
Thoracic outlet syndrome should be considered when evaluating patients with upper limb neurological symptoms, especially in the absence of clear cervical pathology and when pain is atypical – non-dermatomal and clinical signs are subtle with no obvious neurological deficits, with first rib fracture being one of the possible etiological factor.
Dr. Arjun Ganesh, Senior Resident, Department of Orthopedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai, Tamil Nadu, India- 600116. Email: drarjunganeshjournal@gmail.com
Abstract
Introduction: Thoracic outlet syndrome (TOS) results from compression of the neurovascular structures within the thoracic outlet. Neurogenic TOS (NTOS) is the most common subtype and often presents with non-specific upper-limb neurological symptoms, making diagnosis challenging. First rib pathology as a cause of NTOS is rare and may delay recognition and treatment.
Case Report: A 21-year-old male presented with progressive pain, paresthesia, and weakness of the left upper limb for 2 months, aggravated by overhead activities. Clinical examination revealed reduced motor power in the C7, C8, and T1 myotomes with decreased grip strength. Provocative tests for thoracic outlet compression were positive. Computed tomography demonstrated a fractured first rib with mixed lytic–sclerotic changes causing narrowing of the costoclavicular space and compression of the brachial plexus. Magnetic resonance imaging showed edema of the brachial plexus, and nerve conduction studies supported brachial plexopathy. Due to progressive neurological deficits, surgical decompression was performed through a supraclavicular approach, including first rib excision, anterior scalenectomy, and pectoralis minor tendon tenotomy. Postoperatively, the patient showed significant improvement in pain, sensory symptoms, and motor strength.
Conclusion: NTOS should be considered in patients presenting with unexplained upper-limb neurological symptoms, particularly when conventional investigations are inconclusive. Identification of rare etiologies, such as first rib pathology and timely surgical decompression, can lead to excellent functional outcomes.
Keywords: Thoracic outlet syndrome, neurogenic thoracic outlet syndrome, first rib fracture, brachial plexus compression, supraclavicular approach.
Thoracic outlet syndrome (TOS) encompasses a group of symptoms arising from compression of the brachial plexus, subclavian artery, or subclavian vein as these neurovascular structures traverse the thoracic outlet [1]. Based on the predominant structure involved, TOS is classified into neurogenic, venous, arterial, traumatic, and disputed types, with neurogenic TOS accounting for more than 90% of cases and commonly presenting with upper-limb pain, paresthesia, weakness, and functional impairment. [1]. Diagnosis remains largely clinical, with imaging and nerve conduction studies serving as adjunctive tools [2]. We report a rare case of neurogenic TOS secondary to a first rib fracture, presenting with brachial plexus compression. The case highlights diagnostic difficulty, the role of multimodal evaluation, and the importance of surgical decompression in symptomatic patients.
A 21-year-old gentleman presented with progressive pain and weakness in his left forearm and hand for past 2 months. Symptoms were insidious and aggravated by overhead activities. He had a history of lifting heavy weights but denied trauma, constitutional symptoms, or fever. On examination, muscle power in the left upper limb was reduced – C7 (wrist extension), C8 (finger flexion), and T1 (little finger abduction) all graded 4/5 on the Medical Research Council scale. Grip strength was significantly diminished. Provocative tests, including Roo’s test, upper limb stress test, costoclavicular maneuver were positive and coracoid compression reproduced symptoms consistent with neurogenic TOS (Table 1).
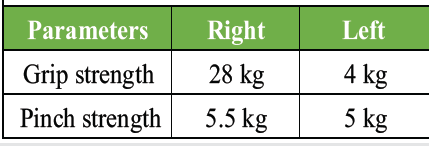
Table 1: Grip and pinch strength
There was no visible swelling, lymphadenopathy, or vascular symptoms. Sensory examination showed patchy paresthesia without dermatomal distribution. There was pain and paresthesia over the supraclavicular region, shoulder, axilla, anterior aspect of the middle third arm, anterior aspect of forearm, ventral and dorsal aspect of hand.
