
Chronic patellar tendon ruptures, though rare and technically challenging, can be effectively managed using an ipsilateral semitendinosus autograft with transosseous figure-of-eight fixation and suture augmentation, restoring excellent knee function with minimal morbidity
Dr. Sumit Raghute, Department of Orthopaedics, All India Institute of Medical Sciences, Nagpur - 441108, Maharashtra, India. E-mail: sumitr67@gmail.com
Abstract
Introduction: Patellar tendon rupture is an uncommon but disabling injury, often resulting from eccentric quadriceps contraction or trauma. Chronic ruptures (>3 weeks) present a reconstructive challenge due to patellar migration, scarring, and tendon retraction, making primary repair inadequate. Various graft options exist; autologous semitendinosus provides a strong, biologically compatible solution with minimal morbidity.
Case Report: A 42-year-old man presented 8 weeks post-injury with left knee instability and inability to extend the leg following a fall. Examination revealed patella alta and an extensor lag. Radiographs and magnetic resonance imaging confirmed chronic patellar tendon rupture with retraction and fibrosis. Surgical reconstruction was performed using an ipsilateral semitendinosus autograft. After adhesiolysis and distal mobilization of the patella, transosseous tunnels were created in the patella and proximal tibia. The semitendinosus graft was passed in a figure-of-eight fashion to recreate the patellar tendon and secured with Suture Tape augmentation. The knee was immobilized in extension initially, with early passive motion and progressive flexion from week 3 onward. Active mobilization and strengthening were started after 6 weeks, and the brace was discontinued by 10–12 weeks. At 6 months, the patient achieved full active extension, 0–120° knee motion, 5/5 quadriceps strength, normal patellar height, and a pain-free gait without lag or instability.
Conclusion: Chronic patellar tendon ruptures can be successfully reconstructed using a semitendinosus autograft with transosseous fixation and suture augmentation. This technique restores extensor mechanism continuity and yields excellent functional recovery when combined with meticulous soft-tissue release and structured rehabilitation.
Keywords: Patellar tendon rupture, semitendinosus autograft, chronic knee injury, tendon reconstruction, patella alta.
Patellar tendon ruptures are rare, with an incidence of approximately 0.68/100,000 person-years. They typically occur in active males in their third or fourth decade of life following eccentric quadriceps contraction or direct trauma [1]. Disruption of the extensor mechanism renders the knee non-functional, and early repair is recommended. Chronic ruptures (>2–3 weeks after injury) are technically demanding due to proximal patellar migration, scarring, and tendon retraction. Primary repair alone is rarely feasible, and reconstruction with graft augmentation is usually required [2].
Autologous hamstring grafts (semitendinosus ± gracilis) are widely used for patellar tendon reconstruction, offering strong biologic tissue with minimal donor morbidity [2]. Allografts, such as the Achilles tendon, have also been reported, but they carry risks of immune reaction and disease transmission [3]. Semitendinosus autograft with preserved tibial insertion has been shown to restore function effectively, even in neglected injuries [4].
We present a case of chronic patellar tendon avulsion in a 42-year-old man successfully managed with semitendinosus autograft reconstruction.
A 42-year-old male presented with a 2-month history of left knee instability and inability to actively extend his knee. The injury occurred when he fell from approximately 6 feet in height, landing awkwardly on his left leg. He recalled a sudden pop sound in the knee and immediate collapse. Initial evaluation at a local clinic noted a lateral patellar dislocation, which was manually reduced. The patient was treated with a knee immobilizer. He presented to our institution 8 weeks later due to persistent disability.
On examination, there was moderate knee swelling and a palpable defect in the area of the patellar tendon just below the patella. The patella was positioned high (suggestive of patella alta). The patient was unable to perform a straight-leg raise, and an extensor lag of about 20° was noted in supine testing. Tenderness was present along the patellar tendon region. The knee was otherwise stable to varus/valgus and anteroposterior testing, and there were no neurovascular deficits.
