
In cases of hip pain associated with high-energy trauma, clinicians should include traumatic iliacus hematoma in the differential diagnosis alongside fractures.
Hiroki Kobayashi, Department of Orthopedic Surgery, National Defense Medical College, Tokorozawa, Saitama 359-8543, Japan. E-mail: supercova0205@gmail.com
Abstract
Introduction: We report a case of femoral nerve paralysis associated with a traumatic iliacus hematoma.
Case Report: A 19-year-old female presented with left groin pain. She fell from a height of 3 m during cheerleading and experienced numbness in the left femoral nerve region along with quadriceps muscle weakness. Radiographs found no sign of fractures; however, magnetic resonance imaging revealed a left iliacus hematoma extending to the lacuna muculorum, adjacent to the femoral nerve. Based on these findings, the diagnosis of traumatic iliacus hematoma accompanied by femoral nerve paralysis was made. Since the hematoma was relatively small, she was conservatively treated. Her symptoms fully resolved by 60 days post-injury.
Conclusion: While femoral nerve paralysis associated with iliacus hematoma is rare and difficult to diagnose correctly, this condition should be included in the differential diagnosis when encountering a patient with groin pain after high-energy trauma.
Keywords: Femoral nerve paralysis, traumatic iliacus hematoma, high‑energy trauma
Iliopsoas hematoma refers to a hematoma within the psoas or iliacus muscles [1]. This condition is often associated with femoral nerve paralysis and often seen in patients receiving anticoagulant therapy (1.3–6.6%) and in patients with hemophilia (5.5–10.4%) [2-4].
In contrast, traumatic iliopsoas hematoma with femoral nerve paralysis is relatively rare. The femoral nerve is located between the psoas major and iliacus muscles and passes beneath the iliac fascia. When a hematoma develops in either of these muscles due to trauma, it is believed that the nerve can become compressed between the relatively unyielding iliac fascia and the muscle, resulting in paralysis; however, this remains a hypothesis due to the limited number of reported cases. Regarding treatment, conservative management is generally chosen in the early stages or in cases of incomplete paralysis, while surgical evacuation of the hematoma is often selected for complete paralysis. With appropriate treatment, the prognosis is generally considered to be favorable [2].
Here, we present a case of traumatic iliacus hematoma with femoral nerve paralysis, accompanied by a review of the literature.
A 19-year-old female presented with pain in her left groin and anterior thigh. Her past medical and family histories were unremarkable. She fell from a height of 3 m during cheerleading, landing forcefully on her buttocks. Due to severe pain, she presented to the emergency department of our hospital. On admission, she was alert with stable vital signs. She complained of left groin pain and numbness in the anterior thigh. The left hip was slightly flexed due to pain exacerbated by extension (Fig. 1).
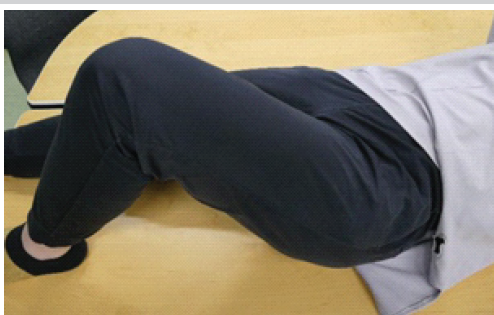
Figure 1: Appearance of the left lower limb at presentation. Due to pain, the hip joint was mildly flexed, and extension was impossible.
The range of motion of the hip joint was as follows: flexion, 30°; extension, −20°; abduction, 30°; adduction, 10°; external rotation, 20°; and internal rotation, 15°. Due to pain, the straight-leg raise test and manual muscle testing (MMT) of the left iliopsoas muscle could not be performed. MMT of the quadriceps muscle was rated 4 on a 0-5 scale, and all other muscles were rated 5. The Japanese Orthopaedic Association (JOA) hip score, which reflects hip joint function, was as low as 9 points. The patellar tendon reflex was positive on the right, and the left was absent. There was no pain or tenderness in the lower back.
Based on the left groin pain and flexed left hip posture, iliopsoas muscle injury was suspected. The pain, numbness, and hypoesthesia in the anterior thigh, along with quadriceps weakness, suggested femoral nerve paralysis. Furthermore, the high-energy trauma and severe pain upon movement indicated possible femoral fractures and hip dislocation. However, no significant abnormalities were found on radiographs (Fig. 2).
