
In this series of seven skeletally immature children, rigid intramedullary nailing of tibial shaft fractures via the suprapatellar approach was not associated with limb deformity or growth arrest.
Ms. Mckenzie D Brandt, University of Central Florida College of Medicine, 6850 Lake Nona Blvd, Orlando - 32827, Florida, United States. E-mail: mc417656@ucf.edu
Abstract
Introduction: Tibial shaft fractures are common pediatric injuries. Rigid intramedullary nails (RIMN) are widely used for the fixation of complex tibial shaft fractures in skeletally mature individuals, but their safety is debated in patients with open physes. There has been growing support for the use of RIMN fixation in pediatric patients due to the stability and rapid return to weight-bearing activities they offer. In this study, we evaluate the utility and safety of suprapatellar RIMN fixation in skeletally immature children with tibial shaft fractures.
Materials and Methods: This retrospective case series includes seven skeletally immature patients treated with suprapatellar RIMN fixation of tibial shaft fractures at a single level one trauma center between May 1, 2009, and May 1, 2024. The primary outcome of interest was clinical signs of iatrogenic growth arrest. Secondary outcomes of interest included post-operative complications and time to full weight bearing (FWB), union, and sport.
Results: The mean age at the time of operation was 13.7 years (range: 12–15) and the mean follow-up time was 14.21 months (range: 6–26.5). We observed no clinical evidence of iatrogenic growth arrest or limb deformity post-operatively. The mean time to union was 24.17 weeks. On average, patients returned to FWB and full activity/sport at 10.33 and 22.67 weeks, respectively. The majority of patients (n = 5) did not require hardware removal with the exception of one patient who developed a deep tissue infection and another with delayed union of an associated fibula fracture.
Conclusion: In a series of seven skeletally immature children, suprapatellar RIMN fixation of tibial shaft fractures was not associated with iatrogenic growth arrest. Benefits of this fixation technique include an expedited return to weight-bearing activity and sport.
Keywords: Intramedullary fixation, skeletally immature, tibial shaft fracture, orthopedic trauma, suprapatellar approach.
Tibial shaft fractures are a common cause of orthopedic inpatient admission to pediatric hospitals in the US [1]. Tibial torsion, sports injuries, and motor vehicle accidents are frequently cited as mechanisms of diaphyseal injury [2,3], and recovery time varies greatly depending on fracture pattern and treatment approach. While the mainstay of tibial shaft fractures in pediatric patients is closed reduction and casting (CRC) – particularly in children <10 years of age – patients with more complex fracture patterns may require surgical fixation [4].
When operative management is required, intramedullary nailing is an effective and minimally invasive strategy. In adults, fixation with a rigid intramedullary nail (RIMN) expedites healing and return to weight-bearing activities, with reduced time to union and lower risk of malunion compared to CRC [5,6]. However, the use of these implants in skeletally immature patients is debated due to concern that their insertion through an open proximal tibial physis may arrest growth. Elastic stable intramedullary nails (ESIN) – inserted distal to the proximal tibial physis – are generally considered a safer alternative in skeletally immature children but are less stable than RIMN [7]. They additionally require post-operative immobilization and a second operation for implant removal after fracture union [8], delaying return to weight-bearing activities and sport.
In recent years, there has been increasing support for the use of RIMN fixation in pediatric tibial shaft fractures, though literature on this topic is sparse. The suprapatellar approach has been widely adopted and reported to allow for better fracture alignment and easier reduction than the infrapatellar approach [9,10]. In this study, we present post-operative outcomes of seven skeletally immature patients who underwent RIMN fixation of tibial shaft fractures via the suprapatellar approach. Our objective is to contribute to the growing literature on the utility and safety of RIMN fixation in skeletally immature tibial shaft fractures, with a particular focus on the suprapatellar approach.
This retrospective study included seven skeletally immature patients treated with suprapatellar RIMN fixation of tibial shaft fractures at a single level one trauma center between May 1, 2009, and May 1, 2024. The criteria for inclusion in the study were (1) patients aged between 11 and 17 years who (2) underwent suprapatellar RIMN fixation of a tibial shaft fracture and (3) had open proximal tibial physes at the time of fixation as determined by pre-operative radiographs. Skeletal maturity status was classified by proximal tibial ossification status at the time of pre-operative imaging studies. Patients with pathologic fractures, congenital or developmental bone or connective tissue diseases, or <6 months of documented follow-up were excluded.
