
Wide local excision with preservation of endplates combined with iliac crest bone grafting and K-wire fixation can effectively restore stability and function in rare cases of chondromyxoid fibroma of the thumb while minimizing recurrence risk.
Dr. Jaideep Das, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: jaideepdas01@gmail.com
Abstract
Introduction: Chondromyxoid fibroma (CMF) is a rare, benign cartilaginous tumor that typically affects long bones but rarely involves the small bones of the hand. This case report presents a unique occurrence of CMF in the right thumb, managed through surgical resection, K-wiring, and iliac crest bone grafting (ICBG).
Case Report: A 51-year-old male presented to our facility with complaints of pain and swelling at the base of his right thumb, persisting for 2 months. The pain was initially managed with home remedies. However, the patient noted progressive swelling after 1 month, prompting him to seek medical attention. Physical examination and imaging studies revealed a mass involving the first metacarpal. A lazy-S incision was made over the affected area. Wide local excision of the tumor in the 1st metacarpal with preservation of endplates, along with the involved first metacarpal, was performed. A tri-cortical graft from the iliac crest, shaped to match the defect, was then placed, and stabilization was achieved using four K-wires under C-arm guidance in a cross configuration. CMF in the hand is rare, and its presence in the thumb poses unique challenges for both diagnosis and treatment. While CMF is typically benign, its local recurrence rate warrants careful surgical planning and follow-up. Resection with structural grafting and K-wire fixation in this case allowed for effective restoration of thumb stability and function.
Conclusion: This case demonstrates successful management of thumb CMF through wide local excision of the tumor of the 1st metacarpal with preservation of endplates, tri-cortical ICBG, and K-wire fixation. The patient is expected to regain functional use of the thumb, emphasizing the importance of tailored surgical approaches in rare tumor presentations.
Keywords: Chondromyxoid fibroma, thumb tumor, iliac crest bone graft, K-wire fixation, rare case.
Chondromyxoid fibroma (CMF) is a rare, benign cartilaginous tumor that comprises <1% of all bone tumors, typically presenting in the second and third decades of life [1]. CMF primarily affects the metaphyseal regions of long bones, particularly the proximal tibia and femur, but is rarely found in the bones of the hands and feet [1,2,3,4,5]. It is seen more frequently in males rather than in females [6]. In cases where CMF involves the hand, it most commonly affects the phalanges or metacarpals, and its presence in the thumb is exceedingly unusual. The rarity of CMF in the hand, particularly in the thumb, presents unique diagnostic and therapeutic challenges for clinicians [1]. Patients with CMF commonly present with insidious symptoms, including localized pain and swelling, often exacerbated by activity [7]. In most cases, symptoms progress gradually, but in some cases, pain may acutely worsen, prompting medical consultation. Due to its benign nature, CMF generally grows slowly, but it can cause significant pain, joint instability, and functional impairment in affected bones. Radiographically, CMF may appear as a lytic, well-demarcated lesion, often showing a lobulated pattern that can mimic other benign and malignant bone tumors. Biopsy and histopathological analysis are essential for accurate diagnosis, as the tumor can be challenging to distinguish from other cartilaginous lesions on imaging alone [1]. Chondroma, in particularly, can be difficult to distinguish since the histological border of this one with chondrosarcoma is very similar, as well as from chondroblastoma and giant cell tumor [8,9]. The management of CMF typically involves surgical intervention [7]. The primary approach is en bloc resection or curettage to ensure complete removal of the lesion and reduce the risk of local recurrence, which is estimated to range from 12.5% to 25% [7,10,11]. Reconstruction options include bone grafting, which provides a robust and structurally sound graft. Stabilization with K-wires or other fixation methods may be necessary, particularly when there is substantial bone involvement, to promote healing and functional recovery. This case report presents a rare occurrence of CMF involving the right thumb metacarpal in a 51-year-old male. The patient was successfully managed with wide local excision of the tumor while preserving the articular endplates, followed by reconstruction using an autologous iliac crest bone graft (ICBG) and stabilization with K-wire fixation. This surgical strategy was chosen to maintain thumb length, restore structural stability, and preserve functional mobility. The case highlights the importance of individualized surgical planning in the management of rare bone tumors located in functionally critical anatomical regions, with emphasis on achieving oncological clearance while optimizing functional outcomes.
A 51-year-old male, right-hand dominant, presented with a 2-month history of pain and swelling at the base of his right thumb. The pain was acute in onset and gradually progressive. Initially, he managed the symptoms with home remedies, but the pain persisted, and after a month, he noticed swelling at the same site, which progressively increased to its current size. Physical examination revealed tenderness and swelling localized over the first metacarpal of the right hand (Fig. 1).

Figure 1: Pre-operative right-hand clinical pictures.
Magnetic resonance imaging was suggestive of a lytic expansile enhancing lesion involving the right 1st metacarpal bone with thinning and break in overlying cortex with associated soft-tissue swelling measuring approximately 3.9 × 3.0 × 4.4 cm in size with the lesion not crossing the 1st carpo-metacarpal joint (Fig. 2). The plan was to excise the lesion in toto and replace the defect with a tri-cortical bone graft from the iliac crest, and send the sample for histopathological study with the differential diagnosis including – CMF, giant cell tumor, and enchondroma.
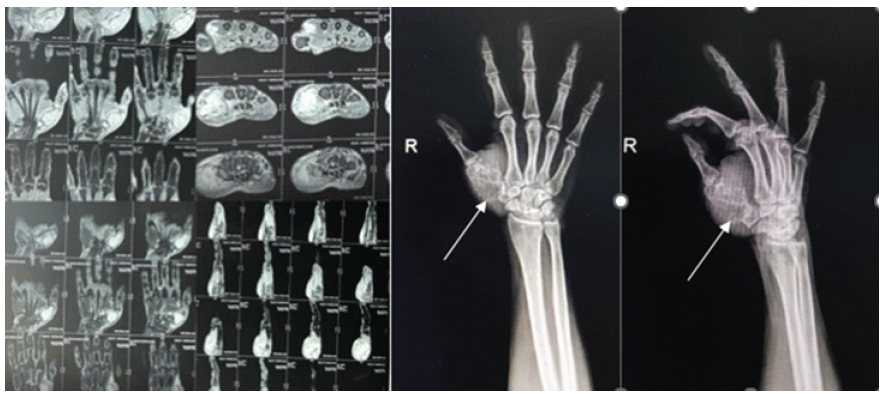
Figure 2: Pre-operative magnetic resonance imaging and X-rays.
Operative procedure
Under a supraclavicular block regional anesthesia, the patient was positioned for surgery, and a tourniquet was applied to the upper arm. A lazy-S incision was made over the base of the right thumb to provide adequate exposure. Dissection was carefully carried down to the level of the metacarpal, preserving surrounding soft tissues and neurovascular structures. A wide local excision of the tumor with preservation of the endplates of the 1st metacarpal both proximally and distally, with a thickness of 5 mm, was performed. After excision, we curated the end plate. The excised mass measured approximately 4.6 cm (Fig. 3 and 4).
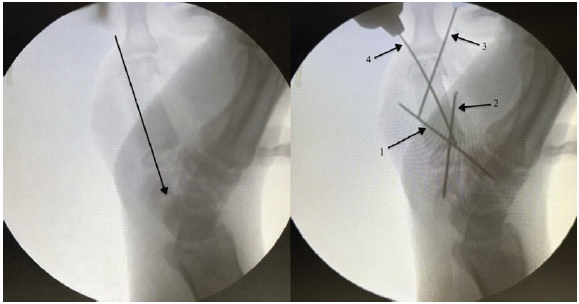
Figure 3: Intraoperative c-arm Image
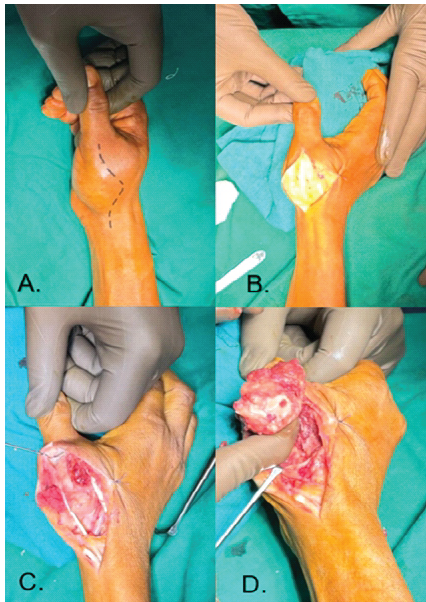
Figure 4: IntraOperative steps and findings.
A tricortical ICBG was harvested, measuring 5 cm, and the edges were smoothed, locked, and aligned into the end plate to fit the metacarpal defect as an en bloc graft within the resected area. First, a temporary K-wire of 1 mm was passed through the ICBG in a distal-to-proximal direction. Once the graft was positioned at the defect site, the wire was advanced to achieve fixation with the trapezium and scaphoid. Following that, the 1st and 2nd K-wires were inserted from distal to proximal in a cross configuration crossing from the graft, proximal end plate, and then the carpal bone. The temporary wire, which was initially placed, was removed. Then, the 3rd K-wire was inserted from the ulnar side, crossing the distal end plate and the graft. Finally, the 4th K-wire was inserted from the radial side, crossing the distal end plate and the graft. All the K-wires were cut and buried; wound closure was done (Fig. 4).
Post-operative Rehabilitation and Follow-up
The patient was placed in a thumb spica slab immediately after surgery for 2 weeks to provide immobilization and reduce stress on the surgical site. Post that sutures were removed and a thumb spica cast was applied for 6 weeks. During follow-up visits at 3 and 6 weeks, X-rays were done, which showed satisfactory graft positioning and bone healing. After 6 weeks, the cast was removed, and gradual mobilization of the interphalangeal (IP) joint and wrist joint was started. By 12 weeks, X-rays showed complete consolidation of the graft with endplates, and K-wires were removed (Fig. 5). Physiotherapy was advised for metacarpophalangeal and IP joints. The patient had regained functional use of his thumb with significantly improved range of motion (ROM), stable grip, and adequate pinch strength by 18 weeks.

Figure 5: (a and b) Immediate post-operative X-rays, (c and d) follow-up X-rays at 12 weeks, (e and f) post-K-wire removal X-rays, (g-i) 18 weeks range of motion clinical pictures.
Postoperatively, histopathological examination revealed a well-circumscribed tumor comprising uniform stellate and spindle-shaped cells arranged in a lobular pattern in a fibromyxoid to chondromyxoid background. Individual tumor cells had moderate to abundant eosinophilic cytoplasm, having oval to spindle-shaped, large pleomorphic hyperchromatic nuclei with conspicuous nucleoli and occasional nuclear grooving seen. The lobules are surrounded by zones of hypercellularity in which they are mononuclear and are intermingled with multiple osteoclast-like giant cells arranged individually and in clusters, along with spindle-shaped cells. Small areas of cartilaginous matrix are also seen in the periphery of the lobules. The impression was CMF (Fig. 6).
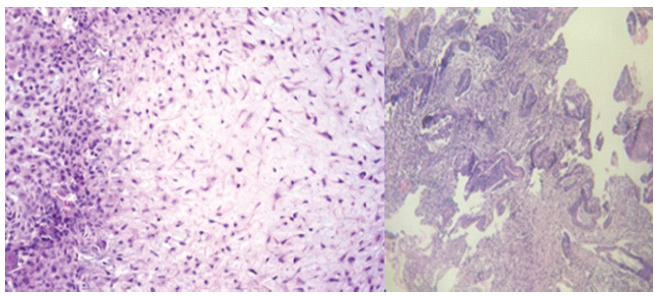
Figure 6: Histopathology slides confirming chondromyxoid fibroma.
This case highlights the efficacy of wide local excision of the tumor with ICBG and K-wire stabilization in managing rare CMFs of the thumb, demonstrating a successful return to function through tailored post-operative rehabilitation.
CMF is a rare benign cartilaginous tumor with an estimated incidence of <1% of all primary bone tumors [1]. Its typical presentation in long bones, such as the proximal tibia or femur, contrasts sharply with the rare occurrences in the bones of the hand. The present case of CMF involving the thumb metacarpal underscores the diagnostic and therapeutic challenges posed by this unusual tumor location, as well as the need for tailored surgical management to restore functional integrity. The primary treatment approach for CMF is complete resection, either through curettage or en bloc excision, to minimize the risk of local recurrence. The recurrence rate for CMF following curettage is estimated at 12.5–25%, highlighting the importance of complete resection, particularly in cases where local recurrence could significantly impact hand function. In this case, wide local excision of the tumor with preservation of endplates was preferred, as it minimizes the likelihood of residual tumor cells and recurrence. However, extensive resection in the thumb necessitates careful reconstruction to restore structural stability and function, a challenge effectively addressed using an ICBG combined with K-wire stabilization.
Functional outcome and scoring
To assess pre-operative and post-operative functional outcomes, standardized hand function scoring systems, such as the “Disabilities of the Arm, Shoulder, and Hand (DASH)” score and the “Michigan Hand Outcomes Questionnaire (MHQ),” were used [12]. Preoperatively, the patient reported moderate-to-severe functional limitations due to pain and restricted thumb movement, with higher DASH and lower MHQ scores indicating substantial impairment. Postoperatively, the patient demonstrated marked improvements in pain, thumb ROM, grip, and pinch strength, which were reflected in lower DASH and improved MHQ scores at the 12-week and 18-week follow-up (Table 1).
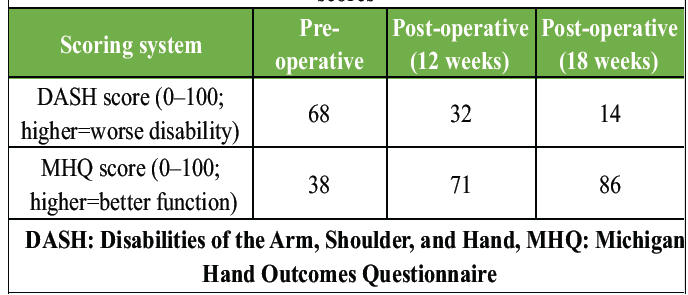
Table 1: Comparison of pre-operative and post-operative functional scores
Limitations and potential for recurrence
While wide local excision of the tumor with preservation of endplates with bone grafting achieved a satisfactory functional outcome, limitations remain. This approach requires donor site harvesting, which can lead to iliac crest morbidity, such as pain or discomfort. In addition, the structural integrity of the graft and fixation may necessitate further follow-up to monitor for complications, such as graft resorption or K-wire migration. Although recurrence rates are low with wide local excision, vigilance in monitoring for recurrence remains critical, especially in rare anatomical sites such as the thumb, where recurrence could impair hand function.
This case report demonstrates the successful management of CMF in the thumb metacarpal through wide local excision, tricortical ICBG, and K-wire stabilization. By employing a tailored surgical approach, we achieved favorable functional outcomes, with significant improvements in thumb ROM, grip, and pain reduction. Functional scoring outcomes confirmed the effectiveness of this approach in restoring hand function postoperatively. Long-term follow-up is essential to monitor for recurrence and maintain hand functionality, underscoring the importance of individualized surgical and rehabilitation strategies in rare bone tumor cases affecting critical structures such as the thumb.
CMF is an uncommon benign cartilaginous tumor that usually arises in the metaphyseal regions of long bones, with its occurrence in small bones being exceptionally rare. We report a rare case of CMF involving the first metacarpal, successfully managed with wide local excision and reconstruction using an autologous ICBG. A distinctive aspect of this management was the preservation of endplates during reconstruction, which provided mechanical stability while maintaining functional outcomes. This technique represents a novel and rarely reported approach.
