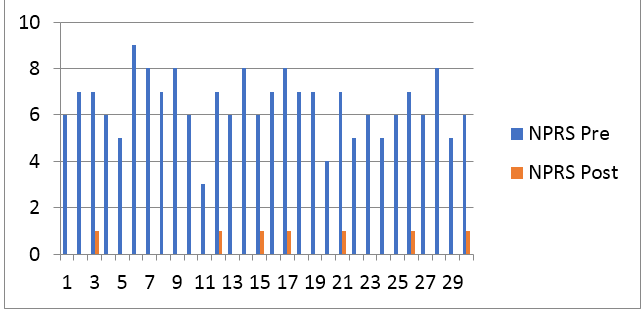
Graph 4: Graphical representation of numeric pain rating scale (NPRS) pre and post (X = Number of pts, Y = NDI scale).
The “t” value of NDI is −1.09 and P = 0.13; t-value of NPRS is −0.47 and P-value is 0.31. P < 0.05 so, the null-hypothesis is accepted, and hence proved that NM and TENS are equally effective in CR patients.
The present study was carried out to compare the effects of NM and TENS in individuals with CR. The results indicated that both treatment approaches were effective in decreasing pain and improving functional outcomes in patients with this condition. The findings further confirm the effectiveness of both TENS and NM in the treatment of CR. Each technique contributes to pain relief and functional recovery through different mechanisms. TENS mainly works through pain modulation by stimulating large-diameter afferent nerve fibers and inhibiting nociceptive signals at the spinal cord level according to the Gate Control Theory. In addition, it promotes the release of endogenous opioids, which helps in reducing the perception of pain. In contrast, NM aims to restore normal nerve mobility and physiological functioning by enhancing the extensibility of neural tissues, reducing neural mechanosensitivity, and improving intraneural blood circulation. A study by Pallewar et al. [11] involving 60 participants showed that NM combined with mechanical cervical traction was effective in reducing pain and improving functional status in patients with CR. The outcomes of the present study are consistent with Pallewar’s findings, which emphasize the importance of NM in relieving symptoms related to nerve root compression and promoting functional recovery. Similarly, Nelakurthy et al. [12] conducted research on 30 patients experiencing cervicobrachial pain using NM techniques. The study concluded that NM along with conventional physiotherapy significantly reduced pain and improved cervical mobility. The results of the present study support Nelakurthy’s conclusions, indicating that NM plays an important role in the physiotherapy management of CR. Another investigation by Cleland et al. [15] evaluated the effectiveness of manual therapy and exercise in individuals with CR and reported considerable improvements in pain and disability. The study emphasized that treatments addressing neural and mechanical dysfunction can substantially reduce symptoms. The present study aligns with these findings, suggesting that interventions focused on improving neural tissue mobility can enhance treatment outcomes. Similarly, Young et al. [16] conducted a randomized clinical trial examining the effects of manual therapy, exercise, and cervical traction in patients with CR. The results demonstrated significant reductions in both pain and disability following conservative physiotherapy management. These findings further support the value of non-invasive physiotherapy interventions, such as NM, in improving patient outcomes. In addition, Butler [17] and Shacklock [18] highlighted that NM techniques help restore the dynamic interaction between neural tissues and surrounding structures. These methods reduce nerve sensitivity and improve nerve gliding, which can help alleviate symptoms, such as radiating pain, numbness, and tingling commonly seen in CR. TENS is also widely used as a supportive modality for pain management in both musculoskeletal and neuropathic conditions. Various studies have reported that TENS effectively decreases pain intensity by modulating nociceptive signals and stimulating the release of endorphins. In individuals with CR, the pain relief achieved through TENS may enable better participation in therapeutic exercises and functional rehabilitation. Overall, the results of this study suggest that both NM and TENS are effective interventions in the conservative treatment of CR.
Limitations
This study has some limitations that should be taken into account when interpreting its findings. The relatively small sample size may limit the ability to generalize the results to the broader population of individuals with CR. In addition, the intervention period was short, and no long-term follow-up was performed to evaluate the lasting effects of NM and TENS.
Recommendations
- Implementation of both methods in clinical practice to treat CR.
- Awareness campaigns on early diagnosis of neck with CR for better outcome.
- Regular physical activity posture awareness.
This research showed the equally positive results in both the groups. Patients in the Group A was treated by using TENS (Conventional/Continuous Mode) and patients in the Group B was treated by using NM (Median Nerve Mobilization [ULTT 1]; Median Nerve Mobilization [ULTT 2A]; Radial Nerve Mobilization [ULTT 2B]; Ulnar Nerve Mobilization [ULTT 3]). Patient’s feedback from both groups on 14th day has shown the equal effect. So, this study concluded that TENS and NM can be an equally effective therapeutic approach to treat CR.
This study highlights that neural mobilization and transcutaneous electrical nerve stimulation both the therapeutic modalities are helpful in reducing the pain caused by Physical Factors.