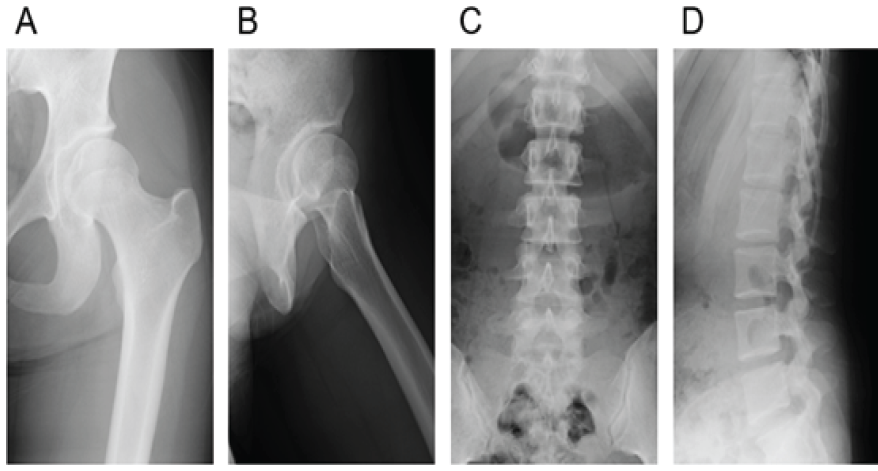
Figure 2: Plain radiographs of the right hip joint and lumbar spine showing no obvious findings, including fracture and dislocation ([a and b] anteroposterior and lateral views of the hip joint; [c and d] anteroposterior and lateral views of the spine).
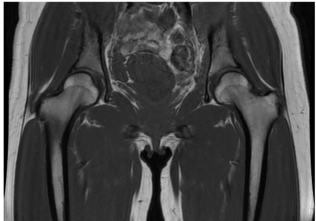
Figure 3: Coronal section of the pelvis on T1-weighted magnetic resonance imaging showing no abnormalities suggestive of occult fracture in the proximal femur.
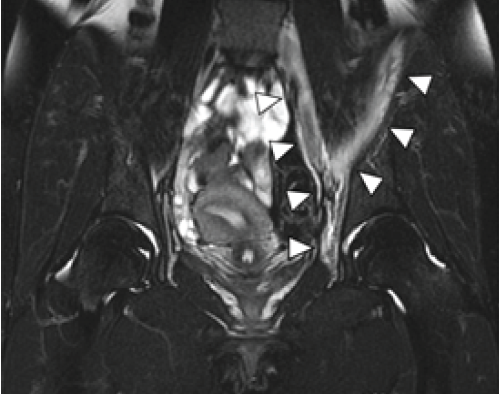
Figure 4: Coronal section of the pelvis on short tau inversion recovery magnetic resonance imaging showing an extensive detachment of the iliacus muscle and a hematoma surrounding the iliacus and iliopsoas muscles and extending into the retroperitoneal space (white arrowheads).
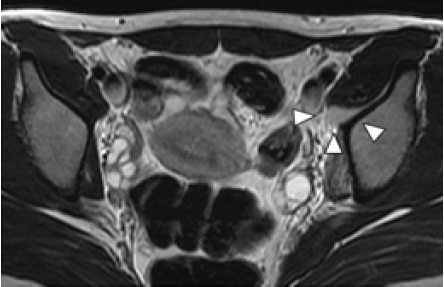
Figure 5: Axial slice of the pelvis on T2-weighted magnetic resonance imaging at the level of the lacuna musculorum. A hematoma has formed around the iliacus muscle (white arrowheads).
These findings led to the final diagnosis of traumatic iliacus hematoma with femoral nerve paralysis. Considering the relatively small size of the hematoma and the mild nerve paralysis, conservative treatment was chosen. Since the patient had difficulty walking due to muscle weakness and pain, she was hospitalized for rest. For the first 2o days after the injury, the patient was confined to bed rest due to severe pain and difficulty in movement. Within a few days, she gradually became able to sit upright. From day 7 post-injury, no restrictions were placed on weight-bearing, and gait training with the assistance of crutches was initiated. Active range-of-motion exercises were not performed. By the 11th day of hospitalization, pain and numbness in the thigh had reduced, and the muscle strength of the iliopsoas and quadriceps recovered to 4 on MMT, allowing discharge. Follow-up was continued on an outpatient basis, and by 60 days post-injury, the symptoms had completely resolved. At this point, the JOA score was 100 points. No recurrence of symptoms has been observed since.
Traumatic iliopsoas hematoma refers to a hematoma caused by trauma in the psoas or iliacus muscles, more frequently found in young males. It is often associated with sports-related injuries and has been reported to cause femoral nerve or obturator nerve impairment [5]. However, such condition has only been reported in 39 cases (with outcomes documented in 36 cases), indicating it is likely an extremely rare disorder [6,7]. These patients were approximately 70% males with an average age of 17.6 years. About 40% of the patients exhibited complete paralysis and often underwent decompression surgery, while patients with incomplete paralysis were most often managed conservatively. At the final follow-up, approximately 20% of patients had residual paralysis. In the present case, the patient was a 19-year-old female with incomplete femoral nerve paralysis, and conservative management was undertaken. Her femoral nerve paralysis fully resolved during the course of treatment, indicating that our diagnosis and choice of treatment were appropriate.