References
- 1. Declerck GM, Rawlings ID, Hunt AC. Chondromyxoid fibroma in the metacarpal bone of the thumb. Acta Orthop Belg 1992;58:216-20. [Google Scholar] [PubMed]
- 2. Nkaoui M, Mahfoud M. Une localisation rare du fibrome chondromyxoïde: A propos d’un cas. Pan Afr Med J 2017;26:219. [Google Scholar] [PubMed]
- 3. Rouvillain JL, Jouannelle A, Delattre O, Pascal-Mousselard H, Catonne Y. Fibrome chondromyxoïde de l’astragale: À propos d’un cas et revue de la littérature. Rev Chir Orthop Reparat Appar Mot 1997;83:372-7. [Google Scholar] [PubMed]
- 4. Bründler E, Zanetti M, Boos N, Von Hochstetter AR. Chondromyxoid fibroma of two thoracic vertebrae. Skeletal Radiol 1999;28:286-9. [Google Scholar] [PubMed]
- 5. Daghfous M, Charfi H, Turki M, Maalla R, Baccari S, Tarhouni L. Le fibrome chondromyxoïde: À propos d’une localisation phalangienne du pouce. Chir Main 2007;26:159-64. [Google Scholar] [PubMed]
- 6. Chouchene MO, Amri R, Melek K, Ali SM. Chondromyxoid fibroma of the hand: A case report. Asian J Orthop Res 2020;3:107-11. [Google Scholar] [PubMed]
- 7. Feldman F, Hecht HL, Johnson AD. Chondromyxoid fibroma of bone. Radiology 1970;94:249-60. [Google Scholar] [PubMed]
- 8. Wu CT, Inwards CY, O’Laughlin S, Rock MG, Beabout JW, Unni KK. Chondromyxoid fibroma of bone: A clinicopathologic review of 278 cases. Hum Pathol 1998;29:438-46. [Google Scholar] [PubMed]
- 9. McMillan CR, Binhammer PA. Which outcome measure is the best? Evaluating responsiveness of the disabilities of the arm, shoulder, and hand questionnaire, the Michigan hand questionnaire and the patient-specific functional scale following hand and wrist surgery. Hand (N Y) 2009;4:311-8. [Google Scholar] [PubMed]
- 10. Bernd L, Ewerbeck V, Mau H, Cotta H. Characteristics of chondromyxoid fibroma: Are malignant courses possible? Presentation of personal cases and review of the literature. Unfallchirurg 1994;97:332-5. [Google Scholar] [PubMed]
- 11. WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours. 5th ed. Lyon: International Agency for Research on Cancer; 2020. [Google Scholar] [PubMed]
- 12. Anderson WJ, Bowers WH. Chondromyxoid fibroma of the proximal phalanx. A tumour that may be confused with chondrosarcoma. J Hand Surg Br 1986;11:144-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Acute Compound Irreducible Dorsal Dislocation of the Thumb IP Joint: A Case Report
May 1, 2026 Acute Compound Irreducible Dorsal Dislocation of the Thumb IP Joint: A Case Report January 1, 2026 Timely Intervention Saves the Limb in a 7-Year-old Child with Distal Femoral Physeal Injury: A Case Report
January 1, 2026 Timely Intervention Saves the Limb in a 7-Year-old Child with Distal Femoral Physeal Injury: A Case Report August 1, 2025 A Case Report of a Rare Entity – Lateral End of Clavicle Chondromyxoid Fibroma which was Mistaken as Giant Cell Tumor and Aneurysmal Cyst
August 1, 2025 A Case Report of a Rare Entity – Lateral End of Clavicle Chondromyxoid Fibroma which was Mistaken as Giant Cell Tumor and Aneurysmal Cyst June 1, 2025 Rare Case of Subscapularis Myositis Ossificans with Intra-articular Extension
June 1, 2025 Rare Case of Subscapularis Myositis Ossificans with Intra-articular Extension