Plain radiographs of the knee showed a high-riding patella with an Insall-Salvati ratio >1.2 and a small bony fragment at the mid-substance region of the patellar tendon, consistent with a possible avulsion from the inferior pole of the patella (Fig. 1).

Figure 1: Pre-operative X-ray showing a high-riding patella with an insallsalvati ratio >1.2 and a small bony fragment at the mid-substance region of
the tendon.
Magnetic resonance imaging (MRI) revealed disruption of the patellar tendon. Laxity with avulsion of the attachment of the patellar tendon with resultant retraction was noted, with an intra-substance high signal intensity of the patellar tendon. The patella was markedly elevated. The MRI also showed low-grade injury to the quadriceps tendon with high T2 signal intensity and wavy fibers (Fig. 2). These findings confirmed a chronic patellar tendon rupture with scarring, in the setting of a traumatic patellar dislocation.
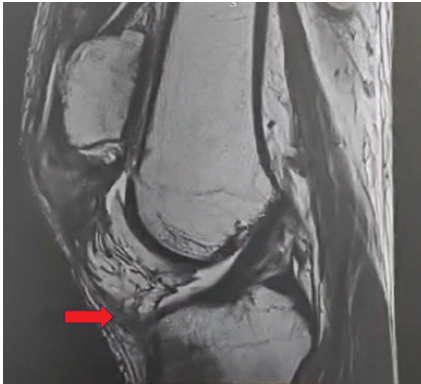
Figure 2: Magnetic resonance imaging showing avulsion of the attachment of the patellar tendon.
Given the chronic nature of the injury and poor quality of the residual tendon, we planned a patellar tendon reconstruction using an autologous hamstring tendon graft.
Under spinal anesthesia and with the patient supine, an examination under anesthesia confirmed the presence of a palpable gap between the patella and the tibial tuberosity. Under a tourniquet, a 15 cm midline incision was taken from the patellar center to the level of the tibial tuberosity. Dissection was carried down through scar tissue to expose the extensor mechanism. Dense adhesions were found around the patella and patellar tendon area. Fibrotic tissue was carefully debrided, and the patella was mobilized: Adhesions in the suprapatellar pouch and patellar retinacula were released to allow the patella to be pulled distally toward its anatomic position (Fig. 3).
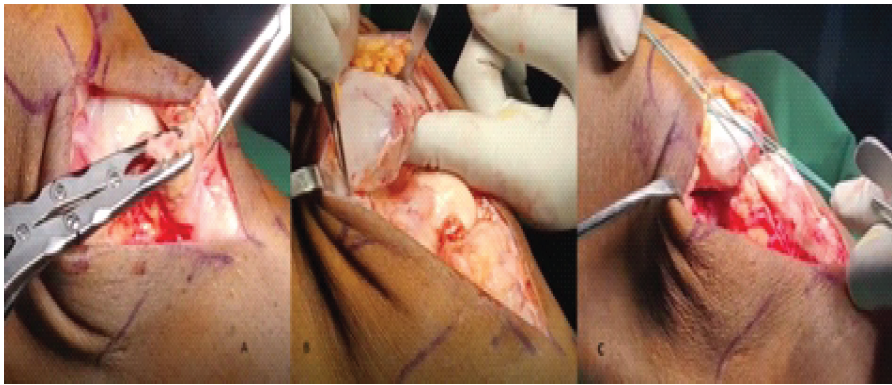
Figure 3: (a) Adhesions and fibrotic tissues were cleared; (b) Patella was mobilised; (c) Ends of the patella approximated.
The ruptured patellar tendon stump was identified at the inferior patellar pole. This stump was freshened, and pair of No. 2 Ethibond sutures were placed transversely through the substance of the remaining patellar tendon. A similar No. 2 Ethibond suture was taken transosseously through the proximal patella, and it was used to pull the patella downward toward the remnant (Fig. 4).
