
Total hip arthroplasty offers comparable early pain relief and functional recovery at 3 months for traumatic femoral neck fractures and non-traumatic hip pathologies. Surgeons should anticipate a higher risk of intraoperative periprosthetic fracture in older patients and optimise femoral preparation accordingly.
Dr. Deepak Ranjan Patro, Department of Trauma and Emergency (Orthopaedics), All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. E-mail: drp8855@gmail.com
Abstract
Introduction: Total hip arthroplasty (THA) is an established procedure for pain relief and functional restoration in both traumatic and non-traumatic hip pathologies, yet comparative data from the Indian population remain limited. This prospective study aimed to compare intraoperative parameters, early post-operative course, and 3-month functional outcomes of THA performed for traumatic femoral neck fractures versus heterogeneous non-traumatic etiologies in an Eastern Indian tertiary care centre.
Material and Methods: This single-centre, prospective comparative study was conducted at All India Institute of Medical Sciences (AIIMS) Bhubaneswar between January 2021 and December 2022, after obtaining approval from the Institutional Ethics Committee, vide reference number (IEC/AIIMS BBSR/PG Thesis/2020–21/82). Forty-eight patients aged 30–70 were enrolled and divided into Group A (traumatic femoral neck fractures, n = 24) and Group B (non-traumatic etiologies, n = 24). All procedures were performed by a single surgeon using a standardised modified Hardinge approach with uncemented components. Key endpoints included the modified Harris hip score (MHHS) and the Visual Analog Scale (VAS) for pain at 3 months, along with intraoperative parameters and early post-operative complications.
Results: Forty-eight patients were analyzed (24 traumatic, 24 non-traumatic), with the traumatic group significantly older than the non-traumatic group (55.17 versus 41.63 years, P < 0.001). Intraoperative surgical time, blood loss, need for transfusion, and early post-operative indices, including drain output, length of stay, and serial VAS scores, showed no significant differences between groups (all P > 0.05). Two intraoperative periprosthetic femoral fractures (8.3%) occurred in the traumatic group and none in the non-traumatic group, while at 3 months, MHHS (65.75 vs. 69.96, P = 0.11), VAS, gait parameters, use of walking aids, and sit-to-stand time were comparable, with no dislocations, deep infections, loosening, or revisions in either group.
Conclusion: THA provided similar early pain relief and functional recovery at 3 months for both traumatic femoral neck fractures and non-traumatic hip pathologies in this Eastern Indian cohort. Although the older traumatic group demonstrated a higher, clinically relevant but statistically insignificant rate of intraoperative periprosthetic fractures, overall early complication profiles and functional outcomes were comparable, supporting THA as a reliable option for both indications while underscoring the need for careful femoral preparation in older fracture patients and for longer-term studies with larger, matched cohorts to evaluate implant survivorship and late complications.
Keywords: Total hip arthroplasty, femoral neck fracture, non-traumatic hip pathology, functional outcomes.
Total hip arthroplasty (THA) is a highly successful and reliable surgical procedure for restoring function and relieving pain in both traumatic and non-traumatic hip pathologies. As global life expectancy rises, the incidence of femoral neck fractures and demand for THA are also increasing. Displaced femoral neck fractures carry high rates of morbidity and mortality, leading many clinicians to favour THA, especially in active older adults, due to superior functional outcomes over hemi arthroplasty [1,2,3,4,5,6,7]. Beyond trauma, non-traumatic etiologies – including osteonecrosis, osteoarthritis (OA), and inflammatory arthritis – commonly require arthroplasty, with optimal results reported across diverse patient groups [8,9,10,11].
However, direct comparisons of THA outcomes for traumatic versus non-traumatic indications reveal conflicting evidence. Some studies indicate greater intraoperative and postoperative complications, blood loss, and longer hospital stays for trauma cases [12,13,14], while others report comparable or even equivalent short-term and long-term outcomes in functional recovery, implant survivorship, and complication rates [15,16]. Most comparative data originate from Western cohorts where the non-traumatic cohort is typically older and dominated by primary OA. Indian studies remain sparse, and population-specific differences are underreported. In this demographic, the non-traumatic cohort is often younger and more commonly presents with etiologies, such as osteonecrosis, post-infectious sequelae, or inflammatory arthritis, which differ significantly from primary OA. To our knowledge, no study to date has prospectively evaluated these outcomes in an Eastern Indian population.
