
This article highlights the importance of early detection and timely removal of migrated Kirschner wires (K-wires) to prevent complications, especially in mobile joints such as the acromioclavicular joint.
Dr. Mantu Jain, Department of Orthopedics, AIIMS, Bhubaneswar, Odisha, India. E-mail: montu_jn@yahoo.com
Abstract
Introduction: Kirschner wires (K-wires) are commonly used in orthopedic fixation, but their potential for migration can lead to serious complications.
Case Report: We present a rare case of a middle-aged male who reported persistent right-sided neck and shoulder pain 3 years following surgery for a lateral end clavicle fracture. Imaging revealed two broken K-wire fragments – one in the right supraclavicular region and another in the posterior neck musculature. The wires were successfully removed through a posterior neck surgical approach with the help of an otorhinologist, and the patient had complete symptomatic resolution postoperatively.
Conclusion: This case underscores the unusual scenario of dual K-wire migration into the cervical region without neurological involvement. It highlights the critical importance of timely hardware removal and cautious use of unthreaded K-wires in mobile joints such as the acromioclavicular joint. Clinicians must be vigilant about potential wire migration, especially in patients with unexplained persistent pain post-surgery. Early detection and multidisciplinary surgical management are key to preventing catastrophic outcomes.
Keywords: Kirschner wire, migration, acromioclavicular joint, neck.
Kirschner wires (K-wires) are commonly used in orthopedic surgeries, ranging from provisional fixation to definitive fracture stabilization [1]. With the evolution of more stable and biomechanically superior implants, such as anatomically contoured plates and intramedullary nails for internal fixation, their routine use for definitive fixation has declined [2]. Nonetheless, K-wires are still used in selected indications, particularly in resource-constrained settings, due to their affordability and ease of use. A major concern associated with K-wire fixation is the potential for delayed removal, which may result in complications [3,4]. Among these, migration of the wire to distant or critical anatomical locations represents the most serious and potentially life-threatening outcome [5,6,7]. Although several cases of K-wire migration have been documented in the literature, migration into the cervical region remains exceedingly rare. We report a unique case of dual K-wire migration into the neck following clavicle fixation, which remained undiagnosed for several years.
A middle-aged male in his fifties presented to our institution with a 3-year history of persistent right-sided neck and shoulder pain. The pain, localized to the posterior neck and right supraclavicular region, had been managed symptomatically at multiple local healthcare facilities without definitive relief. There was no radiation of pain or paraesthesia in either upper limb. The patient had previously been treated for cervical spondylosis, with partial symptom relief following analgesics; however, the symptoms persisted. On detailed history, the patient reported having undergone surgical fixation for a right shoulder fracture 6 years prior (Fig. 1a).
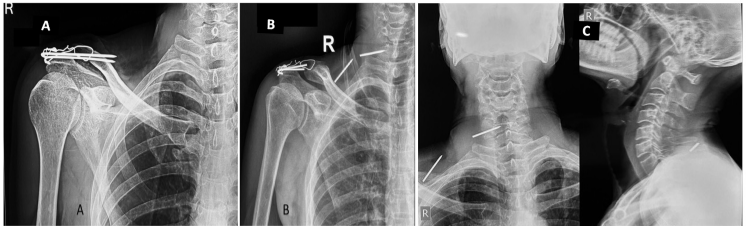
Figure 1: Old radiograph of the right shoulder showing tension band wiring of the acromioclavicular joint and a malunited but healed lateral end clavicle fracture (a); Recent radiograph of the right shoulder (b) and neck demonstrating two broken K-wire fragments migrated to the posterior neck on the right side-one located in the right supraclavicular region and the other at the posterior aspect of the neck (c).
Clinical examination revealed no signs of radiculopathy, motor weakness, or restriction in neck mobility. However, a palpable small swelling (3 × 2 cm) was noted in the right supraclavicular region. The carotid artery was well palpated, and the swelling was lateral to the vascular bundle. Radiographs of the shoulder and neck revealed two broken K-wire fragments – one located in the right supraclavicular region and another posteriorly near the cervical spine (Fig. 1b and c). The shoulder radiograph showed a malunited lateral end clavicle fracture fixed with tension band wiring over two K-wires, both of which were broken distally. A non-contrast computed tomography (CT) scan of the neck was performed to delineate the exact position of the migrated wires (Fig. 2). The case was reviewed in a multidisciplinary team setting with input from an otorhinolaryngology expert. Routine pre-operative laboratory investigations were within normal limits, and the patient was planned for elective hardware removal.