Traumatic iliopsoas hematoma is thought to be caused by the strong contraction of the iliacus muscle caused by sudden hip hyperextension or falls [8]. In our case, the patient sustained falling from a height of 3 m during cheerleading. Cheerleading involves postures with intense hyperextension of the hip in mid-air, which can potentially overstretch the iliacus muscle between the iliac bone and femur. Furthermore, the fall from a substantial height may have triggered a strong protective muscle contraction of the iliacus muscle.
Regarding the cause of femoral nerve paralysis, a past study suggests that, due to the relatively thin fascia, iliacus muscle often increases in volume as a hematoma forms, leading to compression of the femoral nerve that runs over this muscle [9]. Another study suggests that it most often occurs when a hematoma forms at the lacuna musculorum, where the femoral nerve is most susceptible to compression [10]. In our patient, the volume of the hematoma was not particularly substantial; however, it extended to the lacuna musculorum, as observed on MRI (Fig. 3). This suggests that the extent of the hematoma, in addition to the volume, is associated with femoral nerve paralysis.
We presented a case of femoral nerve paralysis associated with a traumatic iliacus hematoma. Since this condition is rare and can be challenging to diagnose correctly, patients are often misdiagnosed with different musculoskeletal or neurological conditions that can cause similar symptoms. When groin or anterior thigh pain occurs following high-energy trauma, this condition should be included in the differential diagnosis.
In cases of hip pain associated with high-energy trauma, clinicians should include traumatic iliacus hematoma in the differential diagnosis alongside fractures.
References
- 1. [1] Otsubo S, Mizumoto J. Idiopathic iliopsoas muscle hematoma. JMA J 2024;7:288-9. [Google Scholar] [PubMed]
- 2. [2] Nefiss M, Tebourbi A, Ben Maatoug A, Bouzidi R. Femoral nerve paralysis complicating a post-traumatic iliopsoas haematoma. BMJ Case Rep 2018;2018:bcr2017220446. [Google Scholar] [PubMed]
- 3. [3] Kong WK, Cho KT, Lee HJ, Choi JS. Femoral neuropathy due to iliacus muscle hematoma in a patient on warfarin therapy. J Korean Neurosurg Soc 2012;51:51-3. [Google Scholar] [PubMed]
- 4. [4] Gertzbein SD, Evans DC. Femoral nerve neuropathy complicating iliopsoas haemorrhage in patients without haemophilia. J Bone Joint Surg Br 1972;54:149-51. [Google Scholar] [PubMed]
- 5. [5] Oueslati MW, Kamoun K, Arfa W, Jenzri M, Chaabouni M, Riahi H. Traumatic iliac muscle hematoma: A rare etiology of quadriceps palsy (case report). Int J Surg Case Rep 2024;115:109124. [Google Scholar] [PubMed]
- 6. [6] Lefevre N, Bohu Y, Klouche S, Chemla N, Herman S. Complete paralysis of the quadriceps secondary to post-traumatic iliopsoas hematoma: A systematic review. Eur J Orthop Surg Traumatol 2015;25:39-43. [Google Scholar] [PubMed]
- 7. [7] Sallahi H, Margad O, Lamkhantar A, Idrissi KK. Posttraumatic hematoma of the iliopsoas muscle with femoral nerve palsy: a case report and review of the literature. Pan Afr Med J. 2015;20:198. [Google Scholar] [PubMed]
- 8. [8] Magana-Reyes J, Dominguez-Gasca LG, Garcia-Luna A, Dominguez-Carrillo LG. Iliacus muscle injury caused by inadequate exercise. Acta Ortop Mex. 2016;30(3):154–157. [Google Scholar] [PubMed]
- 9. [9] Kopell HP, Thompson WA. Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60. [Google Scholar] [PubMed]
- 10. [10] Nobel W, Marks SC Jr., Kubik S. The anatomical basis for femoral nerve palsy following iliacus hematoma. J Neurosurg 1980;52:533-40. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Traumaplasty in Action: Staggered Bilateral Primary Total Knee Arthroplasty for Complex Proximal Tibial Fractures with Osteoarthritis – A Case Report
December 1, 2025 Traumaplasty in Action: Staggered Bilateral Primary Total Knee Arthroplasty for Complex Proximal Tibial Fractures with Osteoarthritis – A Case Report April 1, 2025 A Rare Footprint: A Case Report of Isolated Pre-Axial Fully Developed Supernumerary Toe
April 1, 2025 A Rare Footprint: A Case Report of Isolated Pre-Axial Fully Developed Supernumerary Toe November 10, 2022 Bilateral Dega and Varus Derotational Osteotomies for Painful Hip Subluxation in Acute Flaccid Myelitis: A Case Report
November 10, 2022 Bilateral Dega and Varus Derotational Osteotomies for Painful Hip Subluxation in Acute Flaccid Myelitis: A Case Report April 7, 2014 Reviewers Acknowledgement & Photogallery April-June 2014
April 7, 2014 Reviewers Acknowledgement & Photogallery April-June 2014