Operative technique
The procedures were performed by pediatric fellowship-trained orthopedic surgeons. Fractures were fixed with Advanced Orthopaedic Solutions (AOS) (n = 1), Stryker T2 (n = 2), or Smith and Nephew TRIGEN (n = 4) nail systems with diameters ranging from 8.5 to 10 cm. Implant type and diameter were determined by the admitting orthopedic surgeon.
The patient was positioned supine on a radiolucent table with the knee placed in a semi-extended position (15–30° of flexion) to facilitate access to the suprapatellar entry point. Under fluoroscopic guidance, a longitudinal incision was made proximal to the patella, and the quadriceps tendon was split longitudinally to allow insertion of a protective cannula system. After confirming the correct starting point under fluoroscopy, a guidewire was introduced through the cannula and advanced under fluoroscopy into the tibial canal. Sequential reaming was performed over the guidewire, followed by insertion of an appropriately sized intramedullary nail. Proximal and distal interlocking screws were placed under fluoroscopic guidance. Care was taken throughout the procedure to minimize intra-articular damage by maintaining appropriate alignment of the instrumentation and protecting the patellofemoral joint.
Informed consent was obtained after the risks and benefits of the procedure were described. For open fractures (n = 3), irrigation and debridement was performed in addition to fixation, and the appropriate prophylactic antibiotic regimen was started (Fig. 1).
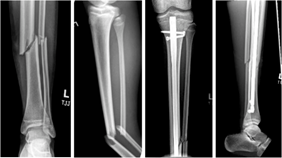
Figure 1: Rigid intramedullary nails fixation of a skeletally immature tibial/fibula fracture. Shown are anterior/posterior and lateral X-rays taken before (left) and immediately after fixation (right) of a left simple oblique midshaft tibia fracture in a skeletally immature patient. An 8.5 × 360 mm Smith and Nephew TRIGEN tibial nail was used in this patient.
Rehabilitation and follow-up protocol
All patients were designated as weight bearing as tolerated (WBAT) post-operatively. Most patients were followed up initially at 4–6 weeks post-operatively and subsequently at 3-month intervals until return to baseline activity was achieved. During each follow-up visit, all patients underwent radiological and clinical assessments. Pre- and post-operative radiographs were used to determine time to union, and successful union was defined as <5° of angulation, and significant leg length discrepancy was defined as >10 mm difference.
The mean age of our study population was 13.7 years. Five patients were male, and two patients were female. Three patients self-identified as non-Hispanic white (42.9%), one as Hispanic white (14.3%), and three patients as Black or African American (42.9%). The majority of injuries were high-energy trauma (n = 5). The most common mechanisms of injury were auto v. pedestrian incidents (n = 4) and sports injuries (n = 2), with one all-terrain vehicle (ATV) rollover accident. All patients were taken to the operating room in <24 h, with the exception of one patient who was admitted on an outpatient basis after a failed attempt at conservative treatment with CRC (Table 1).
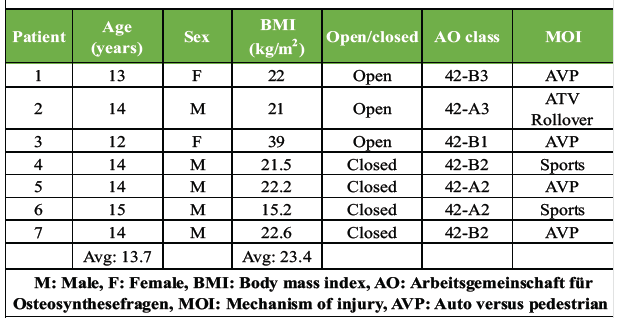
Table 1: Patient and fracture characteristics
The mean post-operative length of stay was 2.43 days (range: 1–4) and all patients were WBAT at the time of discharge. Patients were followed for an average of 14.21 months (range: 6–26.5). The mean time to union was 24.17 weeks (range: 14–31). Patients achieved full weight bearing (FWB) status at 10.33 weeks (range: 6–20) and were able to return to full activity or sport at 22.67 weeks (range: 16–28), on average. All fractures united successfully, with the exception of one patient who ultimately required hardware removal and resection of the affected bone due to osteomyelitis. This patient was excluded from the calculation of mean time to union, time to FWB, or time to return to full activity/sport (Table 2).