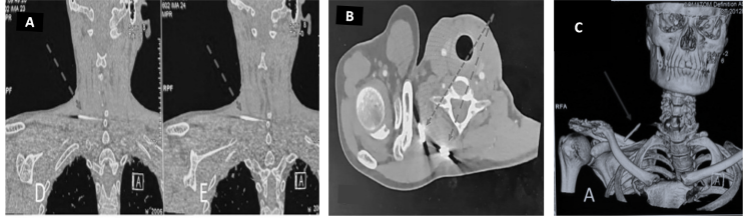
Figure 2: Coronal computed tomography (CT) sections localizing the exact position of the migrated wires (a); Axial CT image (b), and 3D-reconstructed images from CT scan showing the position of the migrated K-wires (c).
Surgical technique
Under general anesthesia, the patient was positioned in the lateral decubitus position. Intraoperative localization of the K-wire fragments was achieved using fluoroscopic guidance, correlating with pre-operative CT findings. A single curvilinear incision was made over the posterior cervical region and extended anteriorly toward the supraclavicular fossa (Fig. 3a).
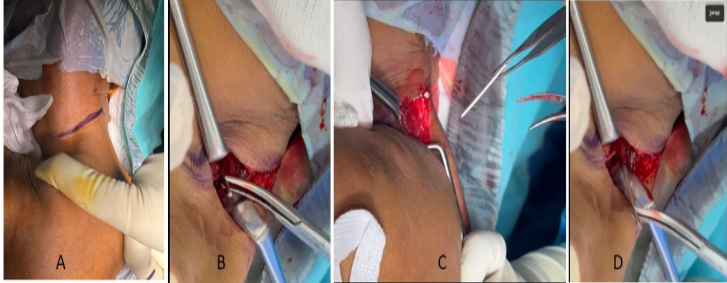
Figure 3: Intraoperative photographs showing the skin incision (a) and retrieval of the two K-wire fragments (b-d).
Dissection was carefully performed in two anatomical planes around the trapezius muscle. The first K-wire fragment was identified anterior to the trapezius within the supraclavicular region. After blunt and sharp dissection through the platysma and fascia, the wire (8 cm length) was successfully retrieved (Fig. 3b). Dissection then continued posterior to the trapezius, where the second K-wire fragment (7 cm length) was located in the paraspinal musculature and removed without difficulty (Fig. 3c and d). In the same operative session, a separate incision was made over the acromion process to remove the tension band wiring from the acromioclavicular joint. The lateral clavicle fracture was found to be malunited, but as the patient was asymptomatic, no further intervention was performed. Both surgical sites were irrigated thoroughly and closed in layers. Post-operative radiographs confirmed complete removal of hardware (Fig. 4). The patient recovered uneventfully, with complete resolution of symptoms by the 1-month follow-up. At 3 months, he remained pain-free with a full, pain-free range of motion at the shoulder and cervical spine.
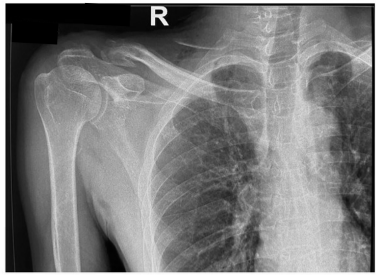
Figure 4: Post-operative radiograph confirming complete removal of the migrated K-wire fragments and the previously placed tension band wiring from the acromioclavicular joint.
This report is unique in that it documents the migration of two distinct broken segments of K-wires into the cervical region – an exceptionally rare phenomenon. While K-wire migration is a recognized complication, it typically involves either a complete wire or a single fragment. In our case, two sizable fragments migrated independently to different anatomical planes in the neck and were successfully removed before causing life-threatening consequences. K-wire migration can lead to serious complications, particularly when wires penetrate critical structures such as the spinal canal, thoracic cavity, or neurovascular bundles [5,6,7,8,9,10,11,12]. A comprehensive search of the PubMed database using the keywords “K-wire,” “migration,” and “neck” yielded 42 articles related to K-wire migration into the cervical region. In addition, relevant references were manually reviewed, resulting in the retrieval of 19 articles specifically reporting K-wire migration into the neck originating from the clavicle or proximal humerus (Table 1). The majority of these cases described migration from the shoulder region to the cervical spine, often associated with neurological symptoms or deficits. There have also been reports of wires migrating into the thoracic cavity and mediastinum. However, migration into the neck without neurological involvement is exceedingly rare. We identified only four such cases in the literature, including those described by Leppilahti and Jalovaara [13], Batin et al. [14], and Ko and Lee. [15].