Investigations
Computed tomography (CT) chest revealed cortical discontinuity of the lateral first rib with mixed lytic–sclerotic changes, subtle periosteal reaction, and mild soft-tissue inflammation. The lesion was seen indenting the divisions of the left brachial plexus and closely abutting the left subclavian artery (Fig. 1 and 2).
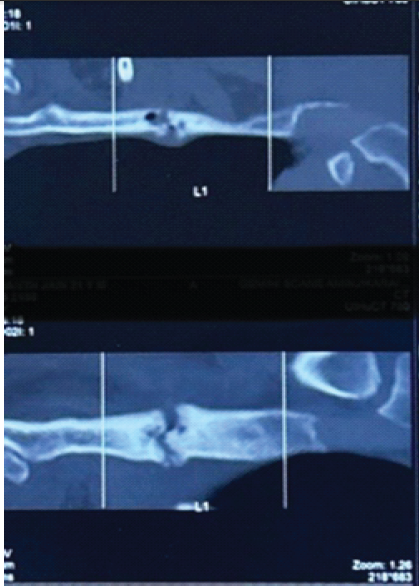
Figure 1: Computed tomography film showing fractured first rib with mixed lytic and sclerotic changes and periosteal reaction.
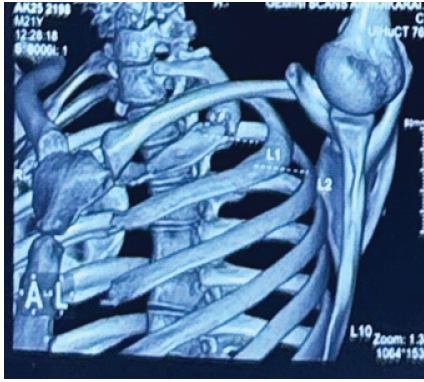
Figure 2: Three dimensional computed tomography reconstruction of the chest showing the location of the first rib fracture and reduced costoclavicular space, causing potential compression of the brachial plexus.
Magnetic resonance imaging (MRI) C-spine demonstrated short tau inversion recovery hyperintense signal in the left brachial plexus divisions and cords, along with edema along the first rib margins (Fig. 3)
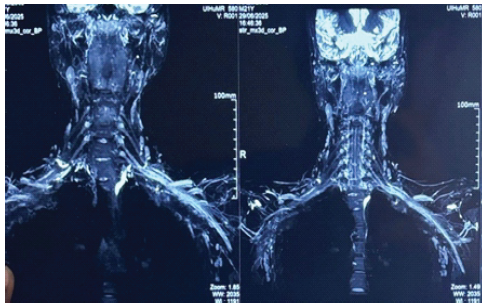
Figure 3: Magnetic resonance imaging C-spine demonstrated a short tau inversion recovery hyperintense signal in the left brachial plexus divisions and cords.
Motor study of the upper limb showed right median and ulnar nerve shows normal compound muscle action potential (CMAP) amplitude, latencies, and conduction velocity and left median and ulnar nerve shows reduced CMAP amplitude, latencies and conduction velocity. Left pronator nerves were reduced amplitude compared to the right side. Sensory study in upper limbs showed right median and ulnar sensory nerves show reduced sensory nerve action potential (SNAP) amplitude, with normal latencies and conduction velocity. Left median and ulnar sensory nerves show reduced SNAP amplitude, with normal latencies and conduction velocity, and the left 4th digit sensory nerve shows reduced amplitude compared to the right side. F-RESPONSE latencies from both median and ulnar nerves were normal. Nerve conduction study suggestive of left polyradiculopathy versus brachial plexopathy.
Management
Due to progressive symptoms and radiological evidence of compression, surgical intervention was planned. The patient underwent left brachial plexus exploration, anterior scalenectomy, first rib excision through supraclavicular approach, and pectoralis minor tendon tenotomy (PMT). The patient is positioned supine with a shoulder roll to facilitate neck extension, and the head is rotated to the contralateral side. A transverse or oblique incision is placed approximately 1–2 cm superior to the clavicle. After division of the platysma, the supraclavicular fat pad is mobilized, with careful identification and preservation of the supraclavicular nerves. The phrenic nerve is identified along the anterior scalene muscle and protected throughout the procedure. Scalenectomy was performed as indicated, followed by exposure of the brachial plexus trunks, allowing neurolysis. Intraoperatively, it was found that the fibrosis and bony irregularity around the first rib contributed to narrowing of the costoclavicular space, which resulted in the compression of the neurovascular structures. Following excision of the first rib, the compression was released at the costoclavicular junction. Through deltopectoral approach, identification and division of the pectoralis minor at the insertion of the coracoid process, and surgical decompression of the infraclavicular portion of the brachial plexus was done. Throughout the procedure, the brachial plexus motor integrity was checked with a nerve stimulator and was found to be intact (Fig. 4,5,6,7). Histopathology of the excised rib showed fibrocartilage and bony fragments with areas of fibrosis and congestion.
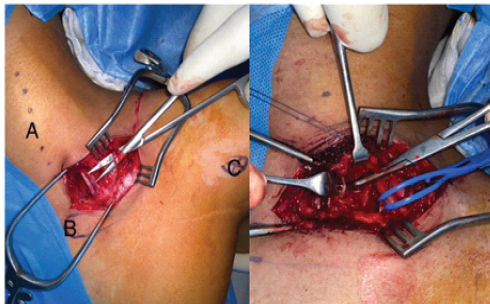
Figure 4: Intraoperative image showing supraclavicular plexus and phrenic nerve, which lies directly over the anterior scalene muscle anteromedially to the brachial plexus.
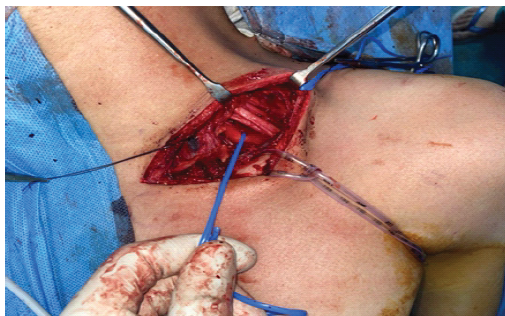
Figure 5: Intraoperative image showing divisions of brachial plexus, middle third clavicle, and subclavian vessels.
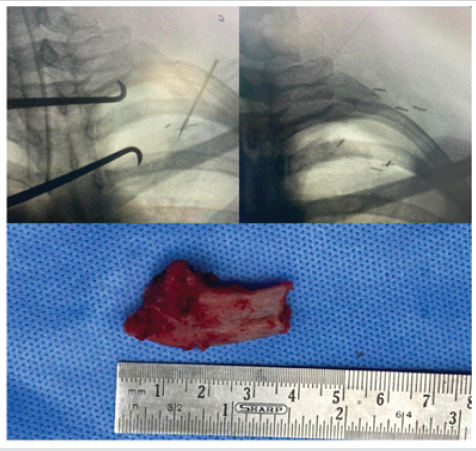
Figure 6: Intraoperative C-arm images showing part of the first rib before and after excision at the costoclavicular junction and the excised portion of the first rib.
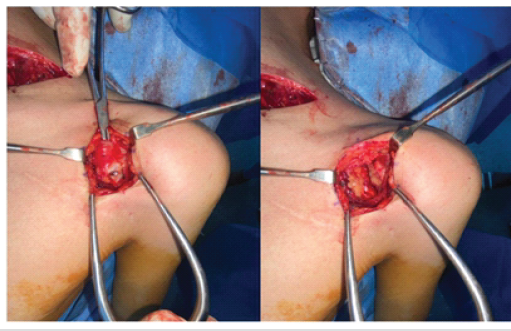
Figure 7: Intraoperative images showing pectoralis minor tendon tenotomy near the coracoid process.
Post-operative outcome
At 4 months follow-up, the patient reported a marked reduction in pain and paresthesia, with significant improvement in grip strength and motor power. There were no post-operative complications. Return to daily activities occurred by 8 weeks post-surgery.
Neurogenic TOS (NTOS) remains a well-recognized diagnostic challenge due to its non-specific clinical presentation and significant symptom overlap with cervical radiculopathy, peripheral neuropathies, brachial plexopathy, and distal entrapment syndromes [3,4]. Patients commonly report neck, shoulder, and upper-limb pain accompanied by paresthesia, weakness, and fatigability, symptoms that are often positional or exacerbated by overhead activities. Because no single clinical test or investigation is pathognomonic, diagnosis is primarily clinical, supported by exclusion of other causes [1]. The role of imaging in NTOS is largely adjunctive, with conventional radiographs, CT, and MRI mainly employed to identify structural abnormalities and rule out alternative etiologies [5]. Dynamic imaging may demonstrate positional narrowing of the thoracic outlet; however, radiological findings often lack specificity. Electrodiagnostic studies, while frequently normal, can provide supportive evidence of brachial plexus involvement and are particularly useful in excluding cervical radiculopathy or peripheral nerve entrapment [2]. In the present case, first rib pathology was identified as the causative factor for brachial plexus compression, representing a rare but documented cause of NTOS. Structural abnormalities of the first rib – including anomalous morphology, callus formation, or post-traumatic changes – have been reported to contribute to neurovascular compression within the thoracic outlet [6]. Based on the clinical history and histopathological report suggests that the repeated weight lifting might have caused the first rib stress fracture, which shows the features of fibrous union with no evidence of malignancy or infection. Cross-sectional imaging with CT and MRI played a pivotal role in accurately delineating the underlying anatomy and guiding surgical planning, while nerve conduction studies corroborated neurological compromise. Surgical decompression is indicated in patients with progressive neurological symptoms, functional impairment refractory to conservative management, or definitive radiological evidence of compression [7]. Among surgical options, scalenectomy combined with first rib excision has demonstrated favorable outcomes by effectively enlarging the thoracic outlet and relieving brachial plexus compression. Several studies report significant symptomatic improvement and functional recovery following appropriately selected surgical intervention [8,9]. The supraclavicular approach provides excellent exposure of the upper and middle trunks of the brachial plexus as they emerge between the anterior and middle scalene muscles [3]. This approach is commonly employed in the management of NTOS, brachial plexus tumors, traumatic plexus injuries, and selected reconstructive procedures. Its principal advantage lies in direct visualization of the brachial plexus proximal to its branching, allowing precise decompression and targeted neurolysis [1]. In patients with NTOS, the supraclavicular approach enables effective decompression of the brachial plexus by addressing compressive structures such as fibrous bands, cervical ribs, anomalous first ribs, or hypertrophied scalene muscles. When combined with first rib excision, this approach offers durable symptomatic relief and permits safe handling of neurovascular structures under direct vision. Compared with the transaxillary approach, the supraclavicular route provides superior exposure of neural elements and is particularly advantageous in complex, recurrent, or anatomically variant cases [6]. Potential complications include phrenic nerve palsy, brachial plexus injury, pneumothorax, and vascular injury; however, these risks are minimized with meticulous surgical technique and sound anatomical knowledge. Overall, the supraclavicular approach represents a safe, versatile, and effective surgical corridor for brachial plexus decompression and reconstruction in appropriately selected patients [9]. PMT has emerged as an important adjunctive or alternative surgical procedure in selected patients with TOS, particularly those with symptoms arising from compression in the subcoracoid space. Compression of the neurovascular bundle beneath the pectoralis minor tendon, often referred to as pectoralis minor syndrome, may coexist with or mimic NTOS [10]. Surgically, PMT is performed through a deltopectoral or infraclavicular approach, allowing identification and division of the pectoralis minor tendon at its insertion on the coracoid process. This maneuver relieves anterior traction on the neurovascular structures and effectively decompresses the infraclavicular portion of the brachial plexus. PMT may be performed as a stand-alone procedure in isolated pectoralis minor syndrome or in combination with supraclavicular decompression and first rib excision in patients with multilevel compression [11]. Several studies have demonstrated favorable outcomes following PMT, with significant improvement in pain, paresthesia, and upper-limb function, particularly when patients are appropriately selected based on clinical and radiological findings [9]. Hence, for our patient, along with surgical excision of the first rib and anterior scalenectomy, PMT was also done in accordance with the clinical and neurological correlation. This case highlights the importance of maintaining TOS in the differential diagnosis of atypical upper-limb neurological symptoms, particularly when initial investigations are inconclusive. Early diagnosis and timely intervention are essential to prevent chronic neurological deficits and to optimize patient outcomes.
