
Combined ALPSA, Hill–Sachs, and HAGL lesions can be effectively managed with a comprehensive, individualized, all-arthroscopic repair strategy to restore shoulder stability.
Dr. Ziad Noun, Clemenceau Medical Center, Clemenceau, Beirut, Lebanon. E-mail: smznoun@hotmail.com
Abstract
Introduction: Traumatic anterior shoulder instability is common in young patients; however, the simultaneous occurrence of an anterior labral periosteal sleeve avulsion (ALPSA) lesion, Hill–Sachs defect, and humeral avulsion of the glenohumeral ligament (HAGL) is exceptionally rare. Managing multiple concurrent soft-tissue and bony injuries presents significant diagnostic and therapeutic challenges. This report describes a unique case of combined ALPSA, Hill–Sachs, and HAGL lesions treated with an all-arthroscopic approach, highlighting the importance of comprehensive evaluation and tailored surgical planning in complex instability patterns.
Case Report: A 17-year-old female sustained a traumatic shoulder injury resulting in recurrent anterior dislocations, progressive pain, and functional weakness. Imaging revealed the coexistence of an ALPSA lesion, a significant Hill–Sachs defect, and a HAGL lesion. Given the complexity of instability, an all-arthroscopic repair strategy was adopted. The procedure included arthroscopic ALPSA repair to restore labral integrity, Hill–Sachs remplissage to address the engaging humeral defect, and arthroscopic HAGL repair using strategic anchor placement and precise suture management to re-establish capsuloligamentous continuity. Postoperative rehabilitation progressed uneventfully, and at 18 months follow-up, the patient demonstrated a near-normal range of motion, excellent functional recovery, and no recurrence of instability.
Conclusion: The coexistence of ALPSA, Hill–Sachs, and HAGL lesions represents a rare and challenging clinical scenario. This case illustrates that a carefully planned all-arthroscopic approach can successfully restore shoulder stability and function while minimizing morbidity. Thorough assessment and individualized treatment strategies are essential for optimal outcomes in complex instability presentations. Further research is warranted to assess the long-term results of combined arthroscopic repair in such rare lesion patterns.
Keywords: Anterior shoulder instability, anterior labral periosteal sleeve avulsion, humeral avulsion of the glenohumeral ligament, Hill–Sachs, arthroscopic repair.
Traumatic anterior shoulder dislocations are among the most common joint dislocations, comprising approximately 45% of all large joint dislocations, with an incidence of 23.9/100,000 person-years [1]. These injuries frequently result in a spectrum of soft tissue and bony lesions that compromise glenohumeral stability. The most commonly encountered injuries include anterior labral periosteal sleeve avulsion (ALPSA), which involves detachment of the labrum with medial displacement and an intact glenoid rim, and Hill–Sachs lesions, characterized by a posterolateral humeral head compression fracture resulting from impaction against the anterior glenoid rim during dislocation [1,2]. Less frequently, dislocations may lead to humeral avulsion of the glenohumeral ligament (HAGL), a disruption of the inferior glenohumeral ligament (IGHL) from its humeral insertion, contributing to persistent instability [3]. While the individual occurrence of these injuries is well documented, the simultaneous presence of all three ALPSA, Hill–Sachs, and HAGL lesions remains exceptionally rare. Existing literature has described concurrent ALPSA and Hill–Sachs lesions as a common combination in recurrent instability [1,4], and studies have reported that HAGL lesions often occur with other pathologies such as labral tears or rotator cuff injuries [5,6]. However, the triad of ALPSA, Hill-Sachs, and HAGL lesions presenting in a single patient and addressed through a unified arthroscopic approach has been scarcely reported. The management of such complex instability patterns poses significant challenges, as each lesion contributes uniquely to shoulder dysfunction. Although arthroscopic techniques have evolved to allow effective repair of these injuries individually, with ALPSA, a variant of the Bankart lesion, undergoing repair and remplissage with favorable outcomes [7,8], and arthroscopic HAGL repair increasingly preferred for reduced morbidity [6,9], there remains limited evidence guiding comprehensive, all-arthroscopic management of this rare combination. Here, we present a rare case of a young female patient with chronic anterior shoulder instability who was found to have concomitant ALPSA, HAGL, and Hill-Sachs lesions on imaging and underwent successful all-arthroscopic surgical repair of all three lesions. This report aims to describe the surgical technique used, highlight key intraoperative decision-making strategies, and discuss the significance of recognizing and addressing this triad in achieving shoulder stability and optimal functional outcomes.