References
- 1. Peolsson A, Peterson G, Hermansen A, Ludvigsson ML, Dedering Å, Löfgren H. Physiotherapy after anterior cervical spine surgery for cervical disc disease: Study protocol of a prospective randomised study to compare internet-based neck-specific exercise with prescribed physical activity. BMJ Open 2019;9:e027387. [Google Scholar] [PubMed]
- 2. Hassan KZ, Sherman AL. Epidural steroids. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 3. Doughty CT, Bowley MP. Entrapment neuropathies of the upper extremity. Med Clin North Am 2019;103:357-70. [Google Scholar] [PubMed]
- 4. Abbott JH, Schmitt J. Minimum important differences for the patient-specific functional scale, 4 region-specific outcome measures, and the numeric pain rating scale. J Orthop Sports Phys Ther 2014;44:560-4. [Google Scholar] [PubMed]
- 5. Akalin E, El Ö, Peker Ö, Senocak O, Tamci S, Gülbahar S, et al. Treatment of carpal tunnel syndrome with nerve and tendon gliding exercises. Am J Phys Med Rehabil 2002;81:108-13. [Google Scholar] [PubMed]
- 6. Gupta R, Sharma S. Effectiveness of median nerve slider’s neurodynamics for managing pain and disability in cervicobrachial pain syndrome. Indian J Physiother Occup Ther 2012;6:127-32. [Google Scholar] [PubMed]
- 7. Coppieters MW, Nee R. Neurodynamic management of the peripheral nervous system. In: Grieve’s Modern Musculoskeletal Physiotherapy. 4th ed. Edinburgh, UK: Elsevier; 2015. p. 287-97. [Google Scholar] [PubMed]
- 8. Jain P, Saharan AK, Vishnoi CS, Bhati MP, Sharma P. Single IASTM and cupping therapy session improves pain and disability in patients with non-specific low back pain. GSC Adv Res Rev 2022;11:45-50. [Google Scholar] [PubMed]
- 9. Kazi MN, Jain DC, Ramaligam T, Taneja D, Saharan M. Frequency of foot pain and its interrelation with footwear among female participants in Surat district. 2022;12;3. [Google Scholar] [PubMed]
- 10. Goel V, , Saharan AK, Saharan M, Taneja D, Sharma S, Comparison of clinical effectiveness of conventional physiotherapeutic techniques versus advanced programmed based electrotherapeutic interventions on chronic lumbar discogenic radiculitis. Int J Health Sci Res 2023;13(12):187-198. [Google Scholar] [PubMed]
- 11. Pallewar M, Kumar Saharan A, Gouru V. The effect of neural mobilization with cervical traction in cervical radiculopathy patients. Int J Dev Res 2021;11:45913-7. [Google Scholar] [PubMed]
- 12. Nelakurthy S, Saharan M, Kushma P, kumar Saharan A. A comparative study to evaluate the effectiveness of conventional therapy alone and combined with neural mobilization in patients with cervicobrachial pain. Pramana Res J 2020;10:116-27. [Google Scholar] [PubMed]
- 13. Taneja DD, Saharan DA, Mathur DM. Effect of spinal mobilization with arm movement in the treatment of cervicobrachial pain syndrome. Int J Dev Res 2018;8:18589-94. [Google Scholar] [PubMed]
- 14. Swaminathan G, Muralidharan V, Joseph BV. Clinical spectrum and importance of evaluation systems in degenerative cervical myeloradiculopathy. Indian Spine J 2019;2:13-9. [Google Scholar] [PubMed]
- 15. Cleland JA, Whitman JM, Fritz JM, Palmer JA. Manual physical therapy, cervical traction, and strengthening exercises in patients with cervical radiculopathy: A case series. J Orthop Sports Phys Ther 2005;35:802-11. [Google Scholar] [PubMed]
- 16. Young IA, Cleland JA, Michener LA, Aguilera AJ, Snyder AR. Manual therapy, exercise, and traction for patients with cervical radiculopathy: A randomized clinical trial. Phys Ther 2009;89:632-42. [Google Scholar] [PubMed]
- 17. Butler DS. The Sensitive Nervous System. Adelaide: Noigroup Publications; 2000. [Google Scholar] [PubMed]
- 18. Shacklock M. Clinical Neurodynamics: A New System of Musculoskeletal Treatment. Edinburgh: Elsevier Butterworth-Heinemann; 2005. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Comparative Effects of Therapeutic Exercise versus Muscle Energy Technique Combined with Transcutaneous Electrical Nerve Stimulation on Pain, Range of Motion, and Functional Outcomes after Anterior Cruciate Ligament Reconstruction: A Prospective Pilot Study
May 1, 2026 Comparative Effects of Therapeutic Exercise versus Muscle Energy Technique Combined with Transcutaneous Electrical Nerve Stimulation on Pain, Range of Motion, and Functional Outcomes after Anterior Cruciate Ligament Reconstruction: A Prospective Pilot Study April 1, 2026 Anterior Cervical Discectomy and Fusion with Polyetheretherketone Cage or Anterior Cervical Plate: A Comparative Evaluation of Short-term Outcomes
April 1, 2026 Anterior Cervical Discectomy and Fusion with Polyetheretherketone Cage or Anterior Cervical Plate: A Comparative Evaluation of Short-term Outcomes April 1, 2026 Arthroscopic Management of a Bucket-Handle Acetabular Labral Tear in a Pediatric Patient: A Rare Case Report with Associated Fleck Sign
April 1, 2026 Arthroscopic Management of a Bucket-Handle Acetabular Labral Tear in a Pediatric Patient: A Rare Case Report with Associated Fleck Sign April 20, 2015 Arthroscopy Assisted Percutaneous Fixation of Ideberg Type Iii Glenoid Fractures
April 20, 2015 Arthroscopy Assisted Percutaneous Fixation of Ideberg Type Iii Glenoid Fractures