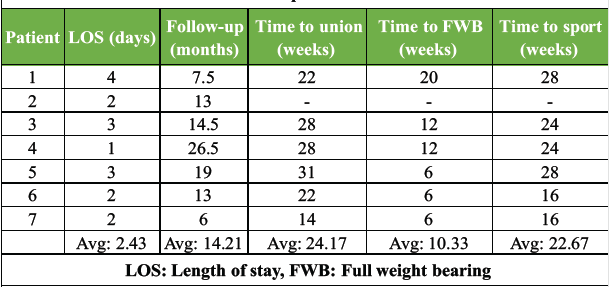
Table 2: Post-operative outcomes
The primary complication of interest was evidence of growth arrest or tibial shortening, and there was no evidence of tibial shortening or partial growth arrest of the proximal tibial physis in any of the included patients. Two patients required hardware removal: One for mobilization of a delayed fibular union, and another for treatment of osteomyelitis, as mentioned previously. No patients required hardware removal due to painful or prominent hardware (Table 3).
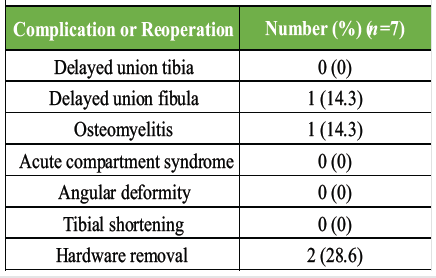
Table 3: Post-operative complications and reoperation
In this study, we describe the use of suprapatellar RIMN in seven skeletally immature tibial shaft fractures. Our study population had excellent post-operative outcomes, with no evidence of tibial non-union or malunion, tibial shortening, angular deformity, or iatrogenic growth arrest. Patients returned to FWB in as little as 6 weeks and to full activity or sport in as little as 4 months. Two patients developed complications unrelated to growth arrest or deformity. One patient had delayed union of an associated fibular fracture, though this resolved after hardware removal and ultimately united. Although one patient developed osteomyelitis post-operatively, this was likely related to the mechanism of injury and open fracture type rather than the use of an intramedullary nail.
Our findings are consistent with previous studies, which reported no signs of physeal injury or growth arrest in skeletally immature tibial shaft fractures fixed with RIMN [11,12,13,14]. Two prior studies have reported results of pediatric RIMN fixation using the infrapatellar approach [11,12], and one study presented a series of 37 skeletally immature tibial shaft fractures fixed via RIMN, though >80% were infrapatellar [13]. A fourth study, recently published in the Journal of the Pediatric Orthopedic Society of North America, observed no significant clinical or radiographic evidence of growth disturbance in a cohort of 35 skeletally immature children treated with suprapatellar tibial RIMN [14]. Participants were surveyed at their final follow-up appointment, and an overall patient satisfaction rating of 9.56/10 was reported by 30 respondents [14].
An advantage of RIMN fixation of tibial shaft fractures is the expedited return to weight-bearing activity, which is associated with improved outcomes and faster healing [15]. All of our patients were able to WBAT at the time of discharge, whereas patients treated with ESIN or CRC are non-weight bearing or partial weight bearing post-operatively [3,16]. CRC in particular requires a significant period of immobilization – often 10–12 weeks – delaying return to weight-bearing activity [7]. Return to sport can also be delayed with these techniques. Patients treated with CRC may require significant rehabilitation to combat muscle atrophy, while patients allowed to weight bear early can maintain muscle bulk during healing. In addition, the standard procedure for ESIN is to remove the hardware after healing [8], requiring a second operation and rehabilitation period. Alternatively, rigid nails can be left in place indefinitely. In this study, there were no patients who required hardware removal for painful or prominent hardware.
Additional studies are needed to determine whether the suprapatellar or infrapatellar approach is superior in skeletally immature children. However, the suprapatellar approach is generally preferred in adults due to superior functional outcomes. Patients who underwent suprapatellar RIMN are less likely to experience persistent anterior knee pain and more likely to be satisfied with their post-operative activity level [17,18,19]. Intraoperatively, the suprapatellar approach also allows for easier fracture reduction, greater accuracy with nail insertion, and shorter operating time with reduced radiation exposure [20,21,22].