The case we are sharing is of a 23-year-old active right-hand dominant female patient who presented to our outpatient clinic with a 6-year history of recurrent right shoulder dislocations. Her initial injury occurred at the age of 17 years following a fall down a flight of stairs, during which she sustained an anterior dislocation of the right shoulder. She was evaluated at a local emergency department, where plain radiographs confirmed an anterior glenohumeral dislocation. Closed reduction was performed successfully, and she was managed conservatively with a sling and swathe immobilization for 3 weeks, followed by a structured physiotherapy program. Over the past 6 years, the patient has experienced 3 additional episodes of anterior shoulder dislocation, each of which required closed reduction. These episodes occurred during relatively low-energy mechanisms, consistent with recurrent anterior shoulder instability. The patient had no known prior significant comorbidities, surgeries, or connective tissue disorders. The patient presented with chronic right shoulder pain and episodes of instability following a remote traumatic injury, with recurrent feelings of the shoulder “giving way.” She complained of decreased range of motion, weakness, and persistent pain interfering with activities of daily living. On examination, the patient exhibited classic signs of anterior shoulder instability. She had a positive apprehension test, expressing fear and discomfort when the shoulder was placed in abduction and external rotation. She also had a positive relocation test with generalized tenderness over the anterior shoulder, no gross deformity at rest. Her range of motion was preserved but limited at end-range due to apprehension. A very mild wasting of the periscapular musculature was noted, but the patient was skinny in nature. No signs of posterior or multidirectional instability were elicited. Neurological examination was intact with no deficits.
A magnetic resonance imaging (MRI) arthrogram of the right shoulder was performed, revealing (Fig. 1):
- Hill–Sachs lesion: A well-defined posterolateral humeral head indentation is evident on multiple axial slices, consistent with a Hill–Sachs lesion. The lesion appears to be moderately deep and engaging, based on its orientation and surface area.
- ALPSA lesion: Detachment and irregularity of the anteroinferior labrum with seemingly an intact periosteum visualized from the 2 to 5 o’clock position (right shoulder), with interposition of contrast between the labrum and glenoid was identified. This is typical of an ALPSA lesion – a variant of the Bankart lesion. The anterior band of the IGHL appears disrupted. No bone loss of the glenoid could be discerned on the MRI.
- HAGL lesion: Contrast extravasation along the medial aspect of the humeral neck, suggestive of a HAGL lesion with discontinuity of the anterior band of the IGHL near its humeral attachment, and contrast tracking along the medial humeral neck were also identified. Clear disruption of the IGHL at its humeral insertion was noted, with its origin appearing indistinct and with irregular signal intensity along its expected course. Presence of contrast and fluid extravasation tracking inferiorly outside the joint capsule, confirming capsular disruption.
Otherwise, the joint appeared distended with intra-articular contrast, clearly outlining intra-capsular structures. No loose bodies were seen. Mild tendinopathy of the rotator cuff was noted at its attachment, with no long head of the biceps tendon or acromioclavicular joint pathologies observed.
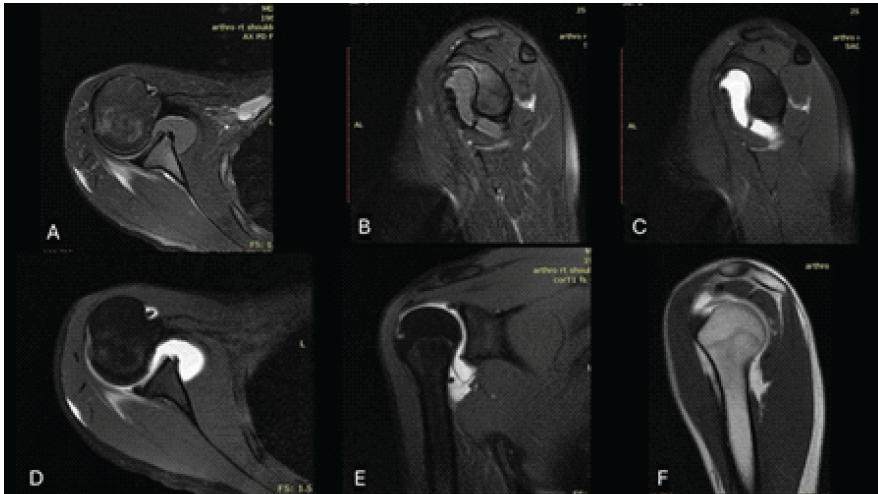
Figure 1: (a) Sagittal proton density fat-saturated magnetic resonance imaging (MRI) showing a medially displaced anterior labroligamentous periosteal sleeve avulsion (ALPSA) lesion with fluid signal indicating anterior labral detachment. (b) Sagittal T1-weighted fat-saturated post-contrast MRI demonstrating enhancement of the displaced anterior labroligamentous complex consistent with ALPSA lesion and reactive synovitis. (c) Axial T1-weighted fat-saturated post-contrast image revealing a Hill–Sachs lesion characterized by a cortical depression and adjacent bone marrow edema in the posterolateral humeral head. (d) Coronal T1-weighted fat-saturated post-contrast MRI showing a humeral avulsion of the glenohumeral ligament (HAGL) lesion with contrast extravasation and ligament disruption at the humeral attachment. (e) Sagittal T1-weighted MRI highlighting a chronic cortical defect of the posterolateral humeral head, consistent with a Hill–Sachs lesion. (f) Axial proton density fat-saturated MRI demonstrating disruption and fluid tracking at the humeral insertion of the IGHL, indicative of a HAGL lesion.
These findings confirmed significant structural pathology predisposing her and contributing to her recurrent anterior instability. As discussed in the introduction, the occurrence of these three lesions simultaneously is a rare finding, and addressing all three simultaneously is not prevalent in the literature. Given the history of recurrent dislocations, physical examination findings consistent with anterior instability, and confirmatory imaging showing multiple lesions, the patient was scheduled for arthroscopic surgical stabilization of the right shoulder. The planned procedure included an ALPSA repair with possible remplissage for the Hill–Sachs lesion and repair of the HAGL lesion, depending on intraoperative findings. Written informed consent was obtained from the patient for publication of this case report and any accompanying images and videos.
Surgical technique
Given the absence of extensive studies on the concomitant presence of all three lesions and the management of such a patient, we decided to perform an arthroscopic anterior shoulder stabilization with an ALPSA repair, HAGL lesion repair, and Hill–Sachs remplissage in an all-arthroscopic approach (Video 1).
Under general anesthesia with regional interscalene block, the patient was given antibiotic prophylaxis and placed in the lateral decubitus position with traction applied to the operative arm. After scrubbing and draping the right upper limb in the usual sterile manner, a standard posterior portal viewing portal is established first. Diagnostic glenohumeral arthroscopy confirmed detachment of the anteroinferior labrum, sparing the periosteum (ALPSA lesion) from the 2 to 5 o’clock position with a humeral avulsion of the IGHL (HAGL lesion) and an engaging medialized Hill–Sachs lesion on the posterolateral humeral head of moderate depth, but with a relatively wide surface area. Accessory anterior and anterosuperior portals, through which two cannulas were placed, were then created under spinal needle guidance. We started with the ALPSA lesion, and the anteroinferior glenoid is debrided using an Incisor 4.5 mm blade – arthroscopic shaver blade (Smith and Nephew, Watford, UK) and rasp to promote healing. The detached labrum was then mobilized and reduced to the glenoid rim. Two SutureFix 1.7 mm anchors (Smith and Nephew, Watford, UK) were then placed at the 2 and 5 o’clock positions along the anterior glenoid face. Non-absorbable sutures were next passed through the labrum and capsulolabral complex using a FirstPass Mini Suture Passer (Smith and Nephew, Watford, UK). Following that, we move to the intra-articular remplissage through a posterolateral portal. This portal was located about 1–1.5 cm lateral and inferior to the standard posterior portal under spinal needle guidance. The Hill–Sachs defect was visualized intra-articularly through the standard posterior portal. Through the second posterolateral portal, a TwinFix PK 5.5 mm anchor (Smith and Nephew, Watford, UK) was placed in the Hill–Sachs lesion after careful debridement and preparation using an Incisor 4.5 mm blade — arthroscopic shaver blade (Smith and Nephew, Watford, UK) and a curette. Sutures were then shuttled intra-articularly through the posterior capsule and infraspinatus tendon using a penetrating tool. The sutures were then left without tying, allowing further access to repair the HAGL lesion before remplissage is completed. We moved back to the anterior ALPSA lesion and the knots of the previously placed anterior glenoid anchors were tied arthroscopically to reapproximate the labrum to the glenoid rim, restoring the bumper effect. Next, the inferior capsule and IGHL complex are visualized through the same posterior portal, identifying the HAGL lesion. At the humeral neck, right distal to the most distal extent of the Hill-Sachs lesion was selected as the anchor site, reflecting its anatomic proximity to the IGHL footprint while also taking leverage of the anatomical confluence of the HAGL lesion and Hill–Sachs defect, minimizing additional hardware and optimizing soft tissue healing. The selected area was lightly debrided to promote healing. One SutureFix 1.7 mm anchor (Smith and Nephew, Watford, UK) was then placed into the humeral neck just after the most distal aspect Hill–Sachs lesion through the posterolateral portal. The sutures were passed through the avulsed IGHL and inferior capsule using an AccuPass suture passer (Smith and Nephew, Watford, UK) and were left untied. Returning to the anchor placed at the humeral neck for HAGL lesion repair, the passed sutures were tied securely, restoring the integrity of the IGHL complex. Finally, the sutures of the anchor placed for the Hill-Sachs remplissage were tied intra-articularly, converting the engaging Hill-Sachs lesion into a non-engaging defect, while maintaining the HAGL repair construct. With the procedure complete, the shoulder was examined under direct visualization to confirm stability and lack of engagement in functional positions. The shoulder joint was exited, and the portals were closed in the standard fashion. Postoperatively, sling and swathe immobilization were done for 4 weeks. Passive range of motion began at 4 weeks postoperative, and active-assisted range of motion was initiated at 6 weeks, and finally, active range of motion was started at 8 weeks postoperative. Strengthening exercises were permitted at 3 months, and return to leisure sport was permitted at 6 months, with the patient achieving nearly the full range of motion in movement without apprehension. At 18 months of follow-up, the patient has achieved a near symmetrical range of motion to the contralateral shoulder, continues to have no complaints, and has returned to lead a full, normal life (Video. 2).
Surgical pearls
- Dual-purpose anchor placement at the distal Hill–Sachs lesion and proximal part of the humeral neck allowed simultaneous HAGL repair and remplissage, improving efficiency and minimizing implant load.
- Meticulous suture passage through the IGHL and posterior capsule and infraspinatus is essential for restoring both static and dynamic stabilizers
- Comprehensive management of ALPSA, HAGL, and Hill–Sachs lesions is critical to restoring anterior shoulder stability in this rare case of these three combined pathologies.
Anterior shoulder dislocations frequently result from a fall or direct trauma to the shoulder, whether during daily activities or sports and recreational events. They have an estimated incidence of 23.9/100,000 person-years and account for approximately 45% of all joint dislocations, with more than 95% of these dislocations occurring in the anterior direction [1]. Traumatic anterior dislocations are commonly associated with injuries to both soft tissue and bony structures surrounding the glenohumeral joint, identified using MRI/magnetic resonance (MR) arthrography or computed tomography/computed tomography arthrography, respectively [10]. Simultaneous occurrence of HAGL, ALPSA, and Hill-Sachs lesions in the context of anterior shoulder instability is an uncommon but clinically significant presentation. Hence, the understanding of the pathoanatomy, prevalence, and management strategies for these combined injuries is crucial for optimal patient outcomes [3].
Pathoanatomy and prevalence
Anterior shoulder dislocations often result in a spectrum of injuries, notably Bankart lesions, Hill-Sachs lesions, and, less commonly, HAGL lesions. First described by Bankart in 1938, the Bankart lesion involves a detachment of the anteroinferior labrum from the glenoid rim along with the joint capsule avulsion, compromising joint stability. A recognized variant is the ALPSA, where the labrum displaces medially along the glenoid neck while the periosteum remains intact, leading to greater instability and technical challenges in repair [1]. On the other hand, Hill–Sachs lesions are osteochondral or chondral compression fractures of the posterolateral humeral head caused by impaction against the anterior glenoid rim during dislocation [2]. In contrast, HAGL lesions refer to the avulsion of the IGHL from their humeral insertion, leading to capsular laxity and instability, due to their essential role as a primary shoulder stabilizer. This mainly occurs during an external rotation hyperabduction mechanism of injury [3].
Rutgers et al. [1] conducted a systematic review and meta-analysis comparing first-time and recurrent anterior shoulder dislocations. Their most notable finding was that Hill–Sachs and Bankart lesions were significantly more prevalent in recurrent dislocations. Interestingly, the prevalence of other injuries, such as bony Bankart, HAGL, superior labrum anterior to posterior lesions, ALPSA lesions, and rotator cuff tears, did not differ substantially between first-time and recurrent events. This challenges the common assumption that such associated injuries develop primarily with recurrent instability. Several studies have documented the frequent co-occurrence of Bankart and Hill–Sachs lesions in patients with anterior shoulder instability. Widjaja et al. [2] reported a strong correlation between these lesions based on radiographic evaluations following anterior dislocations, stating that the presence of one pathology increases the risk of the other by 2.67 times. More recently, Rutgers et al. [1] conducted a systematic review and meta-analysis demonstrating that both lesions are more prevalent in recurrent dislocations, with Hill–Sachs lesions being observed in 85% and Bankart lesions in 66% of these cases, compared to lower rates in initial dislocations. In addition, Horst et al. [4] found that the likelihood of having both injuries concurrently was significantly increased by more than ten times, with larger Hill–Sachs defects being associated with a higher probability of a Bankart lesion. Together, these findings highlight that the presence of one lesion often predicts the other, especially in cases of recurrent shoulder instability, emphasizing the need for comprehensive assessment in clinical practice. The concomitant presence of these lesions is relatively rare. A systematic review done by Bui-Mansfield et al. [5] showed that approximately 62% of HAGL lesions were found to be associated with additional shoulder injuries, including general labral tears (25%), rotator cuff tears (23%), and Hill–Sachs deformities (17%). A more recent prospective study by Provencher et al. [6], which evaluated 28 patients with HAGL lesions confirmed by MR arthrogram over a 6‑year period, reported an even higher incidence of concomitant pathology: 37% of patients presented with associated labral tears alongside their HAGL lesions. However, such lesions are uncommon in single first-time anterior shoulder dislocation episodes. In fact, Shah and Selesnick [11] described the first case of a combined Bankart and HAGL lesion occurring in a single acute traumatic anterior shoulder dislocation, without recurrent instability episodes. A systematic review by Bozzo et al. [12] reported that among 120 patients with identified HAGL lesions, 15% had an associated Bankart lesion, and 13% had a concurrent Hill-Sachs lesion. Another study analyzing the MOON Shoulder Instability Cohort found that patients with HAGL lesions had significantly lower rates of Hill-Sachs lesions and anterior labral tears compared to those without HAGL lesions [3]. These findings highlight the wide spectrum of associated injuries seen with HAGL lesions; however, there is considerable variability between studies in terms of the type and frequency of concomitant pathologies reported. ALPSA lesions are observed in a meaningful subset of anterior shoulder instability cases, appearing in approximately 10% of shoulders with chronic instability, whereas HAGL lesions, although less frequent, are more often linked to acute dislocation events [13]. Meta-analytic data also identify ALPSA as a significant risk factor for recurrent instability following Bankart repair [14]. A recent systematic review and meta-analysis reported that among capsular injuries associated with anterior shoulder instability, ALPSA lesions occur in approximately 24.9% of cases, while HAGL lesions are less common at 6.2%. Although the study primarily focused on prevalence rather than treatment outcomes, the data underscore the relevance of simultaneous ALPSA and HAGL involvement [15]. While the concomitant presentation of ALPSA with Hill–Sachs or HAGL lesions is acknowledged as rare, precise prevalence data for these specific combinations remain limited in the literature. Notably, to date, no study has specifically examined the combined prevalence of ALPSA lesions, Hill–Sachs lesions, and HAGL lesions occurring together in the same patient population.
Management
Management of anterior shoulder instability with combined lesions requires an individualized approach aimed at restoring both static and dynamic joint stability. Arthroscopic ALPSA repair remains the gold standard for addressing the bony Bankart or soft-tissue lesion that heals with medial displacement on the glenoid rim due to its minimally invasive nature and consistently favorable clinical outcomes [13]. Hill–Sachs lesions are managed according to their size and engagement; small, non-engaging lesions often require no direct intervention, while engaging or large lesions benefit from arthroscopic remplissage, which has demonstrated effective restoration of shoulder stability and low recurrence rates [7,8]. HAGL lesions, once predominantly managed through open repair [16], are increasingly being treated with mini-open incisions and arthroscopically, with promising outcomes. Arthroscopic repair allows precise visualization and secure reattachment of the IGHL to its humeral insertion, preserving deltoid function and minimizing soft-tissue trauma. Recent studies have reported comparable clinical outcomes between arthroscopic and open HAGL repairs, with arthroscopic techniques associated with reduced postoperative morbidity and faster rehabilitation [6,9]. Shah and Selesnick [11] described a case involving arthroscopic Bankart repair followed by open HAGL repair, with excellent outcomes after 3 years. More recent case reports and small series suggest that a fully arthroscopic approach addressing combined lesions can achieve good functional outcomes and low recurrence, but there remains a paucity of large-scale studies to define standardized protocols and long-term efficacy [5].
Despite the well-established correlation between ALPSA or Bankart and Hill–Sachs lesions in recurrent anterior instability, and growing recognition of HAGL lesions as contributors to instability, the literature lacks systematic data concerning the prevalence and clinical significance of simultaneous ALPSA, Hill–Sachs, and HAGL lesions presenting in a single episode. The literature is also missing arthroscopic management protocols specifically addressing all three pathologies in one surgical setting and comparative outcomes of arthroscopic versus open repair in combined lesion scenarios with long-term functional results and recurrence rates following triad repair. This paucity of data limits the ability to develop standardized surgical strategies and evidence-based postoperative rehabilitation protocols tailored for such complex presentations.
In conclusion, anterior shoulder instability frequently involves ALPSA and Hill–Sachs lesions, with HAGL lesions representing a less common but important contributor to instability. The simultaneous occurrence of all three lesions presents unique diagnostic and therapeutic challenges. While arthroscopic techniques have advanced considerably, enabling minimally invasive repair of these injuries individually, combined arthroscopic repair of ALPSA, Hill–Sachs, and HAGL lesions remains underreported. Further studies are needed to clarify the optimal management approach and long-term outcomes of this rare triad to guide clinical decision-making and to demonstrate whether arthroscopic soft-tissue procedures or bone block procedures will provide such patients with better outcomes.
When multiple instability lesions coexist, clinicians should maintain a high index of suspicion, employ detailed imaging for full characterization, and consider a combined arthroscopic repair approach to address both static and dynamic stabilizers of the shoulder.
References
- 1. Rutgers C, Verweij LP, Priester-Vink S, Van Deurzen DF, Maas M, Van Den Bekerom MP. Recurrence in traumatic anterior shoulder dislocations increases the prevalence of Hill-Sachs and Bankart lesions: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 2022;30:2130-40. [Google Scholar] [PubMed]
- 2. Widjaja AB, Tran A, Bailey M, Proper S. Correlation between Bankart and Hill-Sachs lesions in anterior shoulder dislocation. ANZ J Surg 2006;76:436-8. [Google Scholar] [PubMed]