TOS should be considered when evaluating patients with upper limb neurological symptoms, especially in the absence of clear cervical pathology. Early recognition, multimodal diagnostic evaluation, and appropriate surgical management can lead to excellent functional recovery.
Diagnosing TOS, a condition requiring exclusion of other causes, ranging from very subtle to excruciating pain, benefits from surgical decompression – Scalenectomy, First rib excision, Pectoralis minor tendon tenotomy.
References
- 1. Sanders RJ, Hammond SL, Rao NM. Diagnosis of thoracic outlet syndrome. J Vasc Surg 2007;46:601-4. [Google Scholar] [PubMed]
- 2. Huang JH, Zager EL. Thoracic outlet syndrome. Neurosurgery 2004;55:897-902; discussion 902-3. [Google Scholar] [PubMed]
- 3. Atasoy E. Thoracic outlet syndrome: Anatomy, diagnosis, and treatment. J Hand Surg Am 2004;29:115-23. [Google Scholar] [PubMed]
- 4. Wilbourn AJ. Thoracic outlet syndrome is overdiagnosed. Muscle Nerve 1999;22:130-6; discussion 136-7. [Google Scholar] [PubMed]
- 5. Peek J, Vos CG, Ünlü Ç, Van De Pavoordt HD, Van Den Akker PJ, De Vries JP. Outcome of surgical treatment for thoracic outlet syndrome: Systematic review and meta-analysis. Ann Vasc Surg 2017;40:303-26. [Google Scholar] [PubMed]
- 6. Roos DB. Congenital anomalies associated with thoracic outlet syndrome. Anatomy, symptoms, diagnosis, and treatment. Am J Surg 1976;132:771-8. [Google Scholar] [PubMed]
- 7. Povlsen B, Hansson T, Povlsen SD. Treatment for thoracic outlet syndrome. Cochrane Database Syst Rev 2014;11:CD007218. [Google Scholar] [PubMed]
- 8. Illig KA, Rodriguez-Zoppi E, Bland T, Muftah M, Jospitre E. The incidence of thoracic outlet syndrome. Ann Vasc Surg 2021;70:263-72. [Google Scholar] [PubMed]
- 9. Likes K, Rochlin DH, Call D, Freischlag JA. Long-term outcomes of surgical treatment for neurogenic thoracic outlet syndrome. Ann Vasc Surg 2014;28:1899-907. [Google Scholar] [PubMed]
- 10. Sanders RJ, Rao NM. The forgotten pectoralis minor syndrome: 100 operations for pectoralis minor syndrome alone or accompanied by neurogenic thoracic outlet syndrome. Ann Vasc Surg 2010;24:701-8. [Google Scholar] [PubMed]
- 11. Thompson RW, Driskill MR. Surgical management of thoracic outlet syndrome. Hand Clin 2004;20:57-69. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 September 29, 2019 SubcapitalNeck of Femur Fracture in a Case of Osteonecrosis of Femoral Head – Rare Presentation
September 29, 2019 SubcapitalNeck of Femur Fracture in a Case of Osteonecrosis of Femoral Head – Rare Presentation October 10, 2021 A Case Series of Acute Painless Bilateral Foot Drop Without Cauda Equina Syndrome
October 10, 2021 A Case Series of Acute Painless Bilateral Foot Drop Without Cauda Equina Syndrome January 10, 2017 Editorial – Formation of New Reviewers Board – A JOCR initiative
January 10, 2017 Editorial – Formation of New Reviewers Board – A JOCR initiative October 10, 2021 Heterotopic Ossification after Open Anchor Fixation of the Posterior Cruciate Ligament Avulsion in a Multiligament Injury of the Knee: A Case Report
October 10, 2021 Heterotopic Ossification after Open Anchor Fixation of the Posterior Cruciate Ligament Avulsion in a Multiligament Injury of the Knee: A Case Report