This study aims to prospectively evaluate and compare the intraoperative, early post-operative, and 3-month functional outcomes of THA performed for traumatic versus non-traumatic hip pathologies in an Eastern Indian cohort. We aim to provide data to refine patient counselling, surgical planning, and post-operative management strategies in Indian healthcare settings.
Study design and setting
This was a single-centre, prospective, comparative study conducted in the Department of Orthopaedics at the All India Institute of Medical Sciences (AIIMS), Bhubaneswar, India, between January 2021 and December 2022, with Institutional Ethics Committee approval, vide reference number (IEC/AIIMS BBSR/PG Thesis/2020-21/82).
Inclusion and exclusion criteria
Inclusion
Patients aged 30–70 years undergoing primary THA for either traumatic femoral neck fracture (Group A) or non-traumatic etiologies (Group B: Primary OA, avascular necrosis, inflammatory arthritis, post-traumatic arthritis, congenital disorders, or hip fusion).
Exclusion
Acute hip infection, revision arthroplasty, tumor, bilateral THA, unwillingness to provide informed consent, or body mass index >30.
Sample size
The sample size was determined using the two-proportion difference formula, referencing data from Agarwal et al. Assuming a risk difference of 0.16 (proportion of success in Group A = 0.84, Group B = 0.68), with a desired confidence level of 95% and accounting for an anticipated 10% loss to follow-up, the minimum required sample size was calculated to be 24 participants per Group [17].
Surgical technique and perioperative care
All procedures were performed by a single senior surgeon under spinal anaesthesia, utilising a standardised modified Hardinge (anterolateral) approach to minimise technical variability.
The approach involved an incision over the greater trochanter, followed by an incision of the tensor fascia lata (TFL). The TFL was retracted anteriorly and the gluteus maximus posteriorly. The gluteus medius was split in line with its fibres, with the incision limited to 5 cm proximal to the greater trochanter to protect the superior gluteal neurovascular bundle. The gluteus minimus and a portion of the vastus lateralis were elevated as a single sleeve from the anterior trochanter. A “T”-shaped capsulotomy was performed to expose the femoral head and neck. The femoral head was dislocated, or in cases of fusion (e.g., ankylosing spondylitis), an in situ neck cut was performed. The acetabulum was sequentially reamed, and uncemented components were implanted after trialing for stability, version, and limb length. Femoral preparation and implantation were followed. Stability was reassessed, and routine closure was performed. All patients received a standardised post-operative protocol, including five days of intravenous antibiotics and multimodal analgesia. Supervised physiotherapy was initiated on post-operative day 2, with appropriate precautions for dislocation. Mobilisation was directed by the chief surgeon based on intraoperative findings and patient stability.
Data collection and outcomes
Data were captured in a structured pro forma. Key endpoints included:
- Primary outcome: Modified Harris hip score (MHHS) and Visual Analog Scale (VAS) for pain at 3 months post-operatively.
- Secondary outcomes:
- Intra-operative parameters: Surgical time (incision to closure), estimated blood loss, need for blood transfusion, any additional surgical procedures (e.g., tenotomy, osteotomy), and intra-operative complications (e.g., periprosthetic fracture).
- Early post-operative parameters (within 5 days): Surgical site infection (SSI), drain volume (bleeding), total length of hospital stay, and daily VAS pain scores.
- 3-month follow-up parameters: Clinical assessment for complications (infection, dislocation, limping, implant loosening, periprosthetic fracture), requirement for walking aids, and sit-to-stand time. Radiographs were obtained to assess implant position and fixation.
Statistical analysis
Data were entered into a Microsoft Excel spreadsheet and analysed using the Statistical Package for the Social SciencesStatistics for Windows, Version 25.0 (IBM Corp., Armonk, NY). The Shapiro–Wilk test was used to assess the normality of continuous data. Normally distributed continuous variables (e.g., age, surgical time) were presented as mean ± standard deviation and compared using the independent Student’s t-test. Non-normally distributed or skewed data (e.g., VAS scores, MHHS) were presented as medians (interquartile ranges) and compared using the Mann–Whitney U test. Categorical variables (e.g., gender, complications, need for transfusion) were presented as frequencies (n, %) and compared using the Chi-square test or Fisher’s exact test where cell counts were low. A P < 0.05 was considered statistically significant for all analyses.