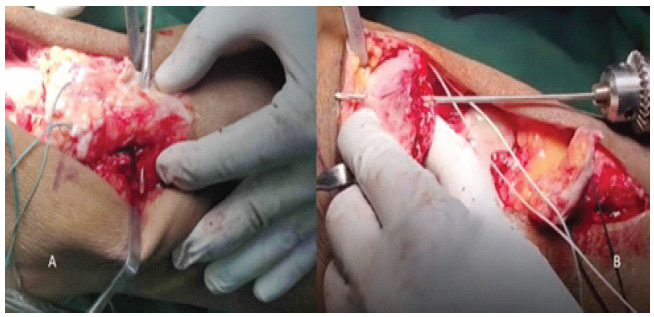
Figure 4: (a) Preparation of trans osseous tunnels; (b) Preparation of vertical trans osseous tunnels through the patella for passage of suture ends.
The ipsilateral semitendinosus tendon was identified through a small incision over the pes anserinus. Using a tendon stripper, the semitendinosus was harvested. The tendon was freed from muscular tissue, and its ends were whip-stitched with a No. 2 Fibre wire. The gracilis tendon was left intact.
Transosseous tunnels were then created to secure the graft. Under fluoroscopic guidance, a guide pin was drilled transversely through the patella at the mid-level of the patella (center of the patellar body). This was over-reamed to a 4.5 mm diameter tunnel. Similarly, a 4.5 mm transverse tunnel was created in the proximal tibia at the level of the tibial tubercle (just below the original patellar tendon insertion) (Fig. 5).
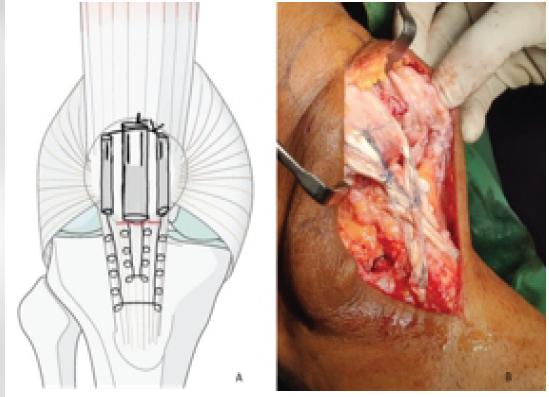
Figure 5: (a) Suture ends passed through the tunnels and tied as described; (b) Fixation biologically augmented with SemiT graft in figure of eight fashion.
Using a No. 2 Suture Tape, a Krackow stitch was taken in the distal patellar tendon, on the medial side with two free ends. Another No. 2 Suture Tape was used to take a Krackow stitch through the lateral side of the patellar tendon. Three transosseous tunnels were drilled vertically in the proximal patella (Fig. 6).

Figure 6: (a and b) 6 months clinical follow-up; (c) 6 months post-operative X-ray.
The first free end of the Suture Tape was passed through the first tunnel, and the second and third free ends were passed through the second tunnel. The fourth free end was passed through the third tunnel. The knee was brought into full extension, and the patella was positioned at the correct height (we verified patellar height by ensuring the patella’s lower pole aligned with Blumensaat’s line and approximating a normal Insall-Salvati ratio). The first and second free ends were tied with each other. Similarly, the third and fourth free ends were tied with each other at the end of the tunnel.
This fixation was then augmented with the biological autograft. The semitendinosus graft was then passed in a figure-of-eight fashion through the transverse tunnels to reconstruct the patellar tendon. Specifically, the graft was first passed through the patellar tunnel from lateral to medial, then laid along the course of the original patellar tendon (over the anterior knee), and then from lateral to medial through the tibial tunnel. By this routing, the semitendinosus effectively formed a new tendinous connection from the tibial tubercle to the patella, spanning and reinforcing the area of the native tendon.
With the graft in place, the semitendinosus graft was then secured. The free end of the graft was tied on itself with adequate tension to achieve apposition of the proximal and distal poles of the patella.
The patient underwent a structured rehabilitation program. The knee was immobilized in full extension post-operatively, with gentle continuous passive motion and supervised physiotherapy initiated on day 1 to control pain, swelling, and maintain muscle tone. For the first 2 weeks, only isometric quadriceps and hamstring exercises were done with the brace locked; partial weight-bearing progressed to full by 2 weeks in extension.
From week 3, passive flexion began (0–30°), increasing by 15°/week to reach 90° by 6 weeks; active extension was avoided. After 6 weeks, active and assisted range of motion (ROM) exercises started, brace flexion was gradually unlocked, and closed-chain and light quadriceps strengthening commenced. The brace was discontinued by 10–12 weeks.
Between 3 and 6 months, therapy emphasized full ROM and progressive strengthening. By 3 months, the patient achieved 0–90° motion, walked brace-free, and showed no graft elongation or patellar alta recurrence.
At the 6-month follow-up, the patient demonstrated substantial improvement and a successful outcome. His surgical incision was well-healed with no signs of infection or wound complications. The patella was maintained in a normal position, and there was no palpable gap in the tendon. He achieved full active knee extension (0°) with no extensor lag, indicating robust restoration of the extensor mechanism. Active knee flexion was up to 90°, with passive flexion up to 120°. The patient’s quadriceps strength was graded 5/5 on manual testing, symmetric to the opposite side, and he could perform a straight-leg raise without difficulty. He walked with a normal gait, was able to ascend and descend stairs reciprocally, and reported no giving-way or instability in the knee.
The patient had returned to his pre-injury level of activity in terms of work and basic recreation. He was pain-free in the knee and did not require any supportive devices for ambulation. Follow-up radiographs showed a normal patellar height (Insall-Salvati ratio restored to ~1.0) and no heterotopic ossification or hardware complications.
Delayed presentation of a patellar tendon rupture significant treatment challenge. In chronic cases, the patella tends to migrate proximally (patella alta) due to the unopposed pull of the quadriceps, and surrounding tissues contract and scar in this malposition [1]. The longer the delay, the more difficult it becomes to mobilize the patella back to its anatomic position. Furthermore, the ruptured tendon ends are typically retracted and atrophied, making primary end-to-end repair under tension either impossible or prone to failure. Approximately 27% of extensor mechanism injuries are chronic; highlighting that missed initial diagnosis is not uncommon [2]. Our case underscores these issues: By 2 months post-injury, the patellar tendon in our patient had insufficient length and quality for direct repair, necessitating a reconstructive approach.
Key principles in management include: (1) Adequate mobilization of the patella/quadriceps mechanism, (2) use of a tendon graft or augmentation to bridge the defect, and (3) protection of the repair with some form of auxiliary support to allow early rehabilitation [2,4,5]. Mobilizing a chronically high-riding patella is often the toughest intraoperative step. Intraoperatively, extensive quadriceps adhesiolysis is performed; one may need to release the tight quadriceps tendon or even perform a quadriceps tendon lengthening (e.g., V-Y turndown) if the patella cannot be brought to the level of the tibial tubercle without excessive tension [1]. Fortunately, in our patient, standard adhesions release allowed anatomic reduction of the patella. We did, however, take care to flex the knee repeatedly after reconstruction to ensure the patella was not overly constrained by residual scar.
For reconstruction of the tendon itself, a variety of graft choices exist. We selected an autogenous semitendinosus tendon graft. Using the patient’s own tissue avoids the immune response and potential disease transmission of allografts. Hamstring autografts are readily available and have high tensile strength relative to the forces on the knee extensor mechanism [2,5]. Semitendinosus-gracilis autograft harvest is associated with minimal long-term donor deficit [2]. An isolated semitendinosus autograft (distal attachment preserved) to reconstruct a chronic patellar tendon tear, allows early motion with a stable repair [5].
