
Irreducible thumb IP joint dislocations are often due to soft-tissue interposition, and early surgical exploration ensures optimal functional outcomes.
Dr. Subashini R, Department of Hand Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: doctor.subashini@ymail.com
Abstract
Introduction: Dislocations of the thumb interphalangeal (IP) joint are rare injuries because of the stability of the collateral ligaments, volar plate, and surrounding tendons, with open and irreducible cases being especially uncommon.
Case Report: We present a case of a 49-year-old male who suffered an open injury to his left thumb in a road traffic accident, resulting in an IP joint dislocation and exposed proximal phalanx bone. Emergency wound debridement and reduction were carried out, but the reduction was obstructed by the flexor pollicis longus tendon encircling the proximal phalanx bone. Following tendon repositioning, reduction was successfully achieved and maintained using a 1.2 mm Kirschner wire. The K-wire was removed at 4 weeks, and by the 3-month follow-up, the patient had achieved satisfactory clinical and functional recovery.
Conclusion: This case underscores the significance of identifying soft tissue interference as a cause of irreducibility and highlights the critical role of early surgical intervention and stabilization in securing favorable outcomes.
Keywords Thumb IP joint dislocation, irreducible dislocation, flexor pollicis longus, open dislocation, K-wire fixation.
Dislocations of the thumb interphalangeal (IP) joint are relatively uncommon injuries, largely because of the intrinsic stability offered by strong capsuloligamentous structures and surrounding tendons. These injuries typically occur when an axial force is applied to an extended thumb, most commonly causing the distal phalanx to displace dorsally. While closed IP joint dislocations are more common and typically managed with closed reduction, open and irreducible cases are rare, more complex, and often necessitate surgical intervention. Irreducible dislocations of the thumb’s IP joint are usually caused by soft tissue structures – such as the volar plate, flexor pollicis longus (FPL) tendon, sesamoid bones, or osteochondral fragments – becoming interposed within the joint. These structures can form a barrier for successful closed reduction and may not be visible on standard radiographs. Consequently, failed initial reduction efforts should raise suspicion of interposed structures and necessitate early surgical exploration. Open dislocations of the thumb IP joint are particularly rare, with only a handful of cases documented in the literature. They also pose further challenges, such as contamination, soft-tissue damage, and potential neurovascular compromise. Prompt diagnosis, appropriate imaging, and careful surgical management are essential to restore joint alignment, preserve function, and minimize long-term complications such as stiffness or instability. In this context, we present a surgical case report of an acute, irreducible, compound dorsal dislocation of the thumb IP joint, emphasizing the mechanisms of irreducibility, intraoperative observations, and functional outcomes. This study underscores the critical role of early diagnosis and comprehensive management in securing optimal clinical outcomes.
A 49-year-old male with no comorbidities presented with a history of a road traffic accident and sustained an open injury to the left thumb. On examination, an open wound was present over the ulnar aspect of the thumb; the proximal phalanx bone was protruding through the wound, and IP joint dislocation was present with mild contamination. The thumb was sensate and viable (Fig. 1).

Figure 1: Clinical pictures of the left thumb at the time of presentation showing the proximal phalanx protruding through the open wound.
X-ray anteroposterior (Fig. 2a) and lateral views (Fig. 2b) of the left thumb were taken, which revealed dorsal dislocation of the IP joint of the thumb without fracture.
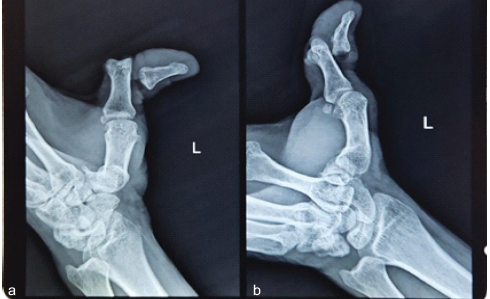
Figure 2: (a and b) X-ray anteroposterior and lateral views of the left thumb showing
thumb interphalangeal joint dislocation.
The patient underwent emergency wound debridement with open reduction and K-wire fixation under a supraclavicular block. Intraoperatively, the FPL tendon was found to be intact. However, it was displaced dorsally around the proximal phalanx shaft, preventing reduction (Fig. 3).