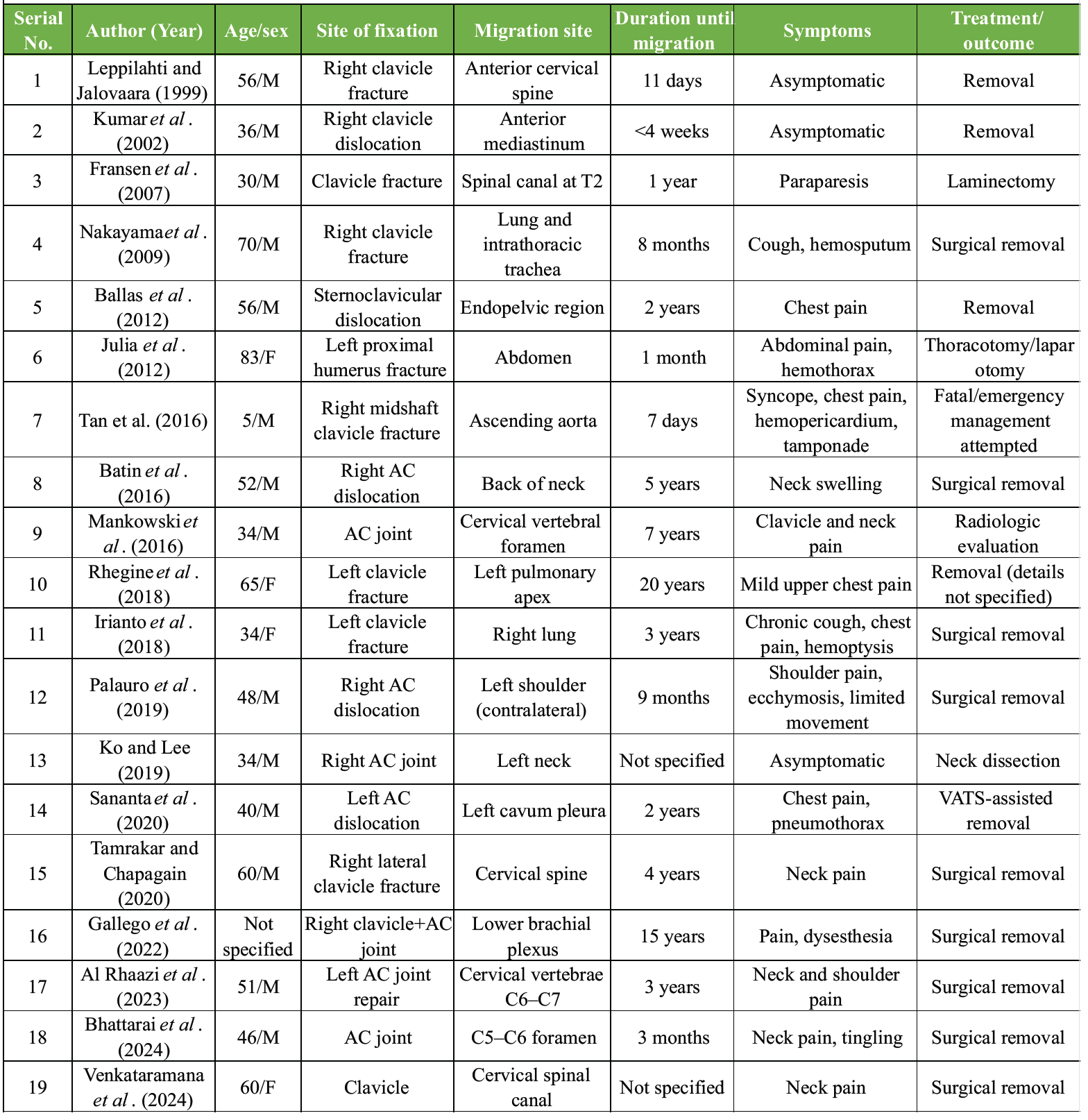
Table 1: Cases of K-wire migration from the clavicle/AC joint/proximal humerus fixation site to neck, thoracic regions, and other distant sites
The mechanisms underlying K-wire migration are multifactorial. Repeated or oscillatory drilling – especially with reused wires – can induce localized thermal necrosis and osteolysis, impairing bone anchorage [16,17,18]. Unthreaded wires, commonly used due to ease of insertion, have less purchase and are more prone to dislodgement. In addition, mechanical forces generated by muscle contractions, joint mobility, and thoracic movements can contribute to wire migration. In this case, the use of tension band wiring for a lateral end clavicle fracture, passing through the acromion, subjected the wires to cyclical biomechanical stress across the mobile acromioclavicular joint. Both wires fractured at the clavicular entry site and migrated – one anteriorly into the supraclavicular region and the other posteriorly into the paraspinal musculature – likely along paths of least resistance. Fortunately, neither fragment impinged on adjacent major neurovascular structures such as the brachial plexus, spinal cord, carotid artery, or jugular veins. The delayed presentation in this case emphasizes the lack of awareness among the patients and the primary care providers regarding the potential for K-wire migration. Early evaluation at the onset of neck pain could have led to the timely detection of the migrated wires, potentially preventing prolonged symptoms and associated risks. As noted by Wichlas et al. [19], off-label use of K-wires persists in many low-/middle-income countries due to constrained implant availability. The majority of reported migrations originate from procedures around the shoulder girdle, particularly the acromioclavicular joint, owing to its high mobility and muscle traction [6,7,8,14,15,16]. Biomechanically sound fixation is essential to mitigate such risks. Pre-contoured lateral clavicle plates or hook plates offer more rigid constructs for lateral end clavicle fractures [20]. Supplementation with lag screws may enhance stability further. Flexible fixation devices such as TightRope systems have shown promise, although current evidence remains limited [21,22,23]. Importantly, to prevent heat-induced osteonecrosis, intermittent drilling with adequate saline irrigation should be employed during K-wire insertion [18]. Definitive prevention of wire-related complications lies in the timely removal of the implant. While conservative management has been attempted in select cases [24], it mandates serial imaging and close surveillance. Surgical retrieval remains the safest and most reliable option, particularly when the migrated fragment is mobile or encroaching on vital structures.
K-wire migration is a potentially serious complication of acromioclavicular fixation. Prompt removal of wires following fracture union is critical to prevent adverse outcomes. When migration occurs, early diagnosis and multidisciplinary surgical management can avert catastrophic consequences. This case reinforces the importance of adhering to safe fixation principles and vigilant post-operative follow-up.