Alternative autografts and allografts are worth considering. Contralateral bone–patellar tendon–bone (BTB) grafts have been used in chronic cases, effectively transplanting a patella-tendon-tibial tubercle unit from the opposite knee. This can anatomically restore the extensor mechanism and patellar height automatically [1]. However, BTB autografts carry significant donor site morbidity (including risking the extensor mechanism of the normal knee) and are typically reserved for cases with large defects or failed prior reconstructions. Achilles tendon allografts are another popular option, especially when the defect is substantial or in the context of multiple ligament injuries or arthroplasty [3]. Allograft use spares the patient a donor-site harvest and provides a large, strong graft. The downside is that processed allografts may be weaker due to sterilization methods and carry a small risk of disease transmission [6]. Husen et al. recently reported a case of bilateral patellar tendon reconstructions with Achilles allograft after failed repairs, with good 3-year results [3]. Synthetic grafts or meshes (such as the ligament augmentation reconstruction system) have also been used in extensor mechanism reconstructions with mixed success [7].
Within hamstring techniques, there are nuances regarding graft attachment. One major decision is whether to preserve the hamstring’s tibial insertion. Cadambi and Engh preserved the distal attachment of the semitendinosus in their technique; they routed the graft through a patellar tunnel and then sutured the free end back to the tibia periosteum, thus avoiding a tibial tunnel [8]. The supposed benefit of preserving the native insertion is that it maintains the graft’s blood supply and possibly its proprioceptive innervation, which could enhance incorporation. Vukman et al. have noted that using a single tendon can be sufficient in neglected patellar tendon repairs [4].
There are methods that aim to shield the reconstructed tendon from excessive forces during the early healing phase, permitting safe mobilization. A traditional method is metal wire circlage or a frame (e.g., the McLaughlin frame) between the patella and tibia [4]. While effective in protecting the repair, wires require a second surgery for removal and carry risks, such as wire breakage or infection. In our practice, we prefer modern augmentations that avoid permanent metal. We utilized a as an internal brace in this case. This tape spans the repair and takes load off the graft during knee flexion, yet it is made of a braided ultrahigh-molecular-weight polyethylene that can remain indefinitely or be removed later if desired. Nguene-Nyemb et al. employed a different approach for augmentation: They folded the quadriceps expansion (tendon) down over the repair and sutured it (a sort of V–Y turndown flap). This biologic augmentation provided additional strength and permitted up to 90° of flexion intraoperatively without undue tension on the repair [5]. Augmentation, whether synthetic or autologous, is strongly recommended by many authors for chronic cases to reduce the risk of failure during rehabilitation.
Our patient’s successful recovery highlights that even delayed patellar tendon injuries can achieve good outcomes with appropriate management. By 6 months, he had full extension, functional flexion, and return to daily activities pain-free. This mirrors outcomes from other reports. Most literature emphasizes that a diligent, graduated rehabilitation is as important as the surgical technique in achieving a good result. If the knee is immobilized too long, arthrofibrosis and muscle atrophy can occur; if mobilized too aggressively, the repair can stretch out or rupture. Typically immobilizing in extension for 4–6 weeks, but allowing controlled passive motion in that period is critical [9].
Potential complications in chronic patellar tendon repair include wound healing problems, infection, re-rupture of the graft, slackening of the graft leading to recurrent patella alta, and fractures of the patella or tibial tubercle through drill holes. Patella fractures have been reported when transverse patellar tunnels are used (especially if the patella is small or osteopenic) [10].
Chronic patellar tendon avulsion injuries, though rare, can be effectively managed with meticulous surgical reconstruction and rehabilitation. This case illustrates that using an ipsilateral semitendinosus autograft to reconstruct a 2-month-old patellar tendon rupture resulted in an excellent functional outcome. Key elements of success included restoring patellar position, utilizing a strong autograft, augmenting the repair to allow early motion, and adhering to a gradual rehabilitation protocol. The patient regained full knee extension, meaningful flexion, and returned to pre-injury activities without extensor lag or pain. This outcome aligns with published experiences and supports the semitendinosus autograft as a versatile and safe option for chronic extensor mechanism ruptures. We recommend this technique for similar cases, with the disclaimer that each case requires individualized planning.