The primary limitation of this study is its small sample size, which limits statistical power and the ability to detect rare complications. The retrospective design introduces potential selection and documentation bias, and the absence of a control group prevents direct comparison with alternative techniques, such as ESIN, CRC, or infrapatellar RIMN fixation. Follow-up was relatively short and variable, which may be insufficient to detect late growth disturbances. The cohort consisted primarily of patients near skeletal maturity, limiting generalizability to younger children with significant growth remaining. Functional outcomes were limited to clinical milestones without validated patient-reported outcome measures or quality-of-life assessments, and the exclusion of one patient with post-operative osteomyelitis from certain outcome analyses may introduce reporting bias. Physeal injury was assessed clinically and radiographically with plain films, potentially missing subtle injuries detectable on advanced imaging. Finally, implant selection was not standardized, introducing technical heterogeneity.
Stable reduction and early mobilization are critical in the management of pediatric tibial shaft fractures with complex fracture patterns. While CRC delays return to weight-bearing activity and ESIN lacks stability, RIMN achieves both goals. In seven skeletally immature tibial shaft fractures fixed with RIMN via the suprapatellar approach, there were no signs of iatrogenic growth arrest or limb deformity. Therefore, we conclude that suprapatellar RIMN is a viable option for fixation of skeletally immature tibial shaft fractures, despite its insertion through the proximal tibial physis. Our study contributes to the limited but growing literature on the use of RIMN fixation of tibial shaft fractures in skeletally immature children and includes a patient population with the youngest reported mean age to date.
While many pediatric tibial shaft fractures can be adequately treated with CRC, RIMN fixation is an excellent and safe option for more complicated fracture types, or perhaps for those who wish to make a quick return to sport. Most patients recovered uneventfully, and there was no evidence of limb deformity or iatrogenic growth arrest.
References
- 1. Galano GJ, Vitale MA, Kessler MW, Hyman JE, Vitale MG. The most frequent traumatic orthopaedic injuries from a national pediatric inpatient population. J Pediatr Orthop 2005;25:39-44. [Google Scholar] [PubMed]
- 2. Hogue GD, Wilkins KE, Kim IS. Management of pediatric tibial shaft fractures. J Am Acad Orthop Surg 2019;27:769-78. [Google Scholar] [PubMed]
- 3. Patel NK, Horstman J, Kuester V, Sambandam S, Mounasamy V. Pediatric tibial shaft fractures. Indian J Orthop 2018;52:522-28. [Google Scholar] [PubMed]
- 4. Kinney MC, Nagle D, Bastrom T, Linn MS, Schwartz AK, Pennock AT. Operative versus conservative management of displaced tibial shaft fracture in adolescents. J Pediatr Orthop 2016;36:661-6. [Google Scholar] [PubMed]
- 5. Bone LB, Sucato D, Stegemann PM, Rohrbacher BJ. Displaced isolated fractures of the tibial shaft treated with either a cast or intramedullary nailing. An outcome analysis of matched pairs of patients. J Bone Joint Surg Am 1997;79:1336-41. [Google Scholar] [PubMed]
- 6. Obremskey WT, Cutrera N, Kidd CM, Southeastern Fracture Consortium. A prospective multi-center study of intramedullary nailing vs casting of stable tibial shaft fractures. J Orthop Traumatol 2017;18:69-76. [Google Scholar] [PubMed]
- 7. Weltsch D, Baldwin KD. Rigid locked nail fixation for pediatric tibia fractures – where are the data? World J Orthop 2019;10:299-303. [Google Scholar] [PubMed]
- 8. Egger A, Murphy J, Johnson M, Hosseinzadeh P, Louer C. Elastic stable intramedullary nailing of pediatric tibial fractures. JBJS Essent Surg Tech 2020;10:e19.00063. [Google Scholar] [PubMed]
- 9. Courtney PM, Boniello A, Donegan D, Ahn J, Mehta S. Functional knee outcomes in infrapatellar and suprapatellar tibial nailing: Does approach matter? Am J Orthop (Belle Mead NJ) 2015;44:E513-6. [Google Scholar] [PubMed]
- 10. Chan DS, Serrano-Riera R, Griffing R, Steverson B, Infante A, Watson D, et al. Suprapatellar versus infrapatellar tibial nail insertion: A prospective randomized control pilot study. J Orthop Trauma 2016;30:130-4. [Google Scholar] [PubMed]
- 11. Widbom-Kolhanen S, Helenius I. Intramedullary nailing of paediatric tibial fractures: Comparison between flexible and rigid nails. Scand J Surg 2021;110:265-70. [Google Scholar] [PubMed]
- 12. Court-Brown CM, Byrnes T, McLaughlin G. Intramedullary nailing of tibial diaphyseal fractures in adolescents with open physes. Injury 2003;34:781-5. [Google Scholar] [PubMed]
- 13. Koshinski JL, Bram JT, Gross PW, Hine SH, Hayes DS, Fabricant PD, et al. Exploring outcomes of tibial rigid intramedullary nailing in adolescent patients. J Orthop Trauma 2025;39:186-91. [Google Scholar] [PubMed]
- 14. Pargas-Colina CD, Coble TJ, Davis SE, Spence DD, Rowland JK, Kelly DM, et al. Outcomes of suprapatellar intramedullary nail fixation of tibial shaft fractures in skeletally immature patients. J Pediatr Soc North Am 2025;12:100200. [Google Scholar] [PubMed]
- 15. Jenkins MD, Jones DL, Billings AA, Ackerman ES, France JC, Jones ET. Early weight bearing after complete tibial shaft fractures in children. J Pediatr Orthop B 2009;18:341-6. [Google Scholar] [PubMed]
- 16. Griffet J, Leroux J, Boudjouraf N, Abou-Daher A, El Hayek T. Elastic stable intramedullary nailing of tibial shaft fractures in children. J Child Orthop 2011;5:297-304. [Google Scholar] [PubMed]
- 17. Sepehri A, You D, Lobo AA, Schneider P, Lefaivre KA, Guy P. Comparison of patient-reported outcomes after suprapatellar versus infrapatellar nailing techniques for tibial shaft fractures: A systematic review and meta-analysis. J Orthop Trauma 2022;36:e208-14. [Google Scholar] [PubMed]
- 18. Sanders RW, DiPasquale TG, Jordan CJ, Arrington JA, Sagi HC. Semiextended intramedullary nailing of the tibia using a suprapatellar approach: Radiographic results and clinical outcomes at a minimum of 12 months follow-up. J Orthop Trauma 2014;28 Suppl 8:S29-39. [Google Scholar] [PubMed]
- 19. Yang CY, Tay ST, Kuo LT. Suprapatellar vs infrapatellar approaches for intramedullary nailing of distal tibial fractures: A systematic review and meta-analysis. J Orthop Traumatol 2023;24:14. [Google Scholar] [PubMed]
- 20. Al-Azzawi M, Davenport D, Shah Z, Khakha R, Afsharpad A. Suprapatellar versus infrapatellar nailing for tibial shaft fractures: A comparison of surgical and clinical outcomes between two approaches. J Clin Orthop Trauma 2021;17:1-4. [Google Scholar] [PubMed]
- 21. Anderson TR, Beak PA, Trompeter AJ. Intra-medullary nail insertion accuracy: A comparison of the infra-patellar and supra-patellar approach. Injury 2019;50:484-88. [Google Scholar] [PubMed]
- 22. Williamson M, Iliopoulos E, Williams R, Trompeter A. Intra-operative fluoroscopy time and radiation dose during suprapatellar tibial nailing versus infrapatellar tibial nailing. Injury 2018;49:1891-94. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study
March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study July 1, 2026 Masquelet Technique Combined with Non-vascularized Fibular Strut Graft for Reconstruction of a Large Tibial Bone Defect in a Skeletally Immature Patient: A Case Report
July 1, 2026 Masquelet Technique Combined with Non-vascularized Fibular Strut Graft for Reconstruction of a Large Tibial Bone Defect in a Skeletally Immature Patient: A Case Report June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies
June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies May 1, 2026 Effect of Intrawound Vancomycin Powder as an Adjunct to SystemicAntibiotic Prophylaxis on Surgical Site Infection Following Open TibialFracture Fixation: A Randomized Prospective Study
May 1, 2026 Effect of Intrawound Vancomycin Powder as an Adjunct to SystemicAntibiotic Prophylaxis on Surgical Site Infection Following Open TibialFracture Fixation: A Randomized Prospective Study