- 3. Freshman RD, Zhang AL, Benjamin Ma C, Feeley BT, Ortiz S, Patel J, et al. Factors associated with humeral avulsion of glenohumeral ligament lesions in patients with anterior shoulder instability: An analysis of the MOON shoulder instability cohort. Orthop J Sports Med 2023;11:23259671231206757. [Google Scholar] [PubMed]
- 4. Horst K, Von Harten R, Weber C, Andruszkow H, Pfeifer R, Dienstknecht T, et al. Assessment of coincidence and defect sizes in Bankart and Hill-Sachs lesions after anterior shoulder dislocation: A radiological study. Br J Radiol 2014;87:20130673. [Google Scholar] [PubMed]
- 5. Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: The HAGL lesion. Am J Sports Med 2007;35:1960-6. [Google Scholar] [PubMed]
- 6. Provencher MT, McCormick F, LeClere L, Sanchez G, Golijanin P, Anthony S, et al. Prospective evaluation of surgical treatment of humeral avulsions of the glenohumeral ligament. Am J Sports Med 2017;45:1134-40. [Google Scholar] [PubMed]
- 7. Brilakis E, Mataragas E, Deligeorgis A, Maniatis V, Antonogiannakis E. Midterm outcomes of arthroscopic remplissage for the management of recurrent anterior shoulder instability. Knee Surg Sports Traumatol Arthrosc 2016;24:593-600. [Google Scholar] [PubMed]
- 8. Villarreal-Espinosa JB, Reinold MM, Khak M, Shariyate MJ, Mita C, Kay J, et al. Rehabilitation protocol variability following arthroscopic Bankart repair and remplissage for management of anterior shoulder instability: A systematic review. Int J Sports Phys Ther 2024;19:1172-87. [Google Scholar] [PubMed]
- 9. Hartzler RU, Gutierrez-Naranjo JM. Arthroscopic management of HAGL (humeral avulsion of glenohumeral ligament) and reverse HAGL lesions. In: Lui TH, editor. Arthroscopy and Endoscopy of the Shoulder. Singapore: Springer Nature Singapore; 2023. p. 111-17. [Google Scholar] [PubMed]
- 10. Ladd LM, Crews M, Maertz NA. Glenohumeral joint instability: A review of anatomy, clinical presentation, and imaging. Clin Sports Med 2021;40:585-99. [Google Scholar] [PubMed]
- 11. Shah AA, Selesnick FH. Traumatic shoulder dislocation with combined Bankart lesion and humeral avulsion of the glenohumeral ligament in a professional basketball player: Three-year follow-up of surgical stabilization. Arthroscopy 2010;26:1404-8. [Google Scholar] [PubMed]
- 12. Bozzo A, Oitment C, Thornley P, Yan J, Habib A, Hoppe DJ, et al. Humeral avulsion of the glenohumeral ligament: Indications for surgical treatment and outcomes-a systematic review. Orthop J Sports Med 2017;5:2325967117723329. [Google Scholar] [PubMed]
- 13. Hantes M, Raoulis V. Arthroscopic findings in anterior shoulder instability. Open Orthop J 2017;11:119-32. [Google Scholar] [PubMed]
- 14. Verweij LP, Van Spanning SH, Grillo A, Kerkhoffs GM, Priester-Vink S, Van Deurzen D, et al. Age, participation in competitive sports, bony lesions, ALPSA lesions, > 1 preoperative dislocations, surgical delay and ISIS score > 3 are risk factors for recurrence following arthroscopic Bankart repair: A systematic review and meta-analysis of 4584 shoulders. Knee Surg Sports Traumatol Arthrosc 2021;29:4004-14. [Google Scholar] [PubMed]
- 15. Tisherman RT, Luo E, Briggs D, Bulleit C, Fatora G, Lau B. Glenohumeral capsular injury rate in patients with glenohumeral instability: A systematic review and meta-analysis. JSES Rev Rep Tech 2024;4:762-7. [Google Scholar] [PubMed]
- 16. George MS, Khazzam M, Kuhn JE. Humeral avulsion of glenohumeral ligaments. J Am Acad Orthop Surg 2011;19:127-33. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations
July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations July 1, 2026 Arthroscopic Rotator Cuff Repair with Versus Without Acromioplasty: A Comparative Clinical Outcome Study
July 1, 2026 Arthroscopic Rotator Cuff Repair with Versus Without Acromioplasty: A Comparative Clinical Outcome Study May 1, 2025 Comprehensive Arthroscopic Management of Multi-ligament Knee Injury: A Case Report
May 1, 2025 Comprehensive Arthroscopic Management of Multi-ligament Knee Injury: A Case Report December 1, 2024 Functional and Radiological Outcome of Meniscal Repair and Conservative Management for Medial Meniscal Root Tear – A Prospective Comparative Study
December 1, 2024 Functional and Radiological Outcome of Meniscal Repair and Conservative Management for Medial Meniscal Root Tear – A Prospective Comparative Study