
In children with acute osteomyelitis, clinicians should maintain a high index of suspicion for concurrent deep vein thrombosis, as timely evaluation and imaging are crucial to prevent missed diagnoses and serious complications.
Dr. Shrihari L Kulkarni, Department of Orthopaedics, SDM College of Medical Sciences and Hospital, Shri Dharmasthala Manjunatheshwara University, Dharwad, Karnataka, India. E-mail: shrihari1711@gmail.com
Abstract
Introduction: Acute osteomyelitis (AOM) is a common pediatric infection; however, its association with deep vein thrombosis (DVT) is rare and often underdiagnosed due to overlapping symptoms.
Case Report: We report three pediatric cases (mean age 9.3 years) of femoral AOM complicated by DVT, all due to methicillin-resistant Staphylococcus aureus (MRSA). Fever, limb pain, and swelling were the presenting triad in all patients. Magnetic resonance imaging confirmed osteomyelitis with abscess, and Doppler ultrasound or computed tomography venogram detected DVT. Management included surgical drainage with cortical decompression and anticoagulation therapy. All patients achieved complete recovery within 10–12 months.
Conclusion: Severe femoral osteomyelitis, particularly when MRSA-positive, should prompt clinicians to consider concurrent DVT. Early combined imaging and intervention can prevent serious complications and ensure optimal functional outcomes.
Keywords: Acute osteomyelitis, deep vein thrombosis, methicillin-resistant Staphylococcus aureus.
Acute osteomyelitis (AOM) is one of the most frequent serious musculoskeletal infections in children, most often resulting from hematogenous spread from a distant infectious focus, with direct inoculation following trauma or surgery being a less common cause [1,2]. In contrast, deep vein thrombosis (DVT) is rare in the pediatric population, with an estimated incidence below 0.01% in otherwise healthy children [3,4]. This low frequency is partly attributed to developmental differences in coagulation physiology, including reduced thrombin generation and increased fibrinolytic activity compared with adults [5,6].
Despite this, the risk of DVT increases markedly in hospitalized children up to 58/10,000 admissions, especially in the presence of recognized risk factors such as central venous catheterization, trauma, hypercoagulable states, prolonged immobility, or chronic inflammatory diseases [5,6]. In recent years, DVT in children has been increasingly associated with severe musculoskeletal infections caused by community-acquired methicillin-resistant Staphylococcus aureus (MRSA), a pathogen with potent virulence factors capable of promoting thrombosis [7].
The co-occurrence of AOM and DVT remains uncommon, but it is clinically important due to the potential for severe complications such as septic pulmonary embolism (SPE). Previous reports suggest that antecedent limb trauma may predispose to osteomyelitis and subsequent thrombophlebitis, with Staphylococcus aureus being the predominant causative organism [8,9]. However, overlapping features, such as fever, swelling, erythema, and pain, often delay the diagnosis of DVT in patients already suspected or diagnosed with AOM [9,10]. Given these challenges, early recognition using combined imaging modalities, including Doppler ultrasonography and magnetic resonance imaging (MRI), is essential to guide prompt, targeted therapy and reduce morbidity.
Case 1
A 3-year-old boy presented to the emergency department with a 3-day history of fever, pain in the left proximal thigh, and inability to bear weight on the affected limb. The symptoms began after a trivial fall while playing, following which he remained ambulatory for approximately 36 h before developing progressive swelling of the left lower limb. Initial evaluation by a local practitioner, including plain radiography, revealed no bony injury; the child was discharged with oral analgesics and antibiotics. However, symptoms persisted, prompting presentation to our center.
On arrival, the patient was febrile with high-grade temperature. Examination revealed diffuse swelling of the left thigh with localized warmth, tenderness, and pain on passive stretch. No neurovascular deficits were noted. Radiographs again showed no fracture but demonstrated increased soft-tissue haziness in the proximal femur region. Laboratory tests revealed anemia, leukocytosis, and markedly elevated C-reactive protein (CRP) (>300 mg/L).
A computed tomography (CT) venogram identified thrombus within the left external iliac, common femoral, and proximal superficial femoral veins, as well as an adjacent intramuscular collection communicating with a deep femoral venous branch. The patient was commenced on low molecular weight heparin (LMWH) and empirical intravenous antibiotics. Despite therapy, his clinical condition deteriorated.
Subsequent MRI of the thigh demonstrated features consistent with AOM of the proximal femur and an associated intramuscular abscess. Surgical intervention was performed, consisting of drainage of the intramuscular collection and decompression of the proximal femur through multiple cortical drill holes. Intraoperative cultures yielded MRSA, and antibiotic therapy was adjusted accordingly (Fig. 1).
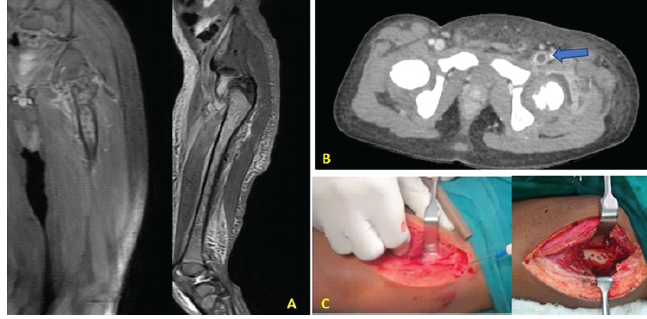
Figure 1: (a) Magnetic resonance imaging showing signs of acute osteomyelitis, (b) computed tomography venogram showing thrombus in the femoral vein, (c) intraoperative images of abscess drainage and cortical drilling.
Postoperatively, LMWH was transitioned to oral anticoagulation with warfarin (2.2 mg once daily) for 3 months, with international normalized ratio monitoring. The patient showed rapid symptomatic improvement, was discharged after 2 weeks of intravenous antibiotics, and completed an additional 2 weeks of oral therapy. At 10-month follow-up, he had regained full limb function without recurrence of infection or thrombotic events.
Case 2
A 15-year-old girl presented to the outpatient department with breathlessness and swelling of the right lower limb. Chest evaluation revealed bilateral basal pneumonia on CT scan. Examination of the right lower limb showed diffuse swelling from the knee to the proximal thigh, with localized warmth, erythema, marked tenderness, and severe pain on passive movement of the knee.
Laboratory tests demonstrated severe anemia and poorly controlled type 1 diabetes mellitus (hemoglobin A1c: 11.9%). Duplex Doppler ultrasound (USG) of the limb identified DVT involving the popliteal and superficial femoral veins, and anticoagulation with rivaroxaban was initiated.
Given the severity of symptoms, an MRI of the thigh was performed, which revealed a large subperiosteal abscess on the posterior aspect of the distal femur (15 × 5 cm), an additional collection anteriorly, and marrow changes consistent with AOM of the mid- to distal femur. The patient underwent incision and drainage of the abscess with cortical decompression of the distal femur (Fig. 2).
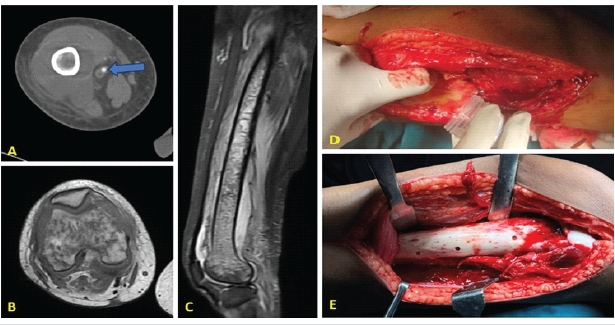
Figure 2: (a) Computed tomography venogram showing femoral vein thrombus, (b and c) magnetic resonance imaging showing subperiosteal abscess and destruction of the distal femur, (d) intraoperative picture of abscess drainage, (e) cortical drilling of the distal femur for decompression.
Intraoperative pus cultures grew MRSA, and antibiotic therapy was adjusted based on sensitivity. Postoperatively, the patient experienced rapid clinical improvement and was discharged after 2 weeks of intravenous antibiotics, continuing oral therapy thereafter. Anticoagulation was maintained with apixaban (10 mg twice daily) for 5 months. At 12-month follow-up, both infection and thrombosis had completely resolved, and full limb function was restored.
Case 3
An 11-year-old boy presented to the emergency department with a 5-day history of swelling and pain in the left lower limb, accompanied by fever and inability to bear weight. The symptoms followed a history of trauma to the left thigh. Initial symptomatic management by a local practitioner failed to yield improvement.
On examination, the patient was febrile with diffuse swelling of the left thigh, localized warmth, erythema, and tenderness. Hip and knee movements were painful, and pain on passive stretch was present. Laboratory investigations showed leukocytosis (total leukocyte count: 23,380 cells/mm3; neutrophils: 80.2%), elevated erythrocyte sedimentation rate, and markedly raised CRP. Doppler USG revealed DVT of the popliteal and superficial femoral veins. MRI confirmed osteomyelitis of the femur with a subperiosteal abscess along the posteromedial aspect, extending from the midshaft to the distal metaphysis (Fig. 3).
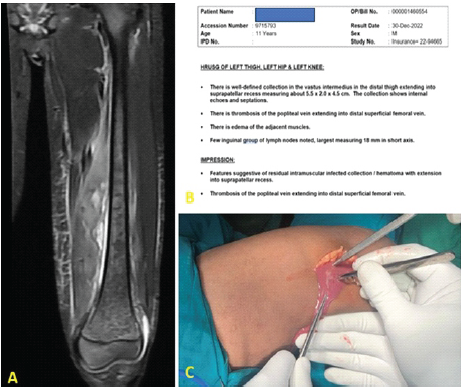
Figure 3:(a) Magnetic resonance imaging showing features of acute osteomyelitis of the femur at the junction of the middle and distal one-third, (b) ultrasound report of the patient, (c) abscess drainage from the thigh.
Surgical drainage of the abscess and cortical decompression of the distal femur were performed. On post-operative day 4, recurrence of swelling prompted re-exploration, which revealed re-accumulation of pus. Repeat cultures grew MRSA, and targeted antibiotics were commenced.
Anticoagulation was initiated with LMWH (30 mg twice daily), and later transitioned to warfarin (1.25 mg once daily) for 3 months. The patient improved steadily and, at 12-month follow-up, demonstrated full recovery without recurrence of infection or thrombotic events (Table 1).
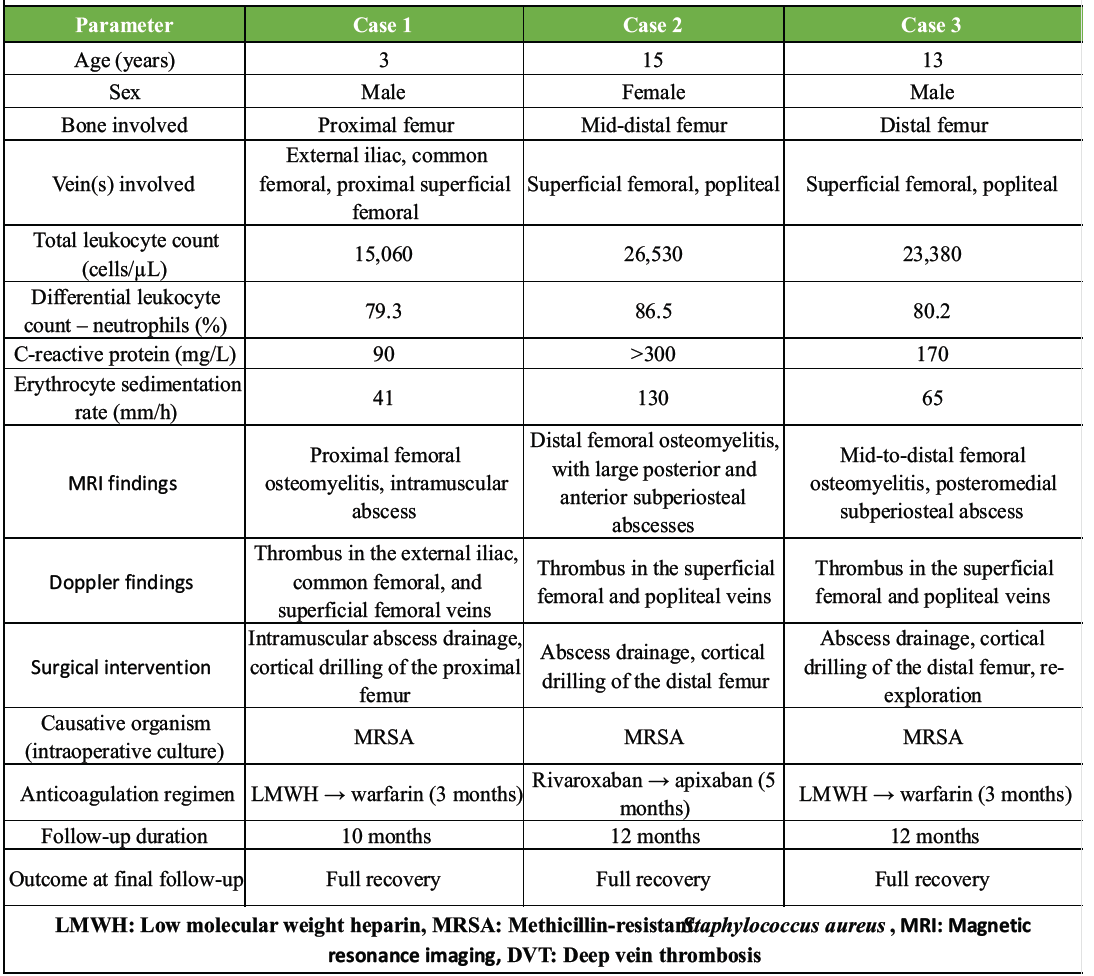
Table 1: Summary of demographic, clinical, laboratory, and treatment details of three pediatric cases of femoral osteomyelitis with DVT
No standardized institutional protocol for DVT screening was used during the study period. Imaging modalities (Doppler USG, CT venogram, or MRI) were selected at the discretion of the treating clinician based on clinical presentation. Routine thrombophilia workup was not performed in any of the three cases.
Acute hematogenous osteomyelitis (AHO) is relatively common in children, whereas its association with DVT remains infrequently reported and poses a diagnostic challenge due to significant symptom overlap between the two conditions [11,12].
During childhood, the metaphysis of long bones has a rich vascular supply, predisposing it to hematogenous bacterial seeding. Minor limb trauma can further increase susceptibility to infection in the setting of bacteremia, particularly when caused by highly virulent organisms such as MRSA or Klebsiella pneumoniae.
If not recognized and treated promptly, the infection may extend beyond the bone to involve the draining venous system, leading to septic thrombophlebitis and DVT. Several clinical and laboratory parameters have been identified as risk factors for thrombosis in pediatric musculoskeletal infection, including intensive care unit admission, sepsis, elevated D-dimer, persistent high-grade fever, and MRSA infection. MRSA has been identified as an independent risk factor for DVT in children with osteomyelitis [13,14].
Two distinct age peaks have been described for pediatric venous thrombosis: Neonates/infants and preadolescents/adolescents. Contributing factors include central venous catheterization (especially in infants), congenital or acquired prothrombotic states, trauma, prolonged immobilization, surgery, and pregnancy in adolescent girls [15].
Over the past decade, reports of DVT in association with AHO have increased. Hollmig et al. identified DVT in 11 of 212 pediatric AHO cases and conducted the only comparative study between AHO patients with and without DVT [16]. Gonzalez et al. reported nine pediatric cases of DVT associated with staphylococcal osteomyelitis, with most involving MRSA [17]. In both studies, thrombus location was most often adjacent to the infected bone, consistent with our series in which all DVTs occurred in the pelvis or lower limb veins adjacent to the femur.
Pathophysiology
The intense inflammatory response of AHO, particularly in MRSA infections, may directly contribute to thrombus formation. S. aureus produces a range of virulence factors that interact with coagulation pathways, including enzymes that promote fibrin deposition and bacterial exotoxins that induce platelet aggregation and vascular smooth muscle spasm [18]. Panton–Valentine leukocidin, a cytotoxin produced by many MRSA and methicillin-susceptible Staphylococcus aureus strains, has been implicated in severe necrotizing infections with high rates of associated thrombosis [19].
Diagnostic challenges
The clinical presentation of AHO complicated by DVT is often severe, with rapid onset of pain, fever, and complete loss of limb function. Local signs such as erythema, swelling, and warmth may extend beyond the segment of bone involved [16,17]. However, these symptoms are non-specific and can be attributed to either infection or thrombosis. Features more specific to DVT, such as shiny skin, dilated superficial veins, or calf tenderness, may be subtle or masked by osteomyelitis-related inflammation.
Color Doppler ultrasonography remains the standard first-line imaging modality for diagnosing DVT [13], but it does not evaluate bone or deep soft-tissue involvement, potentially missing underlying osteomyelitis. Conversely, MRI is highly sensitive for detecting bone infection and related abscesses but does not reliably identify intravascular thrombi. Therefore, a combined imaging approach is essential in high-risk pediatric musculoskeletal infections, especially when fever and swelling persist despite appropriate antibiotics [8,10].
Implications from our series
All three patients in our series presented with overlapping features of AHO and DVT, and all infections involved the femur. Each case required surgical drainage of an associated abscess and decompression of the affected bone, combined with targeted MRSA therapy and anticoagulation. The outcomes were uniformly favorable, with complete functional recovery and no recurrence at follow-up (10–12 months).
Our findings reinforce prior observations [16,17] that:
- DVT in pediatric osteomyelitis is typically located adjacent to the infected bone
- MRSA is the predominant pathogen
- Early surgical intervention combined with anticoagulation improves outcomes.
Clinical recommendations
Pediatric patients presenting with acute femoral osteomyelitis, particularly those with MRSA infection, severe inflammatory responses, or a history of recent trauma, should undergo early Doppler USG screening for DVT. Persistent fever despite antibiotics should prompt an MRI to assess for abscess formation. Timely recognition of this dual pathology enables prompt initiation of antibiotics, anticoagulation, and surgical drainage, thereby reducing the risk of life-threatening complications such as SPE.
Limitations
This report has several limitations inherent to its case series design. The small sample size (n = 3) and single-center, retrospective nature limit generalizability and may introduce selection bias toward more severe MRSA-associated infections. No standardized diagnostic or anticoagulation protocol was applied, and imaging was clinician-directed rather than protocol-driven. We did not perform routine thrombophilia screening, nor did we use validated functional outcome scores for post-thrombotic syndrome or limb function. Long-term follow-up beyond 12 months for late sequelae such as chronic post-thrombotic venous insufficiency was not available. Causation between AOM and DVT cannot be definitively established from this descriptive series; however, the consistent anatomical contiguity between the infected bone and adjacent thrombosed veins supports a pathogenic association rather than coincidence.
Although rare, the coexistence of AOM and DVT in children can be life-threatening. Recognition of one condition should prompt evaluation for the other, given their overlapping clinical features. Early, accurate diagnosis supported by appropriate imaging and timely initiation of antibiotics, anticoagulation, and surgical intervention are critical for optimal outcomes. Ongoing reassessment is essential to detect disease progression or complications.
In pediatric patients with acute osteomyelitis, particularly involving the femur, clinicians should maintain a high index of suspicion for the possibility of concurrent DVT. A thorough evaluation, including targeted imaging, can prevent missed diagnoses and avert serious complications.
References
- 1. Woods CR, Bradley JS, Chatterjee A, Copley LA, Robinson J, Kronman MP, et al. Clinical practice guideline by the pediatric infectious diseases society and the infectious diseases society of America: 2021 Guideline on diagnosis and management of acute hematogenous osteomyelitis in pediatrics. J Pediatric Infect Dis Soc 2021;10:801-44. [Google Scholar] [PubMed]
- 2. Kulkarni SL, Mannual S, Patil N, Daragad M. Study to evaluate the role of surgical management in acute osteomyelities in children. Indian J Health Sci Biomed Res 2022;15:26-33. [Google Scholar] [PubMed]
- 3. Clark DJ. Venous thromboembolism in paediatric practice. Pediatric Anesth 1999;9:475-84. [Google Scholar] [PubMed]
- 4. Walsh S, Phillips F. Deep vein thrombosis associated with pediatric musculoskeletal sepsis. J Pediatric Orthop 2002;22:329-32. [Google Scholar] [PubMed]
- 5. Monagle P, Cuello CA, Augustine C, Bonduel M, Brandão LR, Capman T, et al. American society of hematology 2018 guidelines for management of venous thromboembolism: Treatment of pediatric venous thromboembolism. Blood Adv 2018;2:3292-316. [Google Scholar] [PubMed]
- 6. Lassandro G, Palmieri VV, Palladino V, Amoruso A, Faienza MF, Giordano P. Venous thromboembolism in children: From diagnosis to management. Int J Environ Res Public Health 2020;17:4993. [Google Scholar] [PubMed]
- 7. Vander Have KL, Karmazyn B, Verma M, Caird MS, Hensinger RN, Farley FA, et al. Community-associated methicillin-resistant Staphylococcus aureus in acute musculoskeletal infection in children: A game changer. J Pediatr Orthop 2009;29:927-31. [Google Scholar] [PubMed]
- 8. LePage AA, Hess EP, Schears RM. Septic thrombophlebitis with acute osteomyelitis in adolescent children: A report of two cases and review of the literature. Int J Emerg Med 2008;1:155-9. [Google Scholar] [PubMed]
- 9. Horvath FL, Brodeur AE, Cherry JD. Deep thrombophlebitis associated with acute osteomyelitis. J Pediatr 1971;79:815-8. [Google Scholar] [PubMed]
- 10. Jupiter JB, Ehrlich MG, Novelline RA, Leeds HC, Kiam D. The association of septic thrombophlebitis with subperiosteal abscesses in children. J Pediatr 1982;101:690-4. [Google Scholar] [PubMed]
- 11. Lin MY, Rezai K, Schwartz DN. Septic pulmonary emboli and bacteremia associated with deep tissue infections caused by community-acquired methicillin-resistant Staphylococcus aureus. J Clin Microbiol 2008;46:1553-5. [Google Scholar] [PubMed]
- 12. Lew DP, Waldvogel FA. Osteomyelitis. Lancet 2004;364:369-79. [Google Scholar] [PubMed]
- 13. He Y, Liu S, Su Y. Risk factors of deep vein thrombosis in children with osteomyelitis. Ann Med 2023;55:2249011. [Google Scholar] [PubMed]
- 14. Calderon ML, Salas RM. Deep venous thrombosis associated with acute osteomyelitis. Salus 2017;21:30-6. [Google Scholar] [PubMed]
- 15. Stein PD, Kayali F, Olson RE. Incidence of venous thromboembolism in infants and children: Data from the National hospital discharge survey. J Pediatr 2004;145:563-5. [Google Scholar] [PubMed]
- 16. Hollmig ST, Copley LA, Browne RH, Grande LM, Wilson PL. Deep venous thrombosis associated with osteomyelitis in children. J Bone Joint Surg Am 2007;89:1517-23. [Google Scholar] [PubMed]
- 17. Gonzalez BE, Teruya J, Mahoney DH Jr., Hulten KG, Edwards R, Lamberth LB, et al. Venous thrombosis associated with Staphylococcal osteomyelitis in children. Pediatrics 2006;117:1673-9. [Google Scholar] [PubMed]
- 18. Gorenstein A, Gross E, Houri S, Gewirts G, Katz S. The pivotal role of deep vein thrombophlebitis in the development of acute disseminated Staphylococcal disease in children. Pediatrics 2000;106:E87. [Google Scholar] [PubMed]
- 19. Gillet Y, Dohin B, Dumitrescu O, Lina G, Vandenesch F, Étienne JP, et al. Infections ostéoarticulaires à Staphylocoques dorés sécréteurs de la leucocidine de Panton-Valentine. Arch Pediatr 2007;14 Suppl 1:102-7. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult
July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult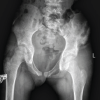 May 1, 2026 Methicillin-Resistant Staphylococcus aureus Iliac Osteomyelitis with Cortical Breach Mimicking Septic Arthritis of the Hip in a Child: A Diagnostic Pitfall
May 1, 2026 Methicillin-Resistant Staphylococcus aureus Iliac Osteomyelitis with Cortical Breach Mimicking Septic Arthritis of the Hip in a Child: A Diagnostic Pitfall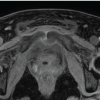 February 1, 2026 When MRSA Misleads: Tuberculous Osteomyelitis of the Anterior Pelvic Bones
February 1, 2026 When MRSA Misleads: Tuberculous Osteomyelitis of the Anterior Pelvic Bones August 1, 2025 An Unusual Presentation of Delayed Hemarthrosis Following Total Knee Arthroplasty: A Case Report
August 1, 2025 An Unusual Presentation of Delayed Hemarthrosis Following Total Knee Arthroplasty: A Case Report