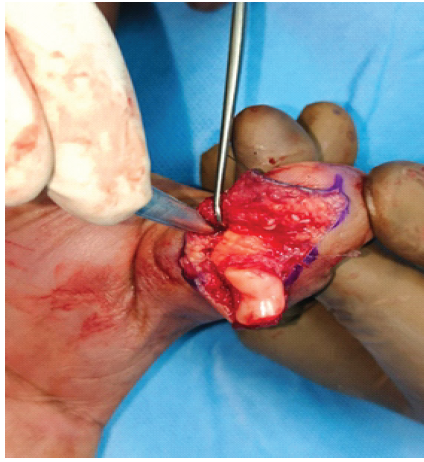
Figure 3: Intraoperative picture showing flexor pollicis longus tendon
interposed within the interphalangeal joint.
The FPL insertion in the distal phalanx was uninjured. Once the tendon was manipulated and repositioned, reduction was achieved. The volar plate injury and the ulnar collateral ligament of the IP joint were injured. The ulnar-side digital artery (Fig. 4a) and digital nerve (Fig. 4b) of the thumb were not injured. Subsequently, the thumb IP joint was immobilized with an axial 1.2 mm K-wire to facilitate healing of soft tissue (Fig. 5). Radiographs were taken on the 1st post-operative day (Fig. 6), which revealed satisfactory reduction.
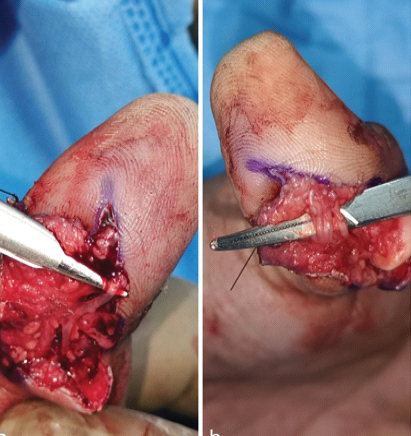
Figure 4: Intraoperative pictures of the ulnar side (a) digital artery and (b)
digital nerve, which were found to be intact.

Figure 6: 1st post-operative day X-ray of left thumb shows satisfactory
reduction.
Postoperatively, the patient was followed up regularly and started on mobilization of the metacarpophalangeal and carpo-metacarpophalangeal joints of the thumb. The K-wire was removed at 4 weeks, and then the patient started on IP joint movements. At the 3-month follow-up, the patient had active, pain-free flexion of 0–45° of the IP joint of the thumb. The patient was able to do all his day-to-day activities.
Thumb IP joint dislocations are rare injuries owing to the strong stabilizing effect of the collateral ligaments, volar plate, and surrounding tendons [1,2]. Most commonly, these injuries result from axial loading with hyperextension, leading to dorsal displacement of the distal phalanx [3]. While closed dislocations are typically amenable to closed reduction, irreducible and open dislocations remain uncommon and clinically significant entities.
Failure of closed reduction is most frequently due to interposition of soft tissue structures, particularly the volar plate. Brown et al. reported that avulsion and interposition of the volar plate from the proximal phalanx is the most common cause of irreducibility [4]. Other structures implicated include the FPL tendon, sesamoid bones, osteochondral fragments, and rarely digital nerves [1,5]. Shah et al. described a case of irreducible thumb IP joint dislocation with digital nerve interposition along with the FPL tendon and volar plate, highlighting the complexity of these injuries [6]. Similarly, Salamon and Gelberman demonstrated that either the volar plate or the FPL tendon can act as a mechanical block to reduction [7]. Mohan et al. and Sabapathy et al. further reported cases where sesamoid bone or combined soft-tissue structures were responsible for irreducibility [8,9]. Naito et al. described a similar case to ours where the displaced FPL prevented reduction in closed IP joint dorsal dislocation of the thumb and required surgical manipulation [10].
Open dislocations of the thumb IP joint are particularly rare, with very few cases described in the literature [1,2]. These injuries are often associated with high-energy trauma such as road traffic accidents and carry increased risks of contamination, soft-tissue damage, and neurovascular compromise. Literature consistently emphasizes that open injuries frequently present as irreducible dislocations requiring surgical intervention [4]. Radiographic evaluation remains essential; however, it may not reveal soft tissue interposition. Persistent joint incongruity after attempted reduction should raise suspicion of a complex dislocation [3]. Although MRI can delineate soft-tissue pathology, it is rarely required in acute settings, as failure of closed reduction itself is an indication for operative exploration.
Management strategies described in the literature uniformly advocate early surgical exploration in irreducible cases [1,4,7]. The objective is to identify and remove the obstructing structure, restore joint congruity, and assess stability. K-wire fixation is commonly used to maintain reduction, especially in unstable joints [2,11]. Early mobilization following a short period of immobilization is essential to prevent stiffness and ensure functional recovery [3]. In the present case, irreducibility was due to dorsal displacement of the FPL tendon, which is consistent with previously reported mechanisms [7,10]. Prompt surgical intervention with debridement, tendon repositioning, and K-wire fixation resulted in satisfactory clinical and functional outcomes at 3 months, reinforcing the importance of early definitive management.