Patient demographics and baseline characteristics
A total of 60 patients were screened for eligibility between January 2021 and December 2022. Twelve patients were excluded (unwillingness to participate). The remaining 48 patients were enrolled and allocated, with 24 patients in Group A (traumatic) and 24 in Group B (non-traumatic). The mean age of patients in Group A was 55.17 years, which was significantly greater than in Group B (41.63 years) (P < 0.001). The gender distribution was identical in both groups (16 male, 8 female). Group A consisted entirely of femoral neck fractures. Group B was heterogeneous, comprising osteonecrosis/avascular necrosis in 18 patients, ankylosing spondylitis in 5 patients, and sequelae of Perthes disease in 1 patient.
Intra-operative outcomes
There were no statistically significant differences between the two groups in terms of mean surgical time, mean estimated blood loss, or the proportion of patients requiring blood transfusions (P > 0.05 for all) (Table 1).
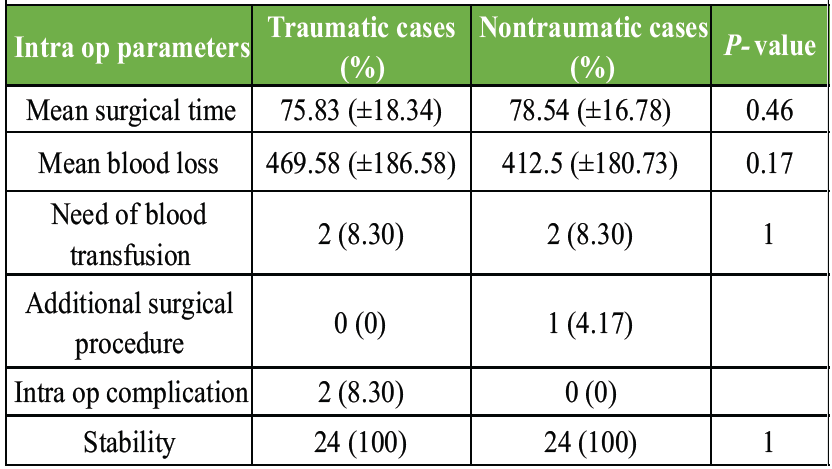
Table 1: Intra-operative parameters
Two intra-operative periprosthetic fractures (proximal femur) occurred in Group A (8.3%) during femoral broaching, which were managed with cerclage wiring. No intraoperative fractures occurred in Group B. One patient in Group B required an adductor tenotomy for contracture. This difference in intra-operative complications was not statistically significant (P = 0.488 by Fisher’s exact test).
Early post-operative and 3-month outcomes
No significant differences were observed in early post-operative parameters, including drain output, length of hospital stay, or VAS pain scores at 24 h, 48 h, or 5 days (P > 0.05 for all) (Table 2).
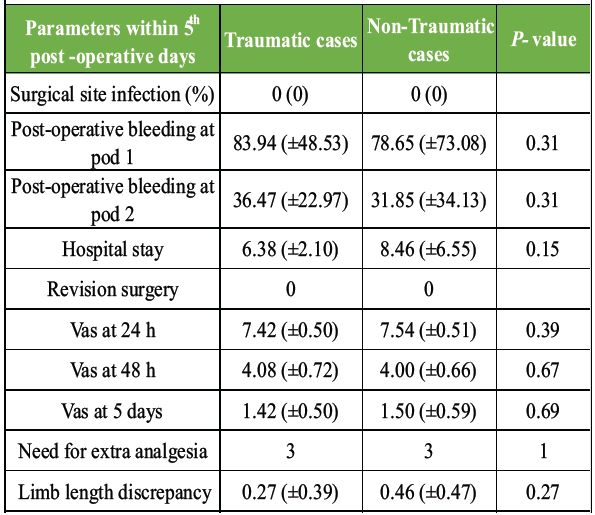
Table 2: Parameters within 5 post-operative days
One case of marginal skin necrosis (non-traumatic Group) was managed conservatively. No deep SSIs were noted in either Group within the 5-day period.
At the 3-month follow-up, no significant difference was found in the primary functional outcomes (Table 3).
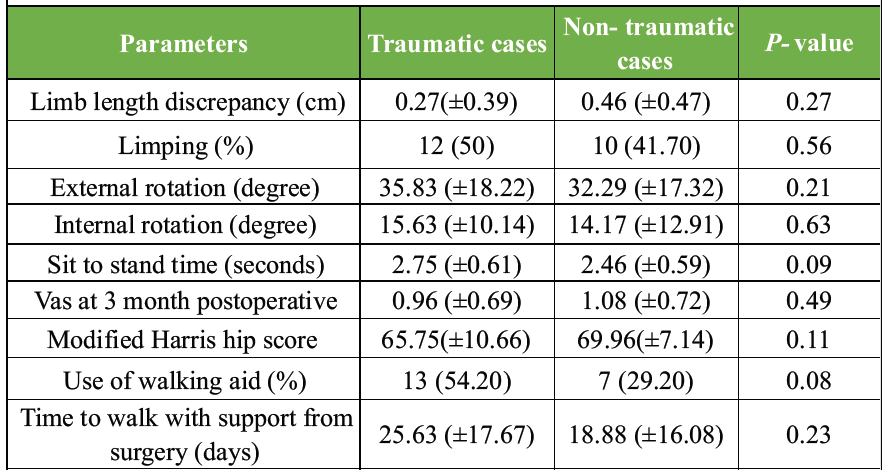
Table 3: Functional and clinical outcomes between 2 groups at 3 months post-operative follow-up
The mean MHHS was 65.75 in Group A and 69.96 in Group B (P = 0.11). The median VAS score at 3 months was also comparable (P > 0.05). No instances of revision surgery, dislocation, deep infection, or implant loosening were recorded in either Group at 3 months. There were no significant differences in limping, use of walking aids, sit-to-stand time, or leg length discrepancy.
The principal finding of this prospective study is that at 3 months post-surgery, patients undergoing THA for traumatic and non-traumatic hip pathologies achieve comparable early functional outcomes. This finding supports our initial hypothesis and aligns with the results of Abboud et al. and Lizaur-Utrilla et al., who also found no significant difference in functional outcomes between the fracture and elective cohorts [15,16]. Our results, however, contrast with several large registry studies that report poorer outcomes and higher complication rates in trauma patients [13,18]. This discrepancy may be multifactorial. Large registry studies often lack the granularity to account for surgical factors (e.g., single-surgeon consistency) or detailed patient-level factors. Furthermore, our study’s short follow-up period may obscure long-term differences. A key finding in our cohort was the non-significant (P = 0.488) but clinically notable trend of intraoperative complications in the trauma group. We observed two (8.3%) periprosthetic fractures in Group A, versus zero in Group B. This is likely attributable to the significant demographic difference we identified: The trauma group was, on average, 13.5 years older than the non-traumatic Group (P < 0.001). This older age is associated with a higher prevalence of osteoporosis, rendering the femur more susceptible to fracture during broaching [19]. This finding underscores the importance of meticulous femoral preparation, careful implant sizing, and readiness to deploy cerclage fixation when performing uncemented THA in older fracture patients [20,21].
A unique aspect of our study is the composition of the non-traumatic Group. Unlike in Western studies, where Group B would consist almost entirely of primary OA, our non-traumatic cohort was younger and dominated by osteonecrosis (75%) and inflammatory arthritis (21%). This demographic reality in the Eastern Indian population introduces a significant confounding variable. Osteonecrosis and ankylosing spondylitis (AS) are distinct pathologies from OA, with different patient profiles and prognoses. Studies have shown that THA in osteonecrosis patients may have higher rates of revision and complications than in OA patients [22], while AS patients may experience more blood loss and functional limitations [23]. Therefore, our “non-traumatic” Group is not a homogeneous control, which complicates direct comparison with other studies. The major strength of this study is its prospective, comparative design, which is a rarity on this topic within the Indian population. A uniform surgical approach, single-surgeon technique, and standardised perioperative protocol reduce variability related to surgeon experience, implant selection, and rehabilitation regimens. This study has several important limitations. The follow-up duration of 3 months is sufficient to capture early functional recovery and acute complications, but is inadequate for assessing long-term outcomes, such as aseptic loosening, late infection, or implant survivorship. The “excellent” survivorship found in our study (no loosening or revision) is due to this short duration of follow-up and not indicative of long-term success. As discussed, the non-traumatic group was highly heterogeneous, and the two groups were not matched for age. This baseline demographic difference (age) is a major confounder that likely influenced the intraoperative fracture rate. Small sample size
Although powered to detect a difference in MHHS, our sample size (n = 48) is too small to draw firm conclusions about complication rates. The study is underpowered to detect a statistically significant difference in rare events, such as fractures or dislocations. The lack of a significant difference in complications should be interpreted with caution. This study, to our knowledge, is the first prospective comparison of its kind in an Eastern Indian population. The findings suggest that despite demographic differences and intraoperative challenges, the early functional recovery trajectory is similar for both groups. This information is valuable for clinicians in counselling patients and managing expectations.
THA provides excellent and comparable early functional outcomes and pain relief at 3 months for patients with both traumatic and non-traumatic hip pathologies. In our cohort, the traumatic Group was significantly older and experienced a higher (though not statistically significant) rate of intra-operative periprosthetic fractures, likely related to poorer bone quality. The early functional parity suggests that THA is a reliable procedure for both indications. However, these findings must be interpreted with caution, given the study’s significant limitations, including the short follow-up period, small sample size, and heterogeneous nature of the non-traumatic cohort. Further research with larger, matched cohorts and long-term follow-up is necessary to confirm these results and assess implant survivorship.
THA can be confidently done in both traumatic and non-traumatic hip pathologies. Heightened intraoperative vigilance and careful femur medullary canal preparation are needed in old trauma patients.
References
- 1. Cahyadi NI, Steven P. Outcome of total hip arthroplasty versus hip hemiarthroplasty for femoral neck fractures in the elderly: A meta-analysis of randomized control trial. Int Surg J 2024;11:2063-9. [Google Scholar] [PubMed]
- 2. Falotico GG, Matsunaga FT, Filho JS, Moraes VY, Garcia MS, Faloppa F, et al. Total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fracture: An overview of systematic reviews total hip arthroplasty versus hemiarthroplasty for displaced femoral neck fracture: An overview of systematic reviews. J Orthop Surg Res 2025;20:718. [Google Scholar] [PubMed]
- 3. Guyen O. Hemiarthroplasty or total hip arthroplasty in recent femoral neck fractures? Orthop Traumatol Surg Res 2019;105:S95-101. [Google Scholar] [PubMed]
- 4. Mori Y, Tarasawa K, Tanaka H, Mori N, Fushimi K, Fujimori K, et al. Does total hip arthroplasty in elderly patients with femoral neck fractures reduce complications? A Japanese DPC study. J Orthop Sci 2025;30:507-12. [Google Scholar] [PubMed]
- 5. Muslim SM, Lingayat MB, Bansode P, Kesharwani A. Comparative outcome assessment of total hip arthroplasty versus bipolar hemiarthroplasty in intracapsular neck of femur fracture in old age. Int J Res Orthop 2023;9:956-61. [Google Scholar] [PubMed]
- 6. Rogmark C, Carlsson A, Johnell O, Sernbo I. A prospective randomised trial of internal fixation versus arthroplasty for displaced fractures of the neck of the femur. Functional outcome for 450 patients at two years. J Bone Joint Surg Br 2002;84:183-8. [Google Scholar] [PubMed]
- 7. Salmons HI, Donnelly PC, Guy DK, Abdel MP. Hemiarthroplasty versus total hip arthroplasty for femoral neck fracture in the elderly: An analysis from the American joint replacement registry. J Arthroplasty 2025;41:765-9. [Google Scholar] [PubMed]
- 8. Cho YJ, Nam DC, Jung K. Arthroplasty in femoral head osteonecrosis. Hip Pelvis 2014;26:65-73. [Google Scholar] [PubMed]
- 9. Lehtimäki, Kautiainen H, Hämäläinen MM, Lehto MU, Ikävalko M, Repo AB, et al. Hip involvement in seropositive rheumatoid arthritis. Survivorship analysis with a 15-year follow-up. Scand J Rheumatol 1998;27:406-9. [Google Scholar] [PubMed]
- 10. Bukowski BR, Clark NJ, Taunton MJ, Freedman BA, Berry DJ, Abdel MP. Primary total hip arthroplasty in patients with ankylosing spondylitis. J Arthroplasty 2021;36:S282-9. [Google Scholar] [PubMed]
- 11. Salman LA, Hantouly AT, Khatkar H, Al-Ani A, Abudalou A, Al-Juboori M, et al. The outcomes of total hip replacement in osteonecrosis versus osteoarthritis: A systematic review and meta-analysis. Int Orthop 2023;47:3043-52. [Google Scholar] [PubMed]
- 12. Lombardi B, Paci M, Nannetti L, Moretti S, Maritato M, Benelli G. Total hip arthroplasty after hip fracture or osteoarthritis: Are there differences in characteristics and outcomes in the early rehabilitative stage? Orthop Nurs 2014;33:43-7. [Google Scholar] [PubMed]
- 13. Charette RS, Sloan M, Lee GC. Not all hip arthroplasties are created equal: Increased complications and re-admissions after total hip arthroplasty for femoral neck fractures compared with osteoarthritis. Bone Joint J 2019;101-B:84-90. [Google Scholar] [PubMed]
- 14. Aprato A, Massè A, Caranzano F, Matteotti R, Pautasso P, Daghino W, et al. Patient-perceived quality of life after total hip arthroplasty: Elective versus traumatological surgery. ISRN Orthop 2011;2011:910392. [Google Scholar] [PubMed]
- 15. Abboud JA, Patel RV, Booth RE Jr., Nazarian DG. Outcomes of total hip arthroplasty are similar for patients with displaced femoral neck fractures and osteoarthritis. Clin Orthop Relat Res 2004;421:151-4. [Google Scholar] [PubMed]
- 16. Lizaur-Utrilla A, Sanz-Reig J, Miralles-Muñoz FA. Cementless total hip arthroplasty after acute femoral neck fracture in active patients. Prospective matched study with a minimum follow-up of 5 years. Rev Esp Cir Ortop Traumatol 2014;58:152-9. [Google Scholar] [PubMed]
- 17. Agarwal V, Dhanda MS, Singh A, Madhan HS, Goel S, Agarwal S, et al. An evaluation of merits of total hip arthroplasty done for traumatic and non-traumatic displaced fracture neck of femur. Int J Res Med Sci 2016;4:1632-5. [Google Scholar] [PubMed]
- 18. Sassoon A, D’Apuzzo M, Sems S, Cass J, Mabry T. Total hip arthroplasty for femoral neck fracture: Comparing in-hospital mortality, complications, and disposition to an elective patient population. J Arthroplasty 2013;28:1659-62. [Google Scholar] [PubMed]
- 19. Ritter J, Alimy AR, Simon A, Hubert J, Ries C, Rolvien T, et al. Patients with periprosthetic femoral hip fractures are commonly classified as having osteoporosis based on DXA measurements. Calcif Tissue Int 2024;115:142-9. [Google Scholar] [PubMed]
- 20. Mathur HH, Kapadiya BD. Short term outcomes of total hip arthroplasty for neck femur fracture in patients above 50 years of age. Int J Orthop Sci 2020;6:1339-43. [Google Scholar] [PubMed]
- 21. Wendler T, Edel M, Möbius R, Fakler J, Osterhoff G, Zajonz D. Fixation of intraoperative proximal femoral fractures during THA using two versus three cerclage wires – a biomechanical study. BMC Musculoskelet Disord 2022;23:40. [Google Scholar] [PubMed]
- 22. Ortiguera CJ, Pulliam IT, Cabanela ME. Total hip arthroplasty for osteonecrosis: Matched-pair analysis of 188 hips with long-term follow-up. J Arthroplasty 1999;14:21-8. [Google Scholar] [PubMed]
- 23. Hu Y, Jiang WZ, Pan CL, Wang T. Active ankylosing spondylitis increases blood loss during total hip arthroplasty for a stiff hip joint. BMC Musculoskelet Disord 2020;21:243. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review
June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report
July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes