
In patients presenting with chronic wrist swelling and flexor tendon dysfunction, the radiological appearance of “rice bodies” is highly predictive of tubercular compound palmar ganglion; prompt surgical excision combined with antitubercular chemotherapy is essential to restore hand function and prevent complications like tendon rupture.
Dr. Nikhil Agrawal, Department of Orthopaedics, All India Institute of Medical Sciences, New Delhi, India. E-mail: nikhilagrawalwork1503@gmail.com
Abstract
Introduction: Tubercular tenosynovitis involving the flexor compartments of the hand, specifically manifesting as a compound palmar ganglion, is a rare form of extrapulmonary tuberculosis (TB). It constitutes a small fraction of musculoskeletal TB cases and is frequently misdiagnosed as rheumatoid arthritis or non-specific synovitis due to its insidious onset and lack of systemic symptoms. This case report is important as it highlights a massive presentation of this condition that persisted for years due to delayed diagnosis. It underscores the necessity of considering a tubercular etiology in chronic hand swellings to prevent severe complications such as tendon rupture and permanent hand dysfunction. While this report describes a single patient, it aligns with the existing rare literature to provide a clear management framework for surgeons in endemic regions.
Case Report: A 45-year-old female of Indian ethnicity presented with a 3-year history of gradually progressive swelling over her left hand and little finger, accompanied by an inability to flex the wrist and fifth digit. She had previously received conservative symptomatic treatment without relief. Clinical examination revealed a non-tender, spongy swelling over the hypothenar eminence and wrist. Magnetic resonance imaging (MRI) revealed extensive tenosynovitis of the fifth flexor compartment containing numerous “rice bodies,” which are characteristic of chronic inflammation. The patient underwent open surgical excision of the mass. Histopathological examination of the excised tissue confirmed the diagnosis by revealing caseating granulomas and Langhans giant cells. She was subsequently treated with a 12-month course of antitubercular chemotherapy (ATT) and achieved full functional recovery without recurrence. Given the rapid clinical improvement, standard first-line chemotherapy was used successfully as a surrogate for drug sensitivity.
Conclusion: This case illustrates that compound palmar ganglion should remain a high-priority differential diagnosis for chronic, unexplained wrist swelling and flexor dysfunction, particularly in endemic regions. The clinical impact of this report lies in reinforcing the diagnostic utility of MRI in identifying “rice bodies” and the absolute necessity of histopathological confirmation. Early surgical excision combined with prolonged ATT is the definitive management strategy to restore hand function and prevent the significant morbidity associated with delayed diagnosis.
Keywords: Tubercular tenosynovitis, compound palmar ganglion, rice bodies, flexor tendon dysfunction, extrapulmonary tuberculosis.
Despite the availability of effective chemotherapy, tuberculosis (TB) continues to be a significant public health challenge, particularly in developing nations. While the spine and large weight-bearing joints are the most common sites for musculoskeletal involvement, TB of the tendon sheaths is a rare entity, accounting for approximately 5% of osteoarticular TB cases [1]. The term “compound palmar ganglion” refers specifically to chronic tuberculous tenosynovitis of the common flexor sheath (ulnar bursa). Anatomically, this bursa extends from the proximal wrist crease to the mid-palm. When infected, the sheath becomes distended with fluid and granulomatous tissue, creating a dumbbell-shaped swelling constrained by the flexor retinaculum. This unique anatomy allows fluid to be displaced between the palmar and volar aspects of the wrist – a pathognomonic clinical sign known as “cross-fluctuation” [2]. Pathologically, the condition is characterized by the exudation of fluid and the formation of “rice bodies”—small, fibrin-derived pellets that are highly suggestive of tubercular etiology, although they can occasionally be seen in rheumatoid arthritis (RA) [3]. Due to its insidious progression and the frequent absence of constitutional symptoms such as fever, early diagnosis is challenging. It is often mistaken for entrapment neuropathies, rheumatoid tenosynovitis, or non-specific soft-tissue tumors. Delayed treatment can lead to devastating complications, including spontaneous tendon rupture, median nerve compression (carpal tunnel syndrome), and permanent joint stiffness [4]. Therefore, a high index of suspicion is required in endemic areas. While magnetic resonance imaging (MRI) provides excellent soft-tissue delineation, the definitive diagnosis relies on histopathological demonstration of caseating granulomas.
A 45-year-old female presented to our outpatient department with a primary complaint of gradually progressive swelling over the left hand and little finger, persisting for over 3 years. The swelling was associated with a significant inability to flex the left wrist and the little finger. The patient reported a history of dull, aching pain and tenderness over the affected area. Before visiting our institution, she had sought consultation from local practitioners and was managed conservatively with oral analgesics and anti-inflammatory medications; however, she experienced no symptomatic relief, and the swelling continued to increase in size. There was no history of trauma, fever, weight loss, or respiratory symptoms suggestive of systemic infection. On physical examination, a diffuse, soft, spongy swelling was noted over the volar aspect of the left wrist, extending distally toward the hypothenar eminence and the proximal phalanx of the fifth digit (Fig. 1).

Figure 1: Pre-operative clinical photograph showing diffuse, spongy
swelling over the volar aspect of the left wrist and hypothenar eminence.
The swelling was tender on palpation. “Cross-fluctuation” was elicited across the flexor retinaculum, suggestive of a compound palmar ganglion. Active and passive flexion of the little finger and wrist were restricted and painful. Neurological examination revealed no sensory deficits in the distribution of the median or ulnar nerves, and vascular status was intact. Laboratory investigations revealed elevated inflammatory markers, with a raised erythrocyte sedimentation rate and C-reactive protein. Specific serological tests for rheumatoid factor and anti-cyclic citrullinated peptide were negative, ruling out rheumatoid etiology. Plain radiographs of the left hand and wrist showed soft-tissue swelling involving the fifth finger and extending up to the wrist, without frank bony destruction. MRI was performed for further evaluation. MRI sequences revealed extensive tenosynovitis involving the fifth flexor compartment. A distinct finding was the presence of multiple small, hypointense, rounded signal voids within the hyperintense fluid on T2-weighted images, characteristic of “rice bodies” (Fig. 2).
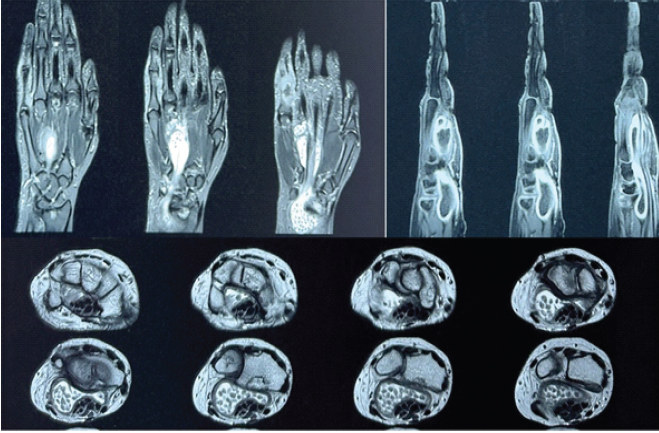
Figure 2: Magnetic resonance imaging (MRI) of the left wrist and hand showing – coronal short tau inversion recovery
sequences reveal extensive tenosynovitis involving the 5th flexor compartment with soft tissue thickening extending to
the distal forearm. Sagittal sections demonstrating significant tendon sheath expansion and erosions near the carpal
bones. Axial MRI sections showing fluid distension within the flexor tendon sheaths containing multiple small, rounded
signal voids characteristic of “rice bodies.”
Soft-tissue thickening extended to the distal forearm. In addition, multiple erosions were noted along the radiocarpal, intercarpal, and carpometacarpal joints. Based on the clinical and radiological features, a provisional diagnosis of tubercular compound palmar ganglion was made. The patient was scheduled for surgical intervention. Under brachial block anesthesia, an open excisional biopsy and synovectomy were performed. A longitudinal incision was made over the palmar aspect of the wrist, extending to the proximal phalanx of the fifth finger. Intraoperatively, a large, lobulated, encapsulated synovial mass measuring approximately 10 cm × 3 cm × 1 cm was identified (Fig. 3).
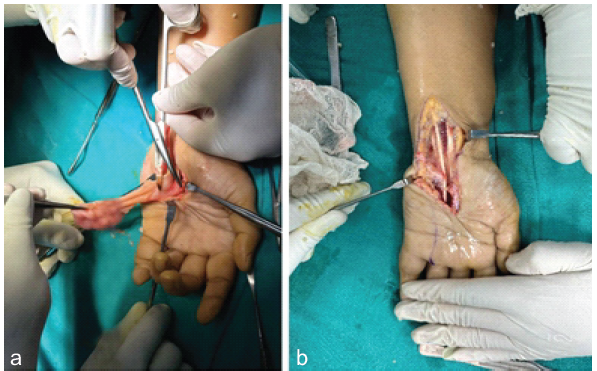
Figure 3: (a and b) Intraoperative photograph showing the retrieval of a large, lobulated synovial mass
from the flexor sheath.
Upon releasing the flexor retinaculum, the flexor tendons were found to be encased in thickened synovium containing frank purulent fluid and numerous glistening white “rice bodies” (Fig. 4).
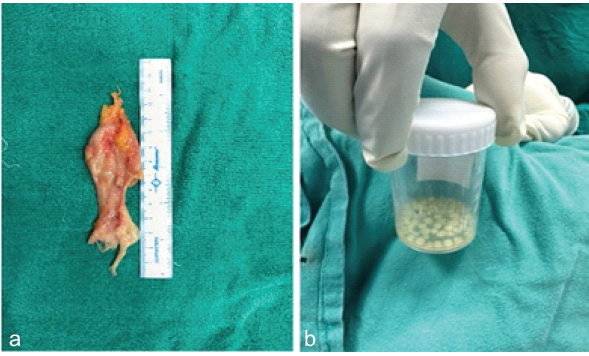
Figure 4: (a and b) Gross specimen photograph showing the excised mass and the collection of numerous white “rice bodies.”
A thorough debulking was performed, removing the thickened synovium and rice bodies while preserving the integrity of the flexor tendons and neurovascular structures. The excised tissue was submitted for histopathological examination. Microscopic analysis revealed fibrocollagenous tissue with multiple granulomas composed of multinucleated giant cells (Langhans type), epithelioid cells, and lymphocytes surrounding areas of central caseous necrosis (Fig. 5).
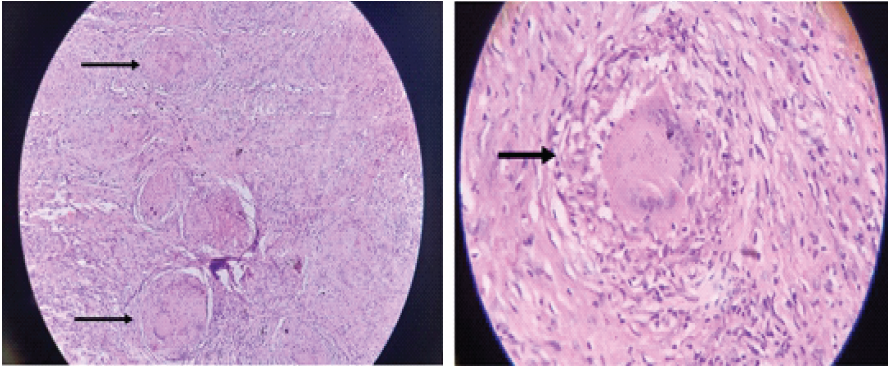
Figure 5: Photomicrograph (hematoxylin and eosin stain) showing a classic granuloma with multinucleated Langhans giant cells, epithelioid cells, and central caseous necrosis, confirming tuberculosis. (a) Low power microscopic picture showing – Fibrocollagenous tissue having multiple granulomas. (b) High power
microscopic picture showing granuloma consisting of multinucleated giant cells, Langhans giant cells, epithelioid cells, fibroblasts, lymphocytes, and central caseous necrosis.
These findings confirmed the diagnosis of tubercular tenosynovitis. Postoperatively, the patient was started on a standard antitubercular therapy (ATT) regimen comprising isoniazid, rifampicin, pyrazinamide, and ethambutol for the initial intensive phase, followed by a continuation phase for a total duration of 12 months. Physiotherapy was initiated early to restore hand function. As the patient showed immediate clinical resolution of swelling and pain within the intensive phase, clinical response was utilized as a surrogate for drug susceptibility testing, which is often reserved for non-responsive cases in our setting. At the 12-month follow-up, the patient was asymptomatic with complete resolution of swelling and restoration of wrist and finger flexion. Objectively, the wrist achieved 60° of flexion and 70° of extension, with total active motion of the fifth digit returning to 270°. No recurrence of the lesion was observed.
Tubercular involvement of the musculoskeletal system is relatively rare, accounting for 1–3% of all TB cases. Within this subset, isolated tenosynovitis of the hand is an even rarer entity, estimated to constitute less than 5% of musculoskeletal TB [1]. The condition was first described by Acrel in 1777, and later, Kanavel defined the detailed anatomy of the flexor tendon sheaths, which is crucial for understanding the pathology of “compound palmar ganglion” [5]. The term “compound palmar ganglion” refers to the infection of the common flexor sheath (ulnar bursa). Anatomically, this bursa extends from the proximal wrist crease to the mid-palm. When infected, the sheath becomes distended, but the unyielding transverse carpal ligament (flexor retinaculum) constricts the swelling in the middle, resulting in a characteristic “dumbbell” or “hourglass” configuration. This allows for the pathognomonic sign of “cross-fluctuation,” where pressure on the palmar swelling produces prominence proximal to the wrist, and vice versa [2]. The diagnosis of tubercular tenosynovitis is notoriously difficult and often delayed, as observed in our case, where the patient suffered for 3 years. While microbiological culture is ideal, musculoskeletal TB is typically paucibacillary; thus, histopathological demonstration of caseating granulomas remains the definitive diagnostic gold standard. The clinical presentation mimics RA, giant cell tumors, fungal tenosynovitis, and atypical mycobacterial infections. Fungal etiology and sarcoidosis were ruled out based on the abundance of rice bodies and the presence of caseous necrosis rather than non-caseating granulomas. “Rice bodies” are a key diagnostic differentiator in our case. First described by Riseborough, these are pellets of fibrin, collagen, and amorphous material derived from infarcted synovial villi [6]. While rice bodies are classically associated with TB, they can also be found in RA and seronegative spondyloarthropathies [7]. However, their abundance and the specific clinical context in endemic regions strongly point toward TB. MRI is the gold standard for pre-operative assessment [8]. On T2-weighted images, rice bodies appear as multiple, small, hypointense nodules within hyperintense synovial fluid, a finding clearly demonstrated in this patient [9]. This “millet seed” appearance is invaluable for surgical planning. Management of this condition has been a subject of debate. While antitubercular chemotherapy (ATT) is the cornerstone of treatment, medical management alone is often insufficient for advanced cases with extensive caseation and rice body formation, as the drugs penetrate the thickened fibrous sac poorly [10]. Furthermore, the mechanical bulk of the lesion can cause median nerve compression (Carpal Tunnel Syndrome) or ischemic necrosis of the tendons. Therefore, a combined approach – extensive surgical debridement (synovectomy) to reduce the bacterial load and remove mechanical irritants, followed by a full course of chemotherapy – is widely accepted as the standard of care [1,3]. In the present case, the complete excision of the mass followed by 12 months of ATT resulted in excellent functional recovery, supporting the efficacy of this combined modality. Repeat post-operative MRI was omitted due to complete clinical resolution and cost constraints prevalent in endemic regions. Tubercular compound palmar ganglion is an elusive diagnosis that requires a high index of suspicion in patients presenting with chronic, slowly progressive wrist swelling. It is easy to diagnose but often neglected, leading to carpal tunnel syndrome [11]. The presence of “rice bodies” on MRI is a strong predictor of tubercular etiology. Histopathological confirmation is mandatory to distinguish this treatable infectious condition from inflammatory or neoplastic mimics. Early, aggressive surgical synovectomy combined with prolonged ATT prevents devastating complications such as tendon rupture and restores hand function.
This case report highlights a rare presentation of extrapulmonary TB manifesting as a massive compound palmar ganglion. It serves as a critical reminder that despite the declining global incidence of TB, musculoskeletal involvement remains a significant diagnostic challenge, particularly in its non-osseous forms. The case reinforces the diagnostic value of MRI, specifically the identification of “rice bodies,” which should trigger an immediate suspicion of tubercular etiology even in the absence of systemic symptoms. While this single case has limited external validity, it demonstrates a successful management protocol of aggressive surgical debridement combined with a prolonged, 12-month course of ATT. This mirrors findings in other documented rare cases and yields excellent functional outcomes, thereby offering a clear management framework for orthopedic surgeons encountering similar complex presentations.
Chronic, progressive wrist swelling with flexor dysfunction should not be dismissively treated as simple inflammation or a common ganglion cyst, especially in TB-endemic regions. The presence of “rice bodies” on MRI is a hallmark warning sign that demands investigation for TB. This case underscores that relying solely on conservative management or medical therapy for large, space-occupying lesions is often futile. The key to preventing permanent hand deformity lies in early recognition, definitive histopathological confirmation, and the synergistic use of surgical excision and antitubercular therapy.
References
- 1. Tuli SM. General principles of osteoarticular tuberculosis. Clin Orthop Relat Res 2002;398:11-9. [Google Scholar] [PubMed]
- 2. Kotwal PP, Khan SA. Tuberculosis of the hand: Clinical presentation and functional outcome in 32 patients. J Bone Joint Surg Br 2009;91:1054-7. [Google Scholar] [PubMed]
- 3. Regnard PJ, Barry P, Isselin J. Mycobacterial tenosynovitis of the flexor tendons of the hand. A report of five cases. J Hand Surg Br 1996;21:351-4. [Google Scholar] [PubMed]
- 4. Bush DC, Schneider LH. Tuberculosis of the hand and wrist. J Hand Surg Am 1984;9:391-8. [Google Scholar] [PubMed]
- 5. Ahmad J, Kumar Shrivastava V, Khanna M, Ayaz A. Tubercular compound palmar ganglion – A review. Int J Orthop Rheumatol 2019;5:22-5. [Google Scholar] [PubMed]
- 6. Woon CY, Phoon ES, Lee JY, Puhaindran ME, Peng YP, Teoh LC. Rice bodies, millet seeds, and melon seeds in tuberculous tenosynovitis of the hand and wrist. Ann Plast Surg 2011;66:610-7. [Google Scholar] [PubMed]
- 7. Gillijns M, Vandesande W. Rice bodies in the wrist. Mod Rheumatol Case Rep 2022;6:150-4. [Google Scholar] [PubMed]
- 8. Hong SH, Kim SM, Ahn JM, Chung HW, Shin MJ, Kang HS. Tuberculous versus pyogenic arthritis: MR imaging evaluation. Radiology 2001;218:848-53. [Google Scholar] [PubMed]
- 9. Sueyoshi E, Uetani M, Hayashi K, Kohzaki S. Tuberculous tenosynovitis of the wrist: MRI findings in three patients. Skeletal Radiol 1996;25:569-72. [Google Scholar] [PubMed]
- 10. Hogan JI, Hurtado RM, Nelson SB. Mycobacterial musculoskeletal infections. Infect Dis Clin North Am 2017;31:369-82. [Google Scholar] [PubMed]
- 11. Panigrahi S, Jain M, Panda R, Karaniveed Puthiyapura L. Patient with tuberculous flexor tenosynovitis of the hand. BMJ Case Rep 2021;14:e243091. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Tuberculous Synovitis of the Elbow Presenting with Multiple Rice Bodies: A Rare Case Report
March 1, 2026 Tuberculous Synovitis of the Elbow Presenting with Multiple Rice Bodies: A Rare Case Report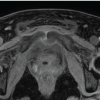 February 1, 2026 When MRSA Misleads: Tuberculous Osteomyelitis of the Anterior Pelvic Bones
February 1, 2026 When MRSA Misleads: Tuberculous Osteomyelitis of the Anterior Pelvic Bones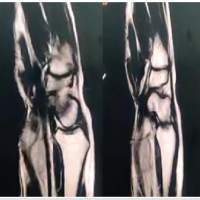 July 1, 2025 Tubercular Palmar Ganglion Presenting as a Severe Carpal Tunnel Syndrome – A Case Report
July 1, 2025 Tubercular Palmar Ganglion Presenting as a Severe Carpal Tunnel Syndrome – A Case Report November 10, 2022 Lactococcus garvieae Periprosthetic Joint Infection in a Cattle Rancher with a Total Knee Arthroplasty: A Novel Reservoir Transmission
November 10, 2022 Lactococcus garvieae Periprosthetic Joint Infection in a Cattle Rancher with a Total Knee Arthroplasty: A Novel Reservoir Transmission