This case highlights the rarity and clinical complexity of acute compound irreducible dorsal dislocations of the thumb IP joint. The presence of soft tissue interposition – particularly the FPL tendon – should be strongly suspected when closed reduction fails. Open injuries further increase the risk of contamination and associated soft-tissue damage, necessitating prompt surgical intervention. Early exploration, identification, and release of the obstructing structure, followed by stable fixation using K-wire, ensures restoration of joint congruity and facilitates optimal functional recovery. Timely management, combined with appropriate post-operative rehabilitation, is essential in achieving satisfactory clinical outcomes and preventing long-term complications such as stiffness or instability.
Irreducible thumb IP joint dislocations are frequently caused by soft tissue interposition and should not undergo repeated forceful reduction attempts; early surgical exploration and stabilization are key to preserving function and ensuring favourable outcomes.
References
- 1. Green DP, Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH. Green’s Operative Hand Surgery. 7th ed. Philadelphia, PA: Elsevier; 2017. [Google Scholar] [PubMed]
- 2. Wolfe SW, Pederson WC, Kozin SH, Cohen MS. Operative Techniques in Hand, Wrist, and Forearm Surgery. Philadelphia, PA: Elsevier; 2013. [Google Scholar] [PubMed]
- 3. Stern PJ. Fractures of the metacarpals and phalanges. J Am Acad Orthop Surg. 1997;5:305-13. [Google Scholar] [PubMed]
- 4. Brown DJ, Parcells AL, Granick MS. Thumb interphalangeal joint dislocation. Eplasty 2016;16:ic02. [Google Scholar] [PubMed]
- 5. Bowers WH. The interphalangeal joints. In: Green DP, editor. Operative Hand Surgery. New York: Churchill Livingstone; 1993. p. 611-50. [Google Scholar] [PubMed]
- 6. Shah SR, Bindra R, Griffin JW. Irreducible dislocation of the thumb interphalangeal joint with digital nerve interposition: Case report. J Hand Surg Am 2010;35:422-4. [Google Scholar] [PubMed]
- 7. Salamon PB, Gelberman RH. Irreducible dislocation of the interphalangeal joint of the thumb. J Bone Joint Surg Am 1978;60:400-1. [Google Scholar] [PubMed]
- 8. Mohan BV, Kishan S, Munshi P, Pathak RH, Pandit H. Irreducible dislocation of the interphalangeal joint of the thumb. J Postgrad Med 1996;42:30-1. [Google Scholar] [PubMed]
- 9. Sabapathy SR, Bose VC, Rex C. Irreducible dislocation of the interphalangeal joint of the thumb due to sesamoid bone interposition: A case report. J Hand Surg Am 1995;20:487-9. [Google Scholar] [PubMed]
- 10. Naito K, Sugiyama Y, Igeta Y, Kaneko K, Obayashi O. Irreducible dislocation of the thumb interphalangeal joint due to displaced flexor pollicis longus tendon: Case report and new reduction technique. Arch Orthop Trauma Surg 2014;134:1175-8. [Google Scholar] [PubMed]
- 11. McCue FC, Meister K. Common sports hand injuries. Clin Sports Med 1992;11:309-25. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Chondromyxoid Fibroma of the Right Thumb: Successful Management with Wide Local Excision, Iliac Crest Bone Grafting and K-Wiring – A Rare Case Report
April 1, 2026 Chondromyxoid Fibroma of the Right Thumb: Successful Management with Wide Local Excision, Iliac Crest Bone Grafting and K-Wiring – A Rare Case Report January 1, 2026 Timely Intervention Saves the Limb in a 7-Year-old Child with Distal Femoral Physeal Injury: A Case Report
January 1, 2026 Timely Intervention Saves the Limb in a 7-Year-old Child with Distal Femoral Physeal Injury: A Case Report August 10, 2023 Giant Cell Tumor of Flexor Pollicis Longus Tendon Sheath: An Uncommon Case Report and Literature Review
August 10, 2023 Giant Cell Tumor of Flexor Pollicis Longus Tendon Sheath: An Uncommon Case Report and Literature Review July 10, 2020 Open Interphalangeal Dislocation of the Great Toe in an Amateur Football Player: A Rare Case Report
July 10, 2020 Open Interphalangeal Dislocation of the Great Toe in an Amateur Football Player: A Rare Case Report