Even in delayed presentations of patellar tendon rupture, meticulous patellar mobilization and biological reconstruction with a semitendinosus autograft can successfully restore extensor mechanis
This technique provides a simple, reproducible, and cost-effective option yielding excellent functional recovery when combined with structured rehabilitation.
m continuity.
References
- 1. Tandogan RN, Terzi E, Gomez-Barrena E, Violante B, Kayaalp A. Extensor mechanism ruptures. EFORT Open Rev 2022;7:384-95. [Google Scholar] [PubMed]
- 2. Harris JD, Fazalare JJ, Phieffer LS, Flanigan DC. Patellar tendon reconstruction with semitendinosus-gracilis autograft. J Knee Surg 2013;26 Suppl 1:S19-24. [Google Scholar] [PubMed]
- 3. Husen M, Krych AJ, Poudel K, Stuart MJ. Patellar Tendon Reconstruction After Failed Primary Repair of Bilateral Ruptures: A Case Report. JBJS Case Connect. 2024 Jan 19;14(1). doi: 10.2106/JBJS.CC.23.00493. PMID: 38241429. [Google Scholar] [PubMed] [CrossRef]
- 4. Vukman P, Kadija M, Sreckovic S, Bilanovic M, Milovanovic D. Neglected patellar tendon rupture treated with a single semitendinosus tendon in one-stage reconstruction surgery: A case report of an unusual injury mechanism. Cureus 2025;17:e80699. [Google Scholar] [PubMed]
- 5. Nguene-Nyemb AG, Huten D, Ropars M. Chronic patellar tendon rupture reconstruction with a semitendinosus autograft. Orthop Traumatol Surg Res 2011;97:447-50. [Google Scholar] [PubMed]
- 6. Liu Q, Tang D, Zhu W, Chen Y. Patellar tendon reconstruction using autologous hamstring tendons for the treatment of extensive patellar tendon ossification. Orthop Surg 2022;14:3119-24. [Google Scholar] [PubMed]
- 7. Talia AJ, Tran P. Bilateral patellar tendon reconstruction using LARS ligaments: Case report and review of the literature. BMC Musculoskelet Disord 2016;17:302. [Google Scholar] [PubMed]
- 8. Cadambi A, Engh GA. Use of a semitendinosus tendon autogenous graft for rupture of the patellar ligament after total knee arthroplasty. A report of seven cases. J Bone Joint Surg Am 1992;74:974-9. [Google Scholar] [PubMed]
- 9. Akpinar B, Baron S, Alaia MJ, Jazrawi LM. Clinical and biomechanical outcomes following knee extensor mechanism reconstruction. Arthrosc Sports Med Rehabil 2020;2:e553-61. [Google Scholar] [PubMed]
- 10. Ciriello V, Gudipati S, Tosounidis T, Soucacos PN, Giannoudis PV. Clinical outcomes after repair of quadriceps tendon rupture: A systematic review. Injury 2012;43:1931-8. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Neglected but Negotiated – A Case Report of Multiple Zone VII Extensor Tendon Injuries Reconstructed Using Fascia Lata Autograft
June 1, 2026 Neglected but Negotiated – A Case Report of Multiple Zone VII Extensor Tendon Injuries Reconstructed Using Fascia Lata Autograft February 1, 2026 Gore-Tex Membrane Augmentation for Treatment of Acute Patellar Tendon Rupture in a Soccer Player – A Case Report
February 1, 2026 Gore-Tex Membrane Augmentation for Treatment of Acute Patellar Tendon Rupture in a Soccer Player – A Case Report July 1, 2025 Open Repair of a Thrice Ruptured Twice Repaired Traumatic Patellar Tendon
July 1, 2025 Open Repair of a Thrice Ruptured Twice Repaired Traumatic Patellar Tendon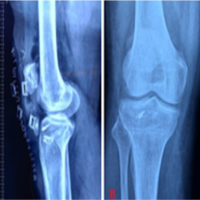 November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report
November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report