
This case illustrates the diagnostic challenge of pediatric palmar masses, demonstrating that inconclusive imaging should not exclude Dupuytren’s disease from the differential diagnosis.
Jeanne Chartrin, Department of General Orthopaedic Surgery, Sainte Elisabeth Clinic, Namur, Belgium. E-mail: jeannechartrin@yahoo.fr
Abstract
Introduction: Dupuytren’s disease is a progressive fibroproliferative disorder primarily affecting men over 40. Its occurrence in children is extremely rare, with fewer than 25 cases reported since 1955. Due to its rarity, it is often overlooked in pediatric patients presenting with palmar masses. The etiology in children remains unclear, and clinical presentation may differ from the adult form, sometimes mimicking other fibromatoses or even malignancies.
Case Report: We report the case of a 12-year-old boy with a painful, progressively enlarging palmar mass. Examination revealed a firm subcutaneous nodule adherent to the palmar fascia, without digital contracture. Imaging suggested a tenosynovial cyst, but Dupuytren’s disease was also considered, leading to surgical excision of the palmar fascia. Histopathology confirmed Dupuytren’s disease, with fibroblastic proliferation and collagen deposition.
Conclusion: This case highlights the importance of considering Dupuytren’s disease in children presenting with palmar masses. Given its rarity, awareness is crucial to avoid misdiagnosis and unnecessary interventions. Long-term follow-up is recommended, given the uncertain recurrence risk in pediatric patients.
Keywords: Dupuytren’s disease, children, case report.
Dupuytren’s disease is a benign, progressive fibroproliferative disorder of the palmar fascia of the hand, leading to nodular thickening and contracture of the fingers. It is most commonly observed in adults over the age of 40 [1], with a higher prevalence in males. Adult cases frequently lead to progressive flexion contractures, requiring surgical or non-surgical management. Despite treatment, recurrence rates remain high, ranging from 12% to 73% [2], depending on the surgical technique.
In children, Dupuytren’s disease is extremely rare, with only a few cases reported [3]. While its clinical presentation can resemble the adult form, pediatric cases may also manifest differently [4,5], with isolated palmar nodules and an absence of digital contractures [1]. This variability in presentation can lead to diagnostic challenges and potential misdiagnosis [6]. Given the rarity of this condition in children, it is crucial to report new cases to improve awareness and facilitate early recognition.
A 12-year-old right-handed boy presented with a painful palmar mass on his left hand. The mass had been intermittently present for over a year, with recent enlargement and increased pain. There was no family history of Dupuytren’s disease, no prior trauma to the affected hand, and no other medical or surgical history.
Clinical examination revealed a firm, localized mass in the palm, initially suggestive of a para-tendinous cyst. X-ray of the left hand showed no bone lesions. An ultrasound examination was performed and revealed an oval hypoechoic lesion of 5 × 2 × 6 mm superficial to the flexor tendons of the fifth digit without vascularization on color Doppler. These findings were suggestive of a flexor tendon tenosynovial cyst; Dupuytren’s fibromatosis was also mentioned, but it considered unlikely given the patient’s young age.
Surgical procedure and post-operative course
Due to persistent pain and functional impairment, surgical excision was performed 1 month later, as the lesion was initially presumed to be a simple cyst.
The patient was positioned supine with a pneumatic tourniquet inflated to 250 mmHg for 17 min. A palmar incision was made over the nodule. Intraoperatively, the lesion exhibited characteristics consistent with Dupuytren’s fibromatosis rather than a simple cystic lesion. A limited fasciectomy of the affected palmar fascia was performed. Postoperatively, the hand was immobilized for 2 weeks to ensure proper healing.
At the 2-week follow-up, the wound was clean, and healing was progressing well. Local wound care was advised until complete healing. The patient exhibited full finger mobility without pain. A small area of hypoesthesia was noted at the commissure, likely due to transient nerve irritation, expected to resolve over time.
Histopathological analysis confirmed Dupuytren’s fibromatosis. The specimen consisted of nodular fragments measuring 5–7 mm. Histologically, it showed fibroblastic proliferation within dense collagen bundles without cytologic atypia or increased mitotic activity, consistent with palmar fibromatosis. The recurrence cannot be reliably estimated, but long-term surveillance is recommended. The patient and his father were informed of the possibility of future nodules, which could also involve the contralateral hand or the plantar fascia. Follow-up with ultrasound imaging was recommended.
Differential diagnosis
The differential diagnosis [6] for pediatric palmar masses includes giant cell tumor of tendon sheath, synovial cysts, extra-abdominal fibromatosis, infantile digital fibromatosis, and epithelioid sarcoma.
Diagnosis relies primarily on clinical presentation but is significantly helped by imaging techniques, particularly ultrasound and MRI. These modalities help characterize the lesion’s nature, extent, and relationship to surrounding structures, thereby supporting accurate diagnosis and guiding appropriate management [7].
Dupuytren’s disease is extremely rare in the pediatric population, with fewer than 25 cases reported since 1955 [8]. Given the rarity, it is often not considered in the differential diagnosis [9] of palmar nodule in children, where tumoral or post-traumatic etiologies are more frequently suspected [6,7,9].
Most reported pediatric cases describe male patients with progressive flexion deformity associated with palpable cords, mirroring the adult phenotype [3,5]. However, atypical presentations have been documented. Spyropoulou et al. reported a 10-year-old boy with a palmar nodule and finger retraction without clinically evident cords [10], while Soltani et al. described an isolated contracture in a post-traumatic context without palmar involvement [4]. Our case further expands this spectrum, as it is presented with a painful isolated nodule without contracture and misleading imaging findings.
Pain, which is uncommon in adult Dupuytren’s disease [2], should raise suspicion of alternative diagnoses. When pain is present, as in some atypical pediatric cases, it may contribute to diagnostic delay, and histopathological confirmation may be required.
A major limitation in the current literature is the lack of long-term follow-up, with most reports documenting <3 years of evolution. In adults, recurrence after surgical treatment is well documented and remains a significant concern [2]. Whether pediatric Dupuytren’s disease shares a similarly high recurrence potential is unknown. To date, only García-Mata and Duart-Clemente reported a 16-year follow-up without recurrence [11]. It remains unclear whether this favorable evolution represents an isolated outcome or suggests a distinct biological behavior in the pediatric population.
Given the limited number of cases and their clinical heterogeneity, systematic reporting and prolonged follow-up are essential to better define the natural history and recurrence risk of pediatric Dupuytren’s disease.
This case highlights the importance of considering Dupuytren’s disease in the differential diagnosis of pediatric palmar masses, as initial imaging may not always be conclusive. Early recognition and appropriate management are essential, especially given the uncertain long-term recurrence risk in pediatric patients.
Pediatric Dupuytren’s disease, although very rare, should be included in the differential diagnosis of a palmar mass, even in the absence of contracture. Atypical presentation and inconclusive imaging should not exclude the diagnosis.
References
- 1. Izadpanah A, Viezel-Mathieu A, Izadpanah A, Luc M. Dupuytren contracture in the pediatric population: A systematic review. Eur J Pediatr Surg 2013;25:151-4. [Google Scholar] [PubMed]
- 2. Sarkar M, Kashyap N, Madabhavi I. Dupuytren’s disease: A review. Chin J Plast Reconstr Surg 2024;6:142-8. [Google Scholar] [PubMed]
- 3. Urban M, Feldberg L, Janssen A, Elliot D. Dupuytren’s disease in children. J Hand Surg 1996;21:112-6. [Google Scholar] [PubMed]
- 4. Soltani A, Zargaran A, Kang N. Post-traumatic dupuytren’s contracture in a paediatric patient: A case report and literature review. Case Rep Plast Surg Hand Surg 2024;11:2436678. [Google Scholar] [PubMed]
- 5. Mandalia VI, Lowdon IM. Dupuytren’s disease in a child: A case report. J Pediatr Orthop B 2023;12:198-9. [Google Scholar] [PubMed]
- 6. Rhomberg M, Rainer C, Gardetto A, Piza-Katzer H. Dupuytren’s disease in children-differential diagnosis. J Pediatr Surg 2002;37:E7. [Google Scholar] [PubMed]
- 7. Zaidi Z, Villarreal Acha D, McCranie A, Kargel J. A review of soft tissue and nerve masses in the pediatric hand: Pathology, diagnosis, and management strategies. Cureus 2025;14:e85999. [Google Scholar] [PubMed]
- 8. Beecher SM, Jeantet Q, Cronin KJ. Paediatric dupuytren’s disease in a child of indian ethnicity: A case report and literature review. Cureus 2021;13:e20434. [Google Scholar] [PubMed]
- 9. Korambayil PM, Padikala A. Paediatric dupuytren’s disease. Indian J Plast Surg 2011;44:521-4. [Google Scholar] [PubMed]
- 10. Spyropoulou GA, Pavlidis L, Milothridis P, Zaraboukas T, Demiri E. Dupuytren in a Child: Rare Presentation of a Rare Clinical Entity. J Hand Surg 2016;41:e477-9. [Google Scholar] [PubMed]
- 11. García-Mata S, Duart-Clemente J. Dupuytren’s disease in a child: A long-term evolution after surgery. J Pediatr Orthop B 2019;28:85-8. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2024 Brodie’s Abscess of the Humeral Paddle in a Child: A case Report
October 1, 2024 Brodie’s Abscess of the Humeral Paddle in a Child: A case Report August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report
August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report August 1, 2026 To Explore or Not? Conservatively Managed Brachial Artery Injury with Good Collateral Flow After Elbow Reduction: A Case Report
August 1, 2026 To Explore or Not? Conservatively Managed Brachial Artery Injury with Good Collateral Flow After Elbow Reduction: A Case Report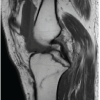 August 1, 2026 An Unusual Catastrophic Neurological Complication Following a Routine Arthroscopic Multiligament Knee Reconstruction: A Case Report
August 1, 2026 An Unusual Catastrophic Neurological Complication Following a Routine Arthroscopic Multiligament Knee Reconstruction: A Case Report