Clinicians should be vigilant for potential K-wire migration in patients with unexplained post-surgical pain, particularly in mobile joints, and prioritize early detection and timely removal to prevent serious complications.
References
- 1. Franssen BB, Schuurman AH, Van Der Molen AM, Kon M. One century of Kirschner wires and Kirschner wire insertion techniques: A historical review. Acta Orthop Belg 2010;76:1-6. [Google Scholar] [PubMed]
- 2. Kang DH, Jung DW, Kim YH, Kim TG, Lee J, Chung KJ. Kirschner wire fixation for the treatment of comminuted zygomatic fractures. Arch Craniofac Surg 2015;16:119-24. [Google Scholar] [PubMed]
- 3. Wasiak M, Piekut M, Ratajczak K, Waśko M. Early complications of percutaneous K-wire fixation in pediatric distal radius fractures-a prospective cohort study. Arch Orthop Trauma Surg 2023;143:6649-56. [Google Scholar] [PubMed]
- 4. Stahl S, Schwartz O. Complications of K-wire fixation of fractures and dislocations in the hand and wrist. Arch Orthop Trauma Surg 2001;121:527-30. [Google Scholar] [PubMed]
- 5. Ballas R, Bonnel F. Endopelvic migration of a sternoclavicular K-wire. Case report and review of literature. Orthop Traumatol Surg Res 2012;98:118-21. [Google Scholar] [PubMed]
- 6. Hrubovčák J, Tulinský Ľ, Jelínek P, Potičný S, Roman J, Szeliga J. From case to context: A case-driven comprehensive review on Kirschner wire migration to the cervical spine and neck. Trauma 2024;27:170-7. [Google Scholar] [PubMed]
- 7. Gallego Palmero C, De La Red Gallego MD, Velez Garcia OM, Gutiérrez Olivera N. Migration of broken Kirschner wire to the brachial plexus after fixation of fracture dislocation of the acromioclavicular joint. J Hand Surg Asian Pac Vol 2022;27:907-11. [Google Scholar] [PubMed]
- 8. Bhattarai A, Gurung B, Sherchan B, Rijal B, Karki PD. K wire migration into spinal canal: an infrequent cause of neurological morbidity – a case report. Ann Med Surg (Lond) 2024;86:7431-5. [Google Scholar] [PubMed]
- 9. Sananta P, Dradjat RS, Julana R, Pandiangan RA, Sukmajaya WP, Abduh M. Migration of K-wire into the cavum pleura after the reduction of acromioclavicular dislocation, a case report and review of literature. Int J Surg Case Rep 2020;74:192-5. [Google Scholar] [PubMed]
- 10. Özbey M, Türkmen U, Şahin E. Thirteen years of migration of Kirschner wires: A mediastinal foreign body. Turk J Thorac Cardiovasc Surg 2023;31:412-5. [Google Scholar] [PubMed]
- 11. Yadav V, Marya KM. Unusual migration of a wire from shoulder to neck. Indian J Med Sci 2003;57:111-2. [Google Scholar] [PubMed]
- 12. Furuhata R, Nishida M, Morishita M, Yanagimoto S, Tezuka M, Okada E. Migration of a Kirschner wire into the spinal cord: A case report and literature review. J Spinal Cord Med 2018;43:272-5. [Google Scholar] [PubMed]
- 13. Leppilahti J, Jalovaara P. Migration of Kirschner wires following fixation of the clavicle–a report of 2 cases. Acta Orthop Scand 1999;70:517-9. [Google Scholar] [PubMed]
- 14. Batın S, Ozan F, Gürbüz K, Uzun E, Kayalı C, Altay T. Migration of a broken Kirschner wire after surgical treatment of acromioclavicular joint dislocation. Case Rep Surg 2016;2016:6804670. [Google Scholar] [PubMed]
- 15. Ko HY, Lee KW. Contralateral migration of Kirschner wire from right acromioclavicular joint to left side of neck: A case report. J Med Case Rep 2019;13:375. [Google Scholar] [PubMed]
- 16. Lyons FA, Rockwood CA Jr. Migration of pins used in operations on the shoulder. J Bone Joint Surg Am 1990;72:1262-7. [Google Scholar] [PubMed]
- 17. Muriuki MG, Reddy AK, Tauchen A, Havey RM, Patwardhan AG, Bindra RR. Effect of K-wire reuse and drill mode on heat generation in bone. Hand (N Y) 2023;18:314-9. [Google Scholar] [PubMed]
- 18. Luo Y, Chen L, Finney FT, Park DW, Talusan PG, Holmes JR, et al. Evaluation of heat generation in unidirectional versus oscillatory modes during K-wire insertion in bone. J Orthop Res 2019;37:1903-9. [Google Scholar] [PubMed]
- 19. Wichlas F, Hofmann V, Strada G, Moursy M, Deininger C. Off-label use of orthopedical trauma implants in a low-income country. Int Orthop 2022;46:21-7. [Google Scholar] [PubMed]
- 20. Jo OI, Almond M, Rupansinghe HS, Ackland DC, Ernstbrunner L, Ek ET. Biomechanical analysis of plating techniques for unstable lateral clavicle fractures with coracoclavicular ligament disruption (Neer type IIB). J Shoulder Elbow Surg 2023;32:695-702. [Google Scholar] [PubMed]
- 21. Ahmed AF, Salameh M, Kayali H, Hantouly A, Darwiche A. Open reduction and tunneled suspensory fixation for lateral end of clavicle fractures: Surgical technique. JSES Rev Rep Tech 2022;2:345-9. [Google Scholar] [PubMed]
- 22. Soh C, Sivapathasundaram N, Parthiban R, Ramanand A. A technique of distal clavicle fracture fixation using the tightrope procedure. Malays Orthop J 2011;5:20-3. [Google Scholar] [PubMed]
- 23. Al-Tawil K, Garner M, Antonios T, Karrupaiah K, Tahmassebi R, Colegate-Stone T, et al. The use of Tightrope device as the sole method of fixation in treating lateral end clavicle fractures. Shoulder Elbow 2022;14:60-4. [Google Scholar] [PubMed]
- 24. Liberski J, Ficek K. Kirschner wire migration from the clavicle to the cervical spine. Int J Case Rep Images 2013;4:308-11. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Chronic Acromioclavicular Joint Instability: Outcomes after Stabilization without Tendon Graft Augmentation
July 1, 2026 Chronic Acromioclavicular Joint Instability: Outcomes after Stabilization without Tendon Graft Augmentation May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series
May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series September 1, 2025 A Silent Shoulder of Plentiful Pathology: An Uncommon Presentation of Acromioclavicular Ganglion Cyst
September 1, 2025 A Silent Shoulder of Plentiful Pathology: An Uncommon Presentation of Acromioclavicular Ganglion Cyst April 1, 2025 Failed Loop Endobutton Acromioclavicular Joint Reconstruction Treated with Duo Figure of 8 FiberTape Augmented Autogenic Graft Wrapping Technique: A Case Report
April 1, 2025 Failed Loop Endobutton Acromioclavicular Joint Reconstruction Treated with Duo Figure of 8 FiberTape Augmented Autogenic Graft Wrapping